
Abstract
BACKGROUND AND PURPOSE: The relevance of cavernous carotid artery calcification on unenhanced CT scans of the brain has recently been investigated against the backdrop of the widespread implementation of coronary artery calcification scoring. We sought to determine whether the degree of cavernous carotid artery calcification correlated with scores of white matter hyperintensity seen on MR images. In so doing, we sought to establish a relative risk for future stroke on the grade of carotid calcification.
METHODS: Neuroradiologic findings in 187 patients who underwent CT and MR imaging examinations within 1 month of each other were retrospectively reviewed. The degree of circumferential calcification and thickness of calcification were graded for the cavernous carotid arteries on the basis of CT findings. Using the scale developed by the Cardiovascular Health Study, the white matter was graded for degree of disease on the basis of MR findings. Correlation tests and regression analyses were performed to determine the impact of age, race, and sex on results.
RESULTS: Although the cavernous carotid calcification scores and the MR imaging white matter scores showed good correlation (P < .001), the effect was mediated by age. With age factored in as a covariant, no correlation was shown between CT calcification scores and MR imaging white matter scores. Sex had no effect, but African American study participants had worse MR imaging white matter scores than did white participants.
CONCLUSION: After adjusting for age, cavernous carotid calcification grades and MR imaging white matter scores do not show a significant correlation. The relative risk for future stroke cannot be predicted from cavernous carotid calcifications.
The explosive advent of coronary artery calcification scoring centers across the country has been driven by the prevailing belief that such scores attained through electron beam or multidetector CT predict future coronary events (1–3). Although the correlation with coronary arteriography findings has yet to be well established, a correlation still seems to exist between such scores and coronary artery stenosis, and hence, future risk of myocardial infarction, independent of conventional risk factors (4). Such calcification of the coronary arteries may even suggest a diffuse atherosclerotic process throughout the body.
Regarding the prediction of future strokes, it is well known that carotid artery stenosis at the carotid bifurcation is a significant risk factor. A number of large scale studies have shown that endarterectomy reduces the risk of stroke in selected patients with moderate to severe cervical carotid stenosis (5–7). Nonetheless, a number of persons will experience cerebral vascular events even in the face of nonstenotic carotid arteries in the neck. This may, in part, because of intracranial atherosclerosis and stenosis, which are known to affect some segments of the population without concomitant large vessel stenoses in the neck (8–10).
Another recent predictor of future stroke is the degree of white matter signal intensity abnormality on long TR T2-weighted pulse sequences through the brain. Beauchamp et al (11) showed that high scores of white matter disease in the Cardiovascular Health Study (CHS) lead to a higher relative risk for strokes in the ensuing 5 years.
With this project, we sought to grade the degree of cavernous carotid artery calcification and assess its relationship to the CHS white matter ischemic score. In so doing, we hoped to assess whether the degree of cavernous carotid artery calcification could be correlated with future stroke risk similar to the way coronary artery calcification scores can predict future risk of myocardial infarction. Considering that this was a retrospective study, we used the CHS white matter score as a surrogate marker for future stroke risk based on the epidemiologic studies conducted by CHS researchers (12–17). We hypothesized that cavernous carotid artery calcification severity would correlate with higher white matter grade and could thus predict a relative risk for stroke.
Methods
A search of the radiology information system at our institution for patients who had undergone CT and MR imaging within 1 month of each other in 2001 was performed electronically by the information technology group at our institution. Of the list provided by the information technology search, we reviewed films of the first 187 patients who were older than 40 years who had CT scans and MR images that were retrievable. Only CT scans that included bone windows to assess the cavernous carotid artery calcification were included in the retrospective review.
The sample consisted of 102 women and 85 men, with a mean age of 61.5 years (SD, 13.1 years; age range, 40–91 years). The mean age for women was 62.9 years (SD, 13.9 years) and for men was 59.8 years (SD, 11.8). There were 78 African American patients (mean age, 59.1 years; SD, 12.9 years) and 97 white patients (mean age, 63.2 years; SD, 12.9). Twelve patients comprised the “other” racial category (mean age, 62.8 years; SD, 14.5 years).
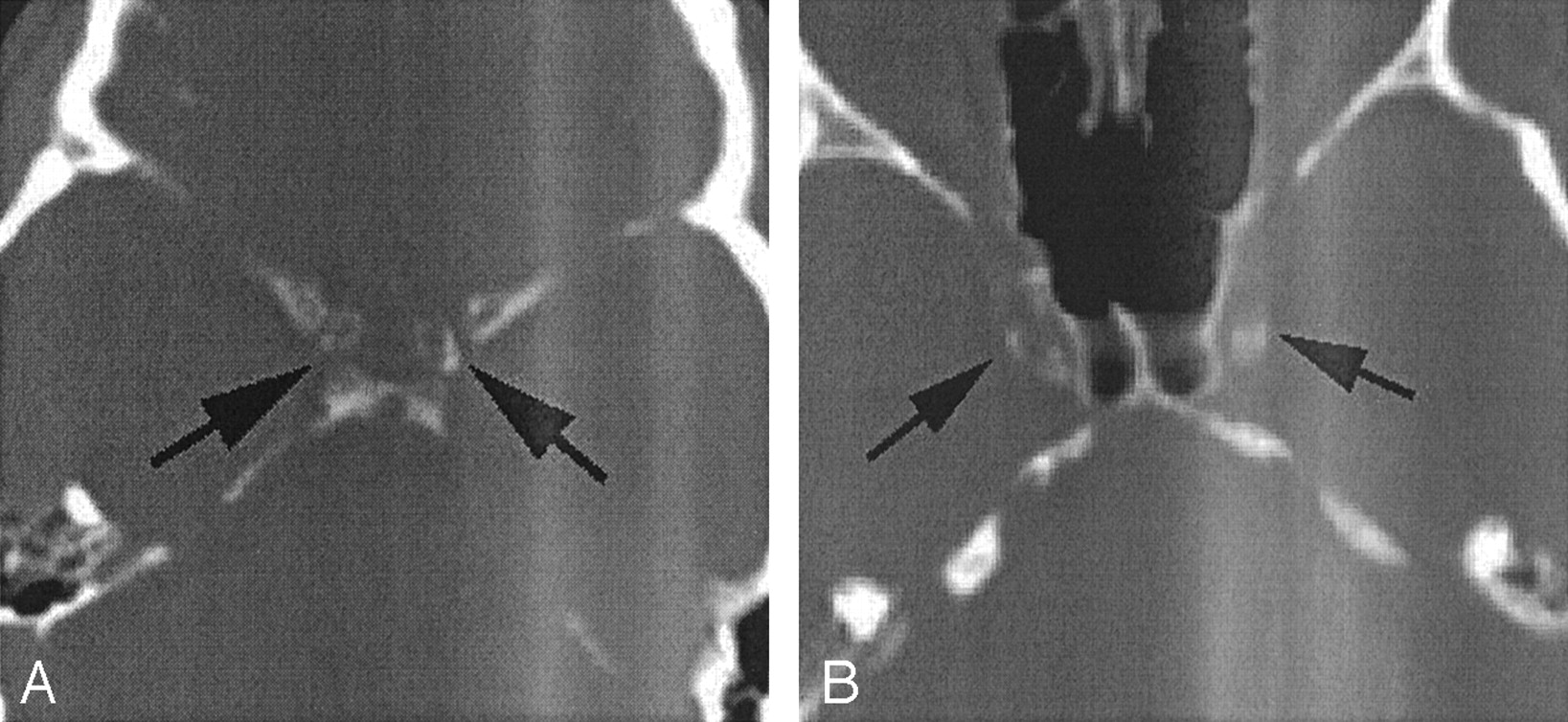
The CT scans were reviewed by an experienced neuroradiologist (D.M.Y) who had earned the Certificate of Added Qualification for Neuroradiology and who had 14 years of experience in the field. The calcifications were graded on a 5-point scale, which is presented in Table 1. In looking at both cavernous carotid arteries, the vessel with the highest score was used (Fig 1). In addition, the thickness of the calcified wall of the cavernous carotid artery was assessed and, once again, the thickest measurement in either carotid artery was used (Table 1). The centimeter scale accompanying the image was used to estimate carotid artery calcification thickness.

CT calcification scores.
A, Circumferential nature of cavernous carotid artery calcification on this CT scan, filmed in a bone window, warrants a grade of 4 (360 degrees of involvement).
B, If the calcification is between 90 and 270 degrees of involvement, it is graded as a 3. The thickness of the calcification, judged by the centimeter scale, was 2 mm in this case.
Grading scales used
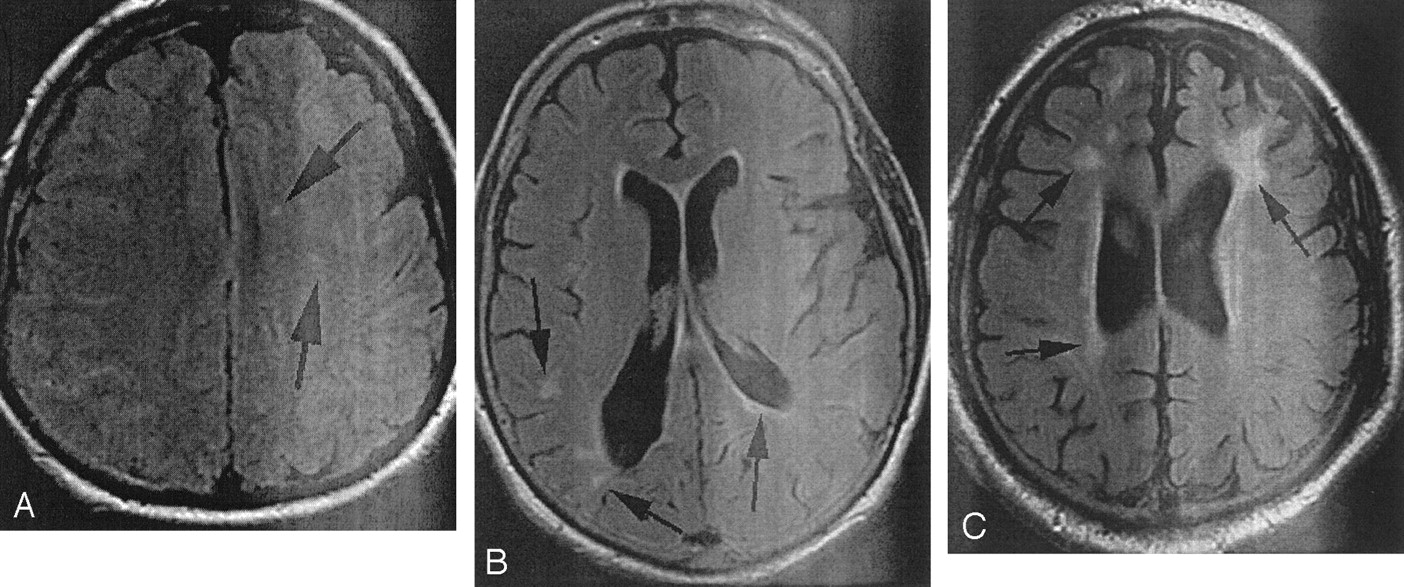
T2-weighted and fluid-attenuated inversion recovery MR images of the white matter were subsequently evaluated in a blinded fashion by the same evaluator, who was unaware at the time of the CT grading scale score for the cavernous carotid arteries (Fig 2). White matter of the brain was assessed by using the scale used by previous CHS researchers (11–17). This scale is noted in Table 1. The reviewer had been trained on the CHS templates for white matter grading. Previous publications report use of this scale, which has shown high reliability and reproducibility (12–17). The CHS scoring system has been shown to have an interobserver reliability rate of 92.1% and an intraobserver reliability rate of 94.5% (12–14). Intraobserver reliability for CT scoring was assessed by multiple readings of 20 cases by the neuroradiologist.

MR imaging white matter disease (arrows) scores. All images obtained through white matter were reviewed by using fluid-attenuated inversion recovery imaging before grades were assigned.
A, This patient was judged to have minimal disease (CHS grade 1).
B, This patients was assigned a CHS score of 4.
C, This patient was assigned a CHS score of 7.
Because we were concerned that demographic factors could play critical roles regarding the extent of intracranial atherosclerosis, differences between sex and racial groups were examined by using either Mann-Whitney tests or Fisher’s exact tests, as appropriate. Additionally, race and sex were considered for inclusion in all logistic regression models presented.
Statistical Analysis
We considered two groups of participants, one having CT scores of 0 or 1 and the other having CT scores >1 (see Table 1). The sample size was determined to achieve a power of 0.8, with an alpha of 0.05 to detect a 30% difference in the MR imaging white matter scores between the two groups of patients. The number of participants required to assess this difference was calculated to be 174. However, the sample size we accrued was increased to 187 to allow for any subdivisions of the data and to address any potential problems with a small number of the scans. Therefore, the first 187 patients meeting entry criteria in 2001 were included in the study.
Spearman correlation coefficients were used to assess the relationships between the degree of circumferential cavernous carotid artery calcification and the MR imaging white matter score, the degree of thickness of the cavernous carotid artery calcification and the MR imaging white matter grading score, and the sum of the values for the degree of peripheral calcification and the thickness of the calcification with the MR imaging white matter score. As per the data presented by Beauchamp et al (11), we subsequently reanalyzed the data by considering only those patients who had a white matter score >5, which is a subgroup that exhibited a relative risk of 9.0 for future stroke in Beauchamp’s work.
We also analyzed the data covariance according to age, to allow assessment of these relationships in the absence of any age differences. For this assessment, a regression analysis was used to assess the effect of the various CT scores on MR imaging white matter scores, when age was included as a covariate.
A Fisher’s exact test was used to assess the relationship between a CT score of ≥2 and an MR imaging score of ≥5. For this analysis, each person’s CT and MR imaging scores were classified in a dichotomous manner. This test was also used to assess the association between calcification thickness (0–1 or >1) and white matter score.
Results
Of the 20 participants who underwent evaluation twice, CT scores of calcification were identical in 15 and were within one grade of the other in five cases. Basic summaries of CT and MR imaging scores recorded in our study are presented in Tables 2 and 3. Using 20 CHS test cases, the reproducibility of the reviewer was 90% for a white matter grade within one value of the first score. The range of error was never more than two grades.
Summary of CT scores
Summary of MR imaging scores
A Fisher’s exact test of the relationship between a CT score of ≥2 for circumferential involvement and an MR imaging white matter score of ≥5 showed that these were highly associated characteristics (P = .023). No association was shown between calcification thickness and white matter score (P = .850). A Mann-Whitney test was performed to compare the CT grades for patients having MR imaging values of 0–4 with those having MR imaging values ≥5. Differences between these two groups were found for circumferential involvement (P = .004), for thickness of calcification (P = .040), and for combined scores (the sum of circumferential and thickness scores) (P = .010). Adjustment for age, however, eliminated all these differences. After adjustment for age, these P values increased to .75 for circumferential involvement, .34 for thickness, and .49 for combined values.
The Spearman correlations for relations of CT scores and MR imaging white matter scores are presented in Table 4. Although an initial review showed that CT scores and MR imaging scores were highly correlated, no relation was shown between CT scores and MR imaging scores after adjustment for age.
Spearman correlation scores
Regression analysis was also conducted by using a binary assessment with MR imaging scores defined as >4 or ≤4 and CT scores separated into 0 and 1 or >1. Only age showed an effect on the MR imaging score, with no independent effect of the CT score after adjustment for age. In a similar fashion, a stepwise regression analysis confirmed that only age showed an effect on MR imaging white matter score and CT score.
An analysis conducted by using logistic regression found that on average, with each year of age, one was 8% more likely to have an MR imaging score >4 (odds ratio comparing two participants 1 year apart is 1.08; confidence intervals, 1.05 and 1.11). Also, age alone explained 27% of the variance found in the MR imaging scores (r2 = 0.27).
The median MR imaging white matter score for African Americans was 3 (25th percentile = 1, 75th percentile = 7), and the median MR imaging white matter score for whites was 2 (25th percentile = 1, 75th percentile = 5) despite a median age of 58 years for the former and 65 years for the latter.
No significant differences were shown in the proportion of participants with MR imaging white matter scores of ≥5 (rather than ≤4) for the different genders (P = .873) or races (P = .101). The proportions of patients with CT scores of circumferential involvement of >1 (rather than ≤1) also showed no differences between races (P = .99) or genders (P = .179). No effects of race or sex were present for calcification thickness as shown by CT or combined circumference-thickness scores. If the MR imaging and CT measurements were considered on the original continuous scale, rather than being dichotomized as above, no differences between races and genders were shown. The Mann-Whitney tests comparing the MR imaging scores yielded P = .784 for sex and P = .170 for race and comparing the CT scores yielded P = .318 for sex and P = .892 for race.
It is important to consider age when making these comparisons. Logistic regression model analyses were used to assess the impact of sex and race on MR imaging and CT scores after adjustment for age. Models assessing the odds of having an MR score ≥5 compared with ≤4 showed that race (P = .004) and age (P < .001) were significant but that sex (P = .458) was not significant. With each year of age, an 8% increase in likelihood of having the higher MR imaging score was present. White race had one-third the likelihood of having the higher MR imaging score compared with the African American race. It is worth noting that very similar results are obtained for the impacts of age, race, and sex when considering the MR imaging score as a continuous outcome in a linear regression. The disparate adjusted and unadjusted results show that it is imperative to take age into consideration when assessing the impact of race on MR imaging score.
When CT scores were evaluated in a similar logistic regression, only age had an effect (P < .001); for each year of age, the likelihood of a higher CT score was 8.2%. Similar results were obtained from linear regression of original CT scores. For all models, for logistic and linear regressions of CT and MR imaging scores, the interactions between age and race, age and sex, and race and sex were not statistically significant (all P values >0.15 for logistic regression and >0.20 for linear regression). Pearson (and Spearman) correlation coefficients to assess the relationships between CT and MR imaging scores after adjustment (or partialing) for age, separately for whites and African Americans and for males and females, showed no linear relationships (all P values >0.4).
Discussion
It would not be surprising if cavernous carotid artery calcification, similar to coronary artery atherosclerosis, could be a reflection of the load of atherosclerotic disease throughout the body. Nonetheless, although briefly mentioned in routine CT reports, little is done with the information that the cavernous carotid arteries are atherosclerotic and/or calcified. The relevance of this finding has not been recently addressed, and because coronary artery calcification seems to have evaluation merit, it was our goal to apply a similar retrospective test to determine the significance of cavernous carotid artery calcification.
Why study vascular calcification? The literature assessing the significance of calcification in plaque has been limited to coronary artery and cervical carotid artery specimens. Many investigators equate the amount of calcification with the degree of plaque burden in the coronary arteries, emphasizing association of advanced lesion with diffuse circumferential pattern of calcium distribution as opposed to point-like presence. On the basis of this recognized model of atherosclerotic progression, we felt justified in assigning the lowest weight to a dot of calcium (extent of calcification score of 1) and the highest weight to a circumferential calcific narrowing (extent of calcification score of 4) (18). When carotid plaques are separated into those with acoustic shadowing on B-mode sonography, which is a good marker of calcification, the hazard ratio for ischemic stroke was significantly higher for those with acoustic shadowing, making detected calcium a good marker of stroke risk (19). However, Duncan et al (20) and Huang et al (21) found that the presence of lipid content but not calcification has an impact on the biomechanical stress on the fibrous cap in ruptured and stable coronary artery plaques. When calcium was replaced with the fibrous part of the plaque, the instability of the lesion increased, indicating a protective role of calcium, even though this slight increase was statistically insignificant. The same replacement of the lipid content by fibrous cap resulted in a median 26% decrease in biochemical stress (18, 21, 22). During the process of plaque expansion, Burke et al observed an increased amount of calcification as the inflammatory infiltration of macrophages linked to the remodeling of the lesion evoked transformation of initial small crystals of calcium into plates and granules of calcium deposits (22).
Because this was a retrospective study, we were unable to conduct assessment of cavernous carotid artery calcification in a way similar to that used for coronary artery calcification with respect to the attenuation, volume, and degree of calcification. In the case of the coronary artery calcification evaluation, the score is calculated according to the Agatston Scale, which is best determined prospectively (23, 24). In that scale, the severity of a calcific lesion corresponds to the peak and area of the attenuation signal intensity in HU on the study. The resultant Agatston score is a summation of the individual lesioned areas located on different sections of the coronary artery. Nonetheless, we think that the scale we used does provide a graded assessment of the degree of atherosclerosis of the cavernous carotid arteries.
The major limitation of our study was its not being a prospective longitudinal study using stroke as an end point. We used a surrogate marker for stroke risk in comparing the cavernous carotid artery calcification scores with the CHS MR imaging white matter scores. Beauchamp et al (11) showed that in those patients with white matter scores of ≥5, an increased risk of subsequent stroke during a 5-year follow-up period exists. Stroke risk by white matter grade showed a stepwise increase in incidence rates, from 5.9 per 1000 person-years for grades 0–1 to 28.1 per 1000 person-years for grades ≥5, with an age-adjusted hazard ratio of 3.8. The hazard ratio was only slightly attenuated to 3.3 after adjusting for other known stroke risk factors (11). The risk of stroke was 2.8% per year for participants with white matter scores ≥5, compared with only 0.6% for participants with grades 0–1. Furthermore, 91 of the 159 strokes reported occurred among the one-third of the participants with grade 3 or higher (11).
An optimal study design would follow the patients for an extended period of time to determine stroke risk, perhaps in a form similar to the CHS in which Agatston-like analysis of carotid artery plaque and longitudinal follow-up would be valuable. At that time, both carotid bifurcation calcification and cavernous carotid artery calcification could be assessed for subsequent stroke risk. The need to justify radiation exposure for the CT study may, however, preclude large-scale longitudinal studies of this type for the population (25). It is for this reason that our exploratory retrospective research project was viewed as a means for determining relative risk. Although cervical carotid atherosclerosis may be a signature of total body atherosclerotic plaque load, it is also known that African Americans may have intracranial stenoses without significant neck findings (6, 9).
Reports in the literature suggest that the distribution of atherosclerotic deposits is race- and sex-dependent when analyzed regarding extracranial and intracranial location. Although whites have a significantly greater incidence of stenosis of the extracranial internal carotid artery, in African Americans and Hispanics, intracranial atherosclerosis has been reported to be more prevalent (7, 26). Male sex can also be a predictor for intracranial lesions, because female persons have reduced amounts of intracranial disease, even though at the same time, especially in the case of female whites, a substantial increase in extracranial carotid artery lesions is present (10). Because whites are characterized with a higher occurrence of significant arterial stenosis, they are also at a higher chance of a preventive detection and a correct assessment for endarterectomy as compared with persons of other ethnicity (27). We did not see a significant relationship between sex or race and CT grades in our study population. However, African Americans did have a higher mean MR imaging white matter score, signifying more disease than whites, an effect that was significant even after adjusting for age in the logistic regression analysis. However, within each sex and race, no relationship was shown between calcified carotid plaque scores and MR imaging white matter scores.
Thus, we found that calcification scores and MR imaging white matter scores showed a significant relationship, but it was mediated only by the age of the patient (as patients got older, they had both more cavernous carotid artery calcification and more white matter disease). Race had a small but independent influence on the MR imaging scores but not on the CT grades; sex did not have an influence. The impact of these variables was overshadowed by age. Cavernous carotid artery atherosclerotic CT scores independently could not predict extent of white matter disease and hence could not predict relative risk of stroke.
Conclusion
Our results show no definite correlation between a high cavernous carotid artery calcification score and advanced white matter grade once one adjusts for age. Our study has shown that cavernous carotid artery calcification and MR imaging white matter scores are linked through the effect of age and do not have an independent relationship in the genders and races studied herein. The significance of cavernous carotid artery calcification as it relates to future stroke risk was not borne out in this study, but a longitudinal study using stroke rather than MR imaging score as an outcome measure may be worthwhile.
References
- Received October 21, 2002.
- Accepted after revision December 9, 2002.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}