
Abstract
BACKGROUND AND PURPOSE: An embolus causing cerebral ischemia is a major cause of death and disability, and the search for methods to reestablish blood flow is of major importance. A technique for the emergent primary treatment of cerebral emboli causing stroke is presented in detail.
METHODS: The method developed implies the mechanical extraction of the embolus with a standard vascular retrieval snare via the endovascular route without the use of thrombolytic agents.
RESULTS: Five consecutive patients were treated to extract an embolus. All patients had substantial improvement in their clinical status. No revascularization hemorrhages occurred.
CONCLUSION: In this small series, the embolectomy method described was reproducible, rapid, and safe. It may offer an alternative to other methods of vascular recanalization.
Embolic occlusion of cerebral arteries is a major cause for stroke. Studies have been performed to evaluate the effectiveness of intravenous thrombolysis in this condition (1–3). Although these studies show positive results when strict criteria are used, the risk of hemorrhagic transformation is increased, possibly because of the fibrinolytic agent. Other techniques have also been investigated and used in certain instances (4–6). The results have varied, partly because of the use of suboptimal tools and techniques and possibly because of the variability of rest circulation in the vascular bed distal to the occlusion. The possibility of mechanical embolectomy has been described earlier, and the technique used herein seems to be fast and reproducible.
Methods
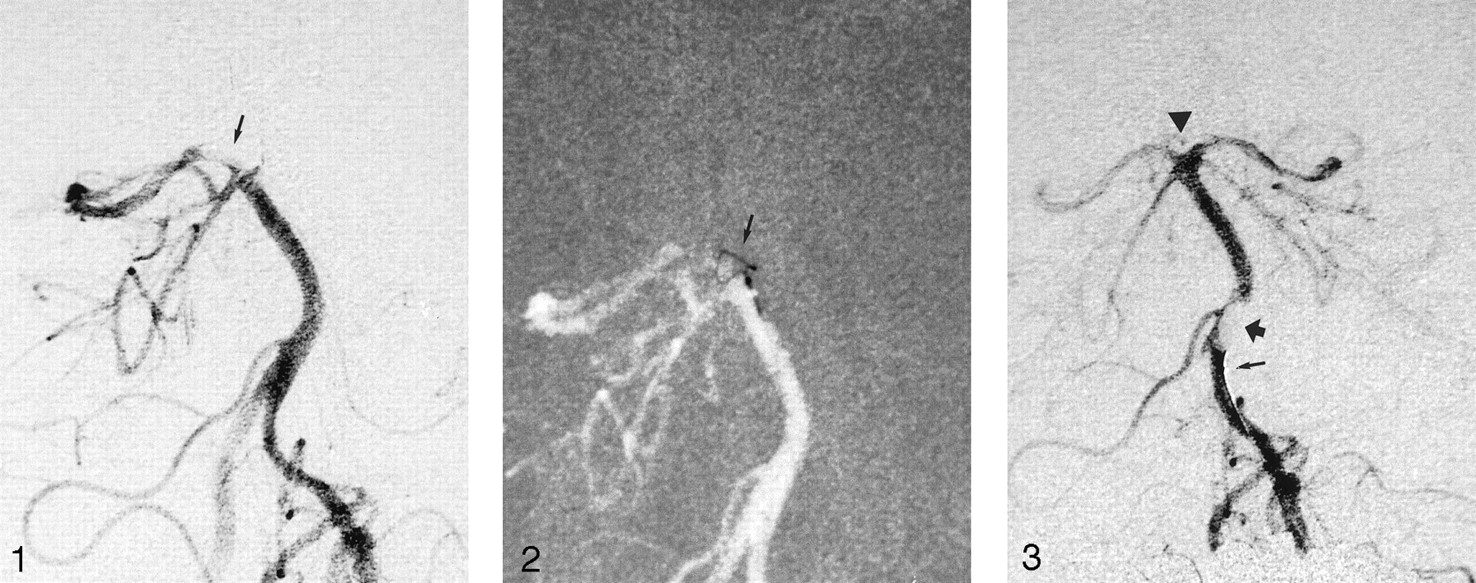
After a CT scan excluded hemorrhage in a patient with acute stroke, immediate diagnostic angiography was performed. Very early signs of ischemia did not prevent us from trying embolectomy. A regular angiographic technique was used for the intervention. In our setting, this technique includes the use of a 6F introducer in the femoral artery through which a 6F guiding catheter is inserted into the extracranial segment of the cerebral artery supplying the area of involvement. If the angiogram shows an arterial occlusion, a microcatheter is positioned with its tip just proximal to the occlusion. A vascular retrieval snare (Amplatz Goose Neck; Microvena Corporation,White Bear Lake, MN) is then introduced. To illustrate the procedure, a case with a basilar tip embolus is included (Fig 1). The snare has to have about the same diameter as the occluded vessel. The loop of the snare is pushed out of the microcatheter just enough for it to open fully and take its built-in shape perpendicular to the catheter and the vessel. The microcatheter is then pushed together with the snare into the embolus, and a minor buckling of the loop can often be seen (Fig 2). After this, the snare is pulled back slightly into the microcatheter so that only a small eye can be seen outside the catheter tip on fluoroscopy. Then, the microcatheter and snare are pulled out a few centimeters. A control angiogram is cautiously obtained to verify the status (Fig 3). If the embolus is caught in the snare, the whole assembly of the snare, the microcatheter, and the guide catheter is pulled out as a unit. This is done to minimize the risk of dislodging the embolus from the snare. If a regular introducer is used, the clot often gets stuck in the valve of the introducer. The clot can be removed by introducing a Luer syringe (without lock) through the valve and aspirating. To facilitate removal of the clot, an introducer with a removable valve can be used. Otherwise, an embolus lost distal to the vessels from the aortic arch is usually asymptomatic.

Diagnostic angiogram (left vertebral artery injection, anteroposterior projection of the basilar artery) shows the basilar tip embolus (arrow) occluding the left posterior cerebral artery, the left superior cerebellar artery, and the basilar tip perforators going to the thalamus.

The snare (arrow) has been pushed out of the microcatheter just enough to open fully, and together with the microcatheter, it has been further pushed into the embolus. A minor buckling of the loop is seen.

The snare has been partially withdrawn into the microcatheter, leaving a small eye outside the tip (bottom arrow) of the microcatheter. After this, the microcatheter with the snare is pulled back a few centimeters, and contrast material is injected. The angiogram shows the clot (top arrow) as a lucency in the contrast material hanging from the tip of the microcatheter. The now-open basilar tip is clearly seen with all of the branches filling (arrowhead).
Results
After the development of this new technique, five consecutive cases were treated successfully. The neurologist in charge admitted four patients with stroke to the neuroradiology section on an emergency basis. Occlusion of middle cerebral artery was clinically suspected in two cases, and occlusion of the basilar artery was suspected in two cases. CT scans had shown no sign of ischemia in three cases and early signs of ischemia in one. In one patient, the embolus was a complication of endovascular aneurysm treatment. Mechanical embolectomy was intended as first treatment, and the emboli were extracted in 20–30 minutes. Blood flow was reestablished within 2–10 hours after ictus. In all of these cases, the clinical outcome was judged to be better than that expected on the basis of the natural history (Table). Another team member successfully performed two of the treatments after receiving only oral instructions similar to those described in Methods. None of the treated patients had a hemorrhage after embolectomy.
Clinical data
Discussion
Stroke is often a personal tragedy that severely affects an individual and that individual’s family. It is also a common condition that creates a large economic burden for society. Those within and outside the medical profession have shared the opinion that stroke is something that has to be accepted and that a direct cure does not exist.
With the introduction of new fibrinolytic drugs, the possibility of direct treatment of an embolus has been investigated. Studies about drug-induced fibrinolysis in this condition have been performed, and improvements in the treatment group have been shown (1–3). The importance of early treatment has been emphasized. In this respect, early treatment means treatment before a good-quality CT scan shows any abnormality, depending on ischemia, and a 3-hour window is recommended (7). For new treatment possibilities to have full impact, everyone from the patient to the first medical contact to the treating physician, must recognize the need for the urgent treatment of stroke.
In interventional neuroradiology, the skill of safe intravascular navigation in the brain has been used for intra-arterial thrombolysis and, at times, for treating an embolus as a complication of an interventional procedure. In the embolization of recently ruptured intracranial aneurysms, the prospect of giving the patient large doses of potent fibrinolytic drugs has been a concern, and the search for other methods have been ongoing. We have tried to burst the embolus with a forceful injection of sodium chloride solution or to disrupt it with a microguidewire, with variable success. The use of a vascular retrieval snare intended for extracting foreign bodies from the vascular tree have been described before (4–6). The result of those procedures is slightly unpredictable, but with the technique described herein, it seems to be far more reliable, and in five consecutive cases, we succeeded in extracting the embolus within 20–30 minutes after the patient entered the angiography suite.
In thrombolysis, the concentration of lytic drug around the clot and the lytic activity is higher when an intra-arterial infusion is used than when an intravenous injection of fibrinolytics is used. Still, with direct intra-arterial infusion in and around the embolus, 1–2 hours is often required to open the vessel. Opening the vessel with an intravenous infusion is probably longer because of the lower local drug concentration. In our experience so far, a fast mechanical revascularization saves the time lost when a patient is transported from the CT scanner to the angiography suite. The fast reestablishment of blood flow without exposing the patient to large doses of fibrinolytic drugs is an appealing prospect. If the snare fails, little time is lost, and intra-arterial fibrinolysis can be started immediately, because the microcatheter is in place.
The manipulation of a clot poses a definite risk of its dislodgment or rupture. In our experience, the extracted clot is far more coherent than what could be expected, even if the clot forms just minutes before, as a complication to a treatment. Despite this possibility, the snare will probably be able to cut the clot into pieces if withdrawn fully into the microcatheter. We have in these five cases not lost symptom giving parts of clot due to this. Also, the use of these microsnares in the intracranial circulation does not seem to be more risky than the use of other tools that we regularly apply in, for example, freshly ruptured aneurysms.
One important question is whether this kind of recanalization, without the use of fibrinolytics, differs from the intravenous fibrinolysis, regarding the risk of hemorrhagic transformation. Can this technique offer the possibility of opening the vessels, even beyond the 3-hour window and after early signs of edema are diagnosed on CT scans? One of our cases involved such a scenario.
The presented technique is reproducible and can undoubtedly be used in embolic complications during neurointerventional procedures.
This small group of patients has not been treated in a formal trial. The interventions have been performed as a last effort to save brain parenchyma, at times in a desperate situation. Intravenous thrombolysis has not been available in Europe, and it is not the option of choice in a patient with a recently ruptured intracranial aneurysm. Because of this situation, approval of the ethics committee was not requested. For further planned study in patients with a National Institute of Health Stroke Scale score above 15 (not to be subjected to intravenous thrombolysis), approval of the ethics committee approval is required.
Conclusion
This article contains a close description of a technique for the emergent extraction of emboli from the cerebral circulation. The intention is to spread the knowledge of this possibility to neurologists and interventional neuroradiologists. The usefulness of this technique was proved in five consecutive, successful cases. Its true value, as compared with that of alternatives, needs further study.
- Received October 1, 2002.
- Accepted after revision December 11, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Mechanical Embolectomy for Acute Ischemic Stroke in the Anterior Cerebral Circulation: The Gothenburg Experience during 2000-2011
- Mechanical thrombectomy as the primary treatment for acute basilar artery occlusion: experience from 5 years of practice
- Mechanical Thromboembolectomy for Acute Ischemic Stroke: Comparison of the Catch Thromboectomy Device and the Merci Retriever In Vivo
- Debunking 7 Myths That Hamper the Realization of Randomized Controlled Trials on Intra-Arterial Thrombolysis for Acute Ischemic Stroke
- Mechanical Thrombectomy for Acute Ischemic Stroke: Thrombus-Device Interaction, Efficiency, and Complications In Vivo
- Analysis of Thrombi Retrieved From Cerebral Arteries of Patients With Acute Ischemic Stroke
- Mechanical Thrombolysis in Ischemic Stroke Attributable to Basilar Artery Occlusion as First-Line Treatment
- Reasons for exclusion from thrombolytic therapy following acute ischemic stroke
- Extending Reperfusion Therapy for Acute Ischemic Stroke: Emerging Pharmacological, Mechanical, and Imaging Strategies
- Use of mechanical extraction devices in basilar artery occlusion
- MERCI 1: A Phase 1 Study of Mechanical Embolus Removal in Cerebral Ischemia
- Endovascular embolectomy of acute basilar artery occlusion