
Abstract
BACKGROUND AND PURPOSE: Focal high signal intensity in the splenium of the corpus callosum on fluid-attenuated inversion-recovery (FLAIR) images is generally considered an abnormal MR finding. We identified high signal intensity in the splenium on FLAIR images in patients of advanced age with otherwise normal images and in patients who had received brain radiation therapy. We undertook an investigation to determine the frequency of this finding in these patient groups.
METHODS: We reviewed the FLAIR images and medical records of 67 patients (group 1) imaged for suspicion of CNS disease and of 18 consecutive patients (group 2) with history of brain radiation therapy. All FLAIR images were evaluated for focal signal intensity abnormalities in the splenium and for diffuse white matter abnormalities. Also, autopsy specimens from two cases not part of either study group were examined.
RESULTS: Among the initial 67 patients in group 1, focal high signal intensity in the splenium was associated with aging, radiation therapy, and white matter changes. Focal high signal intensity in the splenium was evident on FLAIR images in 16 of the 18 patients in the post-radiation therapy group. Histologic examination of the splenium in one autopsy case with a history of chest and neck radiation therapy demonstrated isomorphic gliosis.
CONCLUSION: High signal intensity in the splenium of the corpus callosum on FLAIR images is a common finding after brain radiation therapy and can be seen with aging. The radiologist should be aware of this common finding and not mistake it for more commonly recognized causes of splenial lesions.
Previous reports suggest that focal lesions in the splenium of the corpus callosum are seen almost exclusively in the setting of diseases such as multiple sclerosis, direct tumor involvement, or trauma (1). However, during routine MR imaging with the fluid-attenuated inversion-recovery (FLAIR) technique, focal lesions in the anterior subependymal region of the splenium of the corpus callosum were noted in several patients of advanced age. The lesions appeared unrelated to current symptoms, and clinical history revealed no clear explanation for the abnormal signal intensity on FLAIR images. Similar abnormal signal intensity was noted in the splenium of patients who had undergone prior brain radiation therapy for primary brain neoplasm, with no evidence of direct tumor involvement. Thus, we hypothesized that focal abnormal signal intensity in the undersurface of the splenium on FLAIR images is a common finding in patients of advanced age and in those who have undergone brain radiation therapy and correlates with high signal intensity in the periventricular white matter on FLAIR images. We undertook an investigation to determine the frequency of this finding in these patient groups. We also reviewed the findings at autopsy of two patients of advanced age, both of whom had abnormal signal intensity in the splenium on FLAIR images, to better understand the pathogenesis of this finding.
Methods
Patients
MR images obtained in two groups of patients were evaluated. The initial 78 patients studied (group 1) were imaged as part of their clinical evaluation for suspected CNS disease. A retrospective review of medical records was performed for those cases with high signal intensity in the corpus callosum on FLAIR images. Eleven patients were excluded because of clinical or radiographic evidence suggesting demyelinating disease or direct corpus involvement with tumor. Of the remaining 67 patients (27 male, 40 female patients; age range, 3–93 years; mean age, 50.6 +/− 23.5 years [SD]), 13 had undergone prior brain radiation therapy. The distribution of the neoplasms was as follows: two anaplastic astrocytomas, four metastatic lesions to brain, one medulloblastoma, one pituitary tumor, two oligodendrogliomas, and one acoustic neuroma, and two patients had a history of neck radiation therapy.
We then studied the images of 26 consecutive patients (group 2) with biopsy-proved primary brain neoplasm and a history of radiation therapy. A review of the medical records was performed, and patients were included in the study if axial FLAIR imaging of the brain was performed within 1 year following the completion of therapy. This time frame was selected to provide close temporal correlation of imaging with therapy. Eight patients were excluded owing to clinical or radiographic evidence suggesting demyelinating disease or direct corpus involvement with tumor, or for age older than 65 years. This age cutoff was established to limit the confounding effects of age-related lesions in the splenium documented in group 1. Of the remaining 18 patients (12 male, six female patients; age range, 5–64 years; mean age, 47.5 +/− 13.9 years), the distribution of supratentorial neoplasms was as follows: six glioblastoma multiforme, two astrocytomas, two anaplastic astrocytomas, five oligodendrogliomas, and one mixed glioma, and two patients with infratentorial lesions had medulloblastoma and a brain-stem glioma, respectively. All patients received between 5400 and 6000 cGy of total brain radiation in fractionated dosing. Pretherapy FLAIR images were available for 10 of the 18 patients in group 2; these images were obtained a mean of 1.6 +/− 1.4 months (range, 0.8–7 months) before the first day of radiation therapy. Posttherapy FLAIR imaging was performed in all 18 patients a mean of 7.2 +/− 2.8 months (range, 3.2–11.8 months) following the last day of radiation therapy.
To further investigate the cause of signal intensity changes in the splenium on FLAIR images, postmortem pathologic specimens were obtained in two cases in which previous MR imaging had been performed; however, neither case was part of either study group. In both cases, increased signal intensity in the anterior subependymal region of the splenium was noted on axial FLAIR images. The first case was a 63-year-old man with a history of Hodgkin disease treated with chemotherapy as well as chest and neck radiation therapy 31 years prior. Autopsy revealed diffuse Hodgkin lymphoma with liver metastases but no brain metastasis. The second case was an 80-year-old man with end-stage Parkinson disease who died of pneumonia. At the time of autopsy, the MR findings were known, and the splenium was sectioned in the sagittal plane to better localize the finding at microscopy because no gross lesion was evident. The specimens were stained and evaluated with light microscopy.
Imaging
MR imaging was performed with a 1.5-T superconducting magnet (Signa; GE Medical Systems, Milwaukee, WI). Parameters for the fast spin-echo FLAIR technique were 10,000/156/1 or 10,002/166/1 (TR/TE/excitations), inversion time of 2200, 256 × 192 matrix with a 20-cm field of view, echo train length of 12, and 5-mm-thick sections with a 2-mm intersection gap. Imaging times were less than 3 minutes. All images were obtained in the course of the patient’s routine clinical examination and not as part of a dedicated research protocol. Both sagittal and axial FLAIR images were obtained in the group 1 patients, to better define the location of the splenial lesion. Axial FLAIR images were obtained in all group 2 patients, and in a subset of 12 patients, sagittal FLAIR images were obtained as well.
Evaluation of signal intensity in the splenium of the corpus callosum on FLAIR images for group 1 was scored on the basis of the sagittal MR examination. The images were scored by one of the authors, a neuroradiologist (A.C.M.) with a certificate of added qualification (CAQ). The radiologist was blinded to the patient’s clinical history. For group 2, pre- and posttherapy images were evaluated independently. The images in group 2 were reviewed by two of the authors, a CAQ neuroradiologist (A.C.M.) and a third year radiology resident (J.S.P.). Any discrepancies were resolved by consensus. The signal intensity in the splenium was compared visually with the signal intensity in the remainder of the corpus callosum. Grade 0 indicated that no abnormal signal intensity was observed in the splenium; grade 1 reflected linear high signal intensity in the anterior subependymal region of the splenium; and grade 2 was used for nodular lesions that involved more than half the thickness of the splenium or linear lesions that involved more than half the anteroposterior dimension of the corpus callosum. In addition, diffuse white matter disease was graded. Previous systems have been used for grading white matter changes in the setting of radiation therapy (2). However, we chose a simplified version to decrease subjectivity, a particular problem in the intermediate grades. Grade 0 indicated no signal intensity change relative to normal white matter; grade 1 indicated focal white matter involvement; and grade 2 indicated confluent periventricular white matter high signal intensity abnormalities on FLAIR images. Correlation, regression, and nonparametric statistics were then used as appropriate to address the study hypothesis.
Results
Group 1
Among the initial 67 patients who were imaged as part of their clinical evaluation for suspected CNS disease, 32 patients demonstrated increased signal intensity in the splenium of the corpus callosum on FLAIR images (Fig 1). Eleven of these patients with abnormal signal intensity underwent prior brain radiation therapy. In the sample of all 67 patients, age, history of radiation therapy, and white matter signal intensity abnormality grade were all significant predictors of splenial lesion grade on simple correlational analyses (all P < .001). Regression analysis confirmed that history of radiation therapy and white matter lesion grade each accounted for a significant proportion of variance in splenial lesion grade (P < .001), whereas the effect of age dropped to a nonsignificant level (P > .05) when the effects of the other two variables were entered into the equation. The sample was divided into two subsets for all subsequent analyses: 54 patients with no history of radiation therapy and 13 patients with a history of brain and neck radiation therapy.

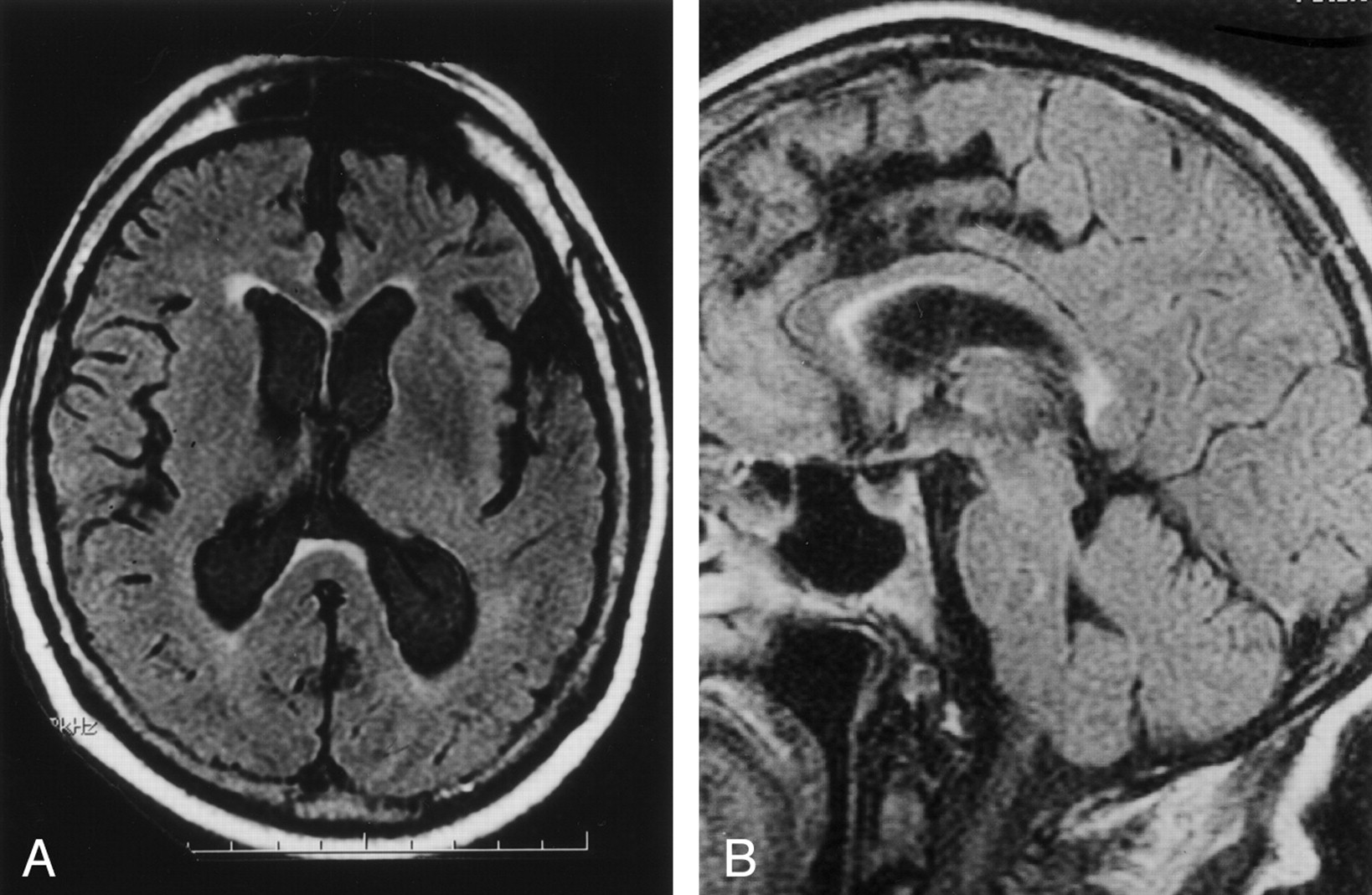
Case of a 67-year-old patient imaged to rule out aneurysm.
A, Axial and B, sagittal FLAIR MR images (10,000/156/1) show high signal intensity in the anterior subependymal region of the splenium of the corpus callosum, involving more than half the thickness (grade 2).
The first subset, 54 patients evaluated for suspected CNS disease, was composed of 34 female and 20 male patients with a mean age of 50.4 ± 23.5 years (range, 3–93 years). Of this subset, 19 (35%) demonstrated increased signal intensity in the splenium of the corpus callosum. This signal intensity abnormality was most typically seen involving the anterior subependymal region of the splenium on axial and sagittal FLAIR images (Fig 1). Within this group, splenial abnormality, white matter abnormality (each coded as present or absent), and age all significantly and positively correlated with each other (all P < .001). Given the dichotomous nature of the variables involved, a distribution-free analysis was used to confirm the positive relation between the presence of splenial lesions and white matter abnormalities (χ24 = 51.8, P < .001). To provide a preliminary evaluation of the relative contribution of age and white matter abnormality to the prediction of splenial lesions, a stepwise regression analysis was conducted, with splenial abnormality as the dependent variable and white matter abnormality and age as independent variables. Results indicated a significant relation between the presence of white matter abnormalities and splenial abnormalities (R2adj = 0.74, P < .001). After accounting for variance in splenial status associated with white matter abnormality, age did not enter into the equation. To further explore the relation between white matter and splenial abnormalities, a count was taken of the number of cases in which splenial lesion grade was greater than, equal to, or less than white matter lesion grade. Although the ratings were made independently, most cases (n = 45 [83%]) showed the same lesion grade for both white matter and splenium. Only nine cases showed a mismatch between splenial and white matter lesion grades, most of which (n = 8) involved a higher grade for white matter than for splenial lesion.
The 13 patients with a history of radiation therapy were then analyzed. This subset was composed of six female and seven male patients with a mean age of 51.5 ± 24.7 years (range, 5–85 years). This group did not significantly differ from the first group in age or sex (both P > .05). In this subset, all patients had splenial lesions, which prevented use of statistical analyses involving the presence or absence of splenial lesions. There was no significant correlation between age and the presence or absence of white matter abnormalities in this group (P > .05), likely at least partly due to the small sample size. However, an analysis of the frequency with which splenial lesion grade was greater than, equal to, or less than white matter lesion grade again showed that most cases (n = 8 [61%]) showed the same lesion grade for each tissue type. Only five patients showed a mismatch between splenial and white matter lesion grade, and in all cases, the splenial grade was higher.
A nonparametric analysis was used to further explore the minority of patients in each group who showed a mismatch in either direction between the grade of splenial lesion and the grade of white matter lesion. Patients with a higher grade of splenial than white matter lesion had a history of radiation therapy (five of five cases), whereas patients with a higher grade of white matter than splenial lesion had generally not received radiation (eight of nine cases; χ21 = 10.4, P = .001). The presence of higher splenial or higher white matter lesion grade was not significantly related to sex of the patients (both P < .05). However, patients with higher splenial than white matter lesion grades, all of whom had received radiation, were significantly younger than those with higher white matter lesion grades (t12 = 2.4, P < .05; mean age 50.0 + 17.3 versus 70.6 + 14.8, respectively).
Group 2
High signal intensity in the splenium of the corpus callosum was evident in 16 (89%) of the 18 posttherapy FLAIR examinations (Table 1). Of these 16 images, all were scored as having grade 2 lesions in the splenium. In those cases in which both axial and sagittal FLAIR images were available, the abnormality was demonstrated along the undersurface of the splenium. Overall, postradiation white matter disease was graded as 0 (no signal intensity change relative to normal white matter) in four of 18 patients and grade 1 (minimal increased signal intensity) in the remaining 14 patients. In patients with both pre- and posttherapy FLAIR images, eight of 10 patients developed the abnormal signal intensity in the splenium of the corpus callosum following radiation therapy (Fig 2). The other two patients demonstrated abnormal signal intensity in the splenium on pre- and posttherapy images. These two patients were the oldest in this group at 62 and 64 years of age.

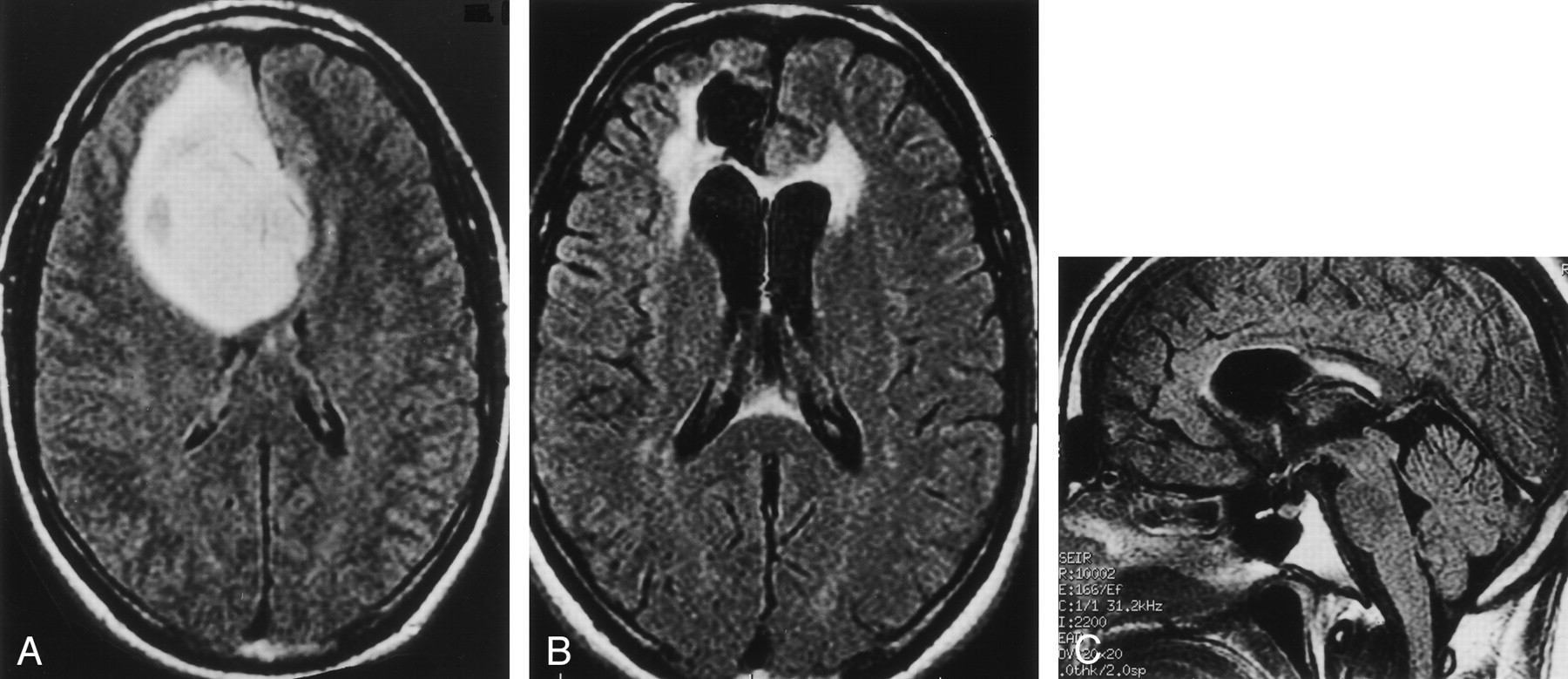
Case of a 32-year-old man (patient 12 in Table) with geminocystic astrocytoma.
A, Axial FLAIR MR image (10,002/166/1) obtained 0.8 months before radiation therapy shows normal signal intensity in the splenium.
B, Axial and C, sagittal FLAIR images (10,002/166/1) obtained 5.8 months after radiation therapy demonstrate a bright focus of abnormal signal intensity in the anterior subependymal region of the splenium of the corpus callosum (grade 2).
Summary of clinical and radiologic findings in the radiation therapy group
Autopsy Specimens
The two autopsy cases demonstrated focal abnormal signal intensity abnormalities in the anterior subependymal region of the splenium (grade 1 lesions) on FLAIR images. Pathologic examination of the undersurface of the splenium in the case of the 63-year-old patient with a history of chest and neck radiation therapy revealed a band of isomorphic gliosis in the predicted location of the splenial lesion identified on FLAIR MR images (Fig 3). The histologic appearance of the anterior subependymal region of the splenium obtained from the 80-year-old patient was normal.

Two autopsy cases.
A, Axial FLAIR (10,000/156/1) image obtained in a 63-year-old man shows grade 1 signal intensity abnormality in the anterior subependymal region of the splenium.
B, Photomicrograph of histologic specimen of the splenium (same patient as in A) demonstrates a band of isomorphic gliosis (hematoxylin and eosin stain; original magnification, x60).
C, Axial FLAIR (10,000/156/1) image obtained in an 80-year-old man shows grade 1 signal intensity abnormality in the anterior subependymal region of the splenium.
D, Photomicrograph of histologic specimen of the splenium (same patient as in C) shows no gliosis (hematoxylin and eosin stain; original magnification, x60).
Discussion
The aging brain demonstrates characteristic morphologic cerebral white matter changes, which are now being detected with advanced MR imaging (3, 4). The term “leukoaraiosis” is commonly used to describe these changes when bilateral and patchy or diffuse hypoattenuation is seen on CT scans or hyperintensity is seen on T2-weighted MR images (5). Leukoaraiosis may demonstrate various morphologic patterns on MR images and can be seen in healthy adult patients, or may be associated with specific attributable neurologic deficits or dementia (6–10). Pathologic correlation has demonstrated that hyperintense periventricular caps and a smooth subependymal halo seen with aging represent demyelination with subependymal gliosis and discontinuity of the ependymal lining, which are nonischemic in nature (11). However, white matter hyperintensities ranging from punctuate to confluent have been demonstrated to reflect small cavitations, tissue loss, and arteriosclerosis corresponding with increasing severity of ischemia (11, 12).
Although there are no previous studies that clearly describe a focal age-related white matter process in the corpus callosum that would explain our findings, there are hints in the literature. A positive relationship between age and callosal T1 relaxation time and a negative relationship between age and callosal area have previously been established (13). The first group of patients we examined demonstrated a clear correlation between abnormal high signal intensity in the splenium and white matter high signal intensity on FLAIR images, most consistent with leukoaraiosis of aging. More sophisticated imaging tools have recently become available to evaluate white matter tracks, perhaps the most promising of which is diffusion tensor imaging, which can quantify the degree of directional freedom of water diffusion within these white matter bundles. In a recent article, Chepuri et al (14) conclude that there is a significant difference between the posterior and anterior corpus callosum with respect to anisotropy. The authors suggest that one contributing factor may be structures within the callosum apart from the axonal fibers. With respect to the effect of radiation on the corpus callosum, Palmer et al (15) conclude that the posterior corpus callosum shows the largest deviation from normal with respect to volume in children treated for posterior fossa tumors after craniospinal radiation therapy. The authors suggest that this finding may be caused by the close proximity of the posterior corpus callosum to the radiation portal.
The autopsy findings in the patients with abnormal signal intensity in the splenium on FLAIR images were of interest with regard to a possible explanation for this lesion. The one patient with histologic changes in the splenium also had a history of radiation therapy. In this case, the findings suggested a slow loss of axons and their associated myelin sheaths from this zone of the posterior corpus callosum. The pathogenesis of these alterations is not evident from the histologic examination, other than to suggest that it was an indolent process and not due to an ischemic infarct. In the autopsy case without a history of radiation, no abnormalities were seen at microscopy, despite similar imaging findings.
There have been many previous reports of lesions limited to the splenium in the absence of tumor or demyelination. Kim et al (16) describe a focal, ovoid lesion of the splenium in six patients, all of whom had been treated with antiepileptic medications. Of some interest is the fact that in two cases they report resolution of symptoms after withdrawal of the medication. There are many other reports of the callosal lesions of Marchiafava-Bignami disease (17–19). This entity had for some years been associated with poorly nourished individuals who are alcoholics but has now been described in nonalcoholic malnourished individuals (20). With respect to our patients, none were being treated for epilepsy. However, it is intriguing to consider the role of nutrition in these cases. Certainly the elderly and patients with cancer are more at risk. The pathologic examination in the positive autopsy case, however, did not show evidence of necrosis described in the acute setting of Marchiafava-Bignami disease but rather a longstanding demyelination. In addition, the clinical features of that disease such as confusion, dysarthria, and seizures were not reported in the medical records. The authors of one report (17), however, suggest that this disorder is in fact more common than previously considered and may lack the classic, more severe symptoms.
After brain radiation therapy, diffuse white matter changes are estimated to occur in 38–100% of patients (21). Furthermore, the extent of this abnormal signal intensity has been shown to be dose dependent in animal models (22). Postradiation deep white matter signal intensity abnormalities commonly follow a similar distribution to that of deep white matter disease seen in older patients and those with atherosclerotic risk factors (2). In the diffuse form, the abnormalities are often symmetric when whole-brain radiation therapy has been given and range from small foci of abnormal signal intensity at the angle of the lateral ventricles to confluent signal intensity abnormality involving most of the cerebral white matter. Focal lesions following radiation therapy, though uncommon, were initially described nearly 71 years ago (23). These rare lesions usually manifest as a necrotic mass lesion with an unpredictable but often poor clinical outcome (24). Pathologic studies have demonstrated that focal and diffuse radiation changes in the brain have a similar microscopic appearance, ranging from mild characteristic vascular changes to coagulative necrosis (21). MR imaging is exquisitely sensitive for detecting the subtle T2 prolongation associated with the vasogenic edema from damage to the capillary endothelium and axonal demyelination commonly seen in radiation-induced white matter disease. After MR imaging evaluation of 18 patients who had received fractionated brain radiation therapy an average of 7.2 months before imaging, we determined that a focal lesion in the corpus callosum is commonly apparent on FLAIR images (16 of 18 patients). This signal intensity abnormality ranged from a small linear band along the undersurface of the splenium, to confluent involvement of the splenium. Furthermore, this lesion may be seen in the absence of the diffuse deep white matter signal intensity abnormality commonly seen following radiation therapy. Of the 10 patients with pre- and posttherapy images available, eight of 10 patients displayed normal signal intensity before radiation therapy and focal increased abnormal signal intensity in the splenium following therapy. These findings suggest that the splenium may be particularly sensitive to radiation therapy. It is of considerable interest to the authors that one of the patients in group 1 with a lesion in the splenium had prior stereotactic radiation therapy for an acoustic tumor that did not include the splenium and two others had only upper chest radiation therapy. Although the lesions we report typically involved the splenium in all cases, it is not at all clear that the pathogenesis in the aging population and that in the radiation cases are the same. In fact, the findings at autopsy suggest that these may represent different lesions.
In a recent article, Friese et al (1) describe 296 patients with abnormalities of the corpus callosum on MR images. In only 59 was a diagnosis established. These included ischemia, Virchow-Robin spaces, diffuse axonal injury, multiple sclerosis, hydrocephalus, acute disseminated encephalomyelitis, Marchiafava-Bignami disease, lymphoma, glioblastoma multiforme, and hamartoma. Such reports foster the general sentiment in the literature that lesions in the callosum are a reflection of some underlying disease. We suggest that such lesions are relatively common, particularly among the elderly and after radiation therapy, and may not warrant further evaluation.
This investigation is intended to be an initial study, and there are some methodologic limitations. The rating system used for scoring abnormal signal intensity in the splenium and periventricular white matter on FLAIR images was not validated with multiple viewers. However, we believe this system is sufficiently simple to avoid being overly subjective. The numbers in all groups are relatively small; however, they are sufficient to provide statistical power. At the inception of this study, we considered that the abnormal signal intensity in the splenium on FLAIR images might represent flow artifact. This motivated us to obtain sagittal images, as these artifacts are extremely unlikely to be reproducible in the same location in two orthogonal imaging planes. Although each component of this study has limitations, the separate investigation of both patient groups and the autopsy findings, taken together, strongly support our findings.
One obvious question is why are these lesions being reported now when MR imaging has been available for over 20 years? It is our contention that it simply reflects the fact that they are more evident on FLAIR images. The proximity to the high signal intensity of the lateral ventricle makes them difficult to identify with confidence on T2-weighted images. This problem is noted with all white matter lesions in the juxtaventricular area, as they are frequently obscured on T2-weighted images by the adjacent high signal intensity of the ventricles. As FLAIR imaging replaces proton density-weighted imaging at many centers, we believe that this finding will be noted with increasing frequency.
Conclusions
Focal high signal intensity in the splenium of the corpus callosum on FLAIR images is a common finding following brain radiation therapy and can be seen in the absence of other white matter changes. A similar signal intensity abnormality on FLAIR images is commonly seen in patients of advanced age with no prior history of radiation therapy. Although the true pathogenesis of this finding remains uncertain, the radiologist should be aware of this common finding and not mistake it for more recognized causes of lesions in the splenium of the corpus callosum.
Acknowledgments
The authors would like to extend their appreciation to Sandra Billings at Dartmouth-Hitchcock Medical Center for her assistance with the preparation of the manuscript.
References
- Received June 10, 2002.
- Accepted after revision November 19, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.