
Abstract
Summary: We describe a case of an actively bleeding aneurysm demonstrated by CT angiography (CTA). The active hemorrhage was characterized by a nebulous attenuation in the subarachnoid space adjacent to the aneurysm. The measurements (HU) of the hemorrhage were equal to or slightly less than those of the contrast material in the arteries and diminished as one moved further from the aneurysm. As CTA is used more frequently in the diagnosis of cerebral aneurysms, it is important to understand imaging features of this potentially lethal condition.
CT angiography (CTA) is being used more frequently in the diagnosis of cerebral aneurysms. An actively bleeding aneurysm is a dangerous and potentially lethal condition. We describe the CTA characteristics of a patient with this condition.
Case Report
A 35-year-old man presented with a weeklong history of severe headache. On admission, a CT scan failed to demonstrate evidence of subarachnoid blood. Lumbar puncture findings revealed xanthochromia. Results of the neurologic examination were unremarkable. The patient was referred for CTA to rule out an aneurysm.
CTA was performed on a multisection, spiral scanner with the following parameters: high quality pitch with 1.25 mm collimation, reformatted to intervals of 0.5 mm. One hundred twenty-five milliliters of contrast material were injected at 4.5 mL/s with an 18-second delay. The images were reformatted with volume-rendering reconstruction.
CTA is performed routinely at our institution as the initial study in a patient with a suspected aneurysm. The diagnosis of cerebral aneurysms by using this technique is usually rather straightforward because of the stark difference in HU between bone, brain, and cerebral spinal fluid and the contrast in the vessels and in the aneurysm. The aneurysm appears as a clearly demarcated area of enhancement outside the normal vascular lumen. Published data (1), as well as our experience, have shown that the contrast that fills the aneurysm during CTA can routinely be distinguished from acute subarachnoid blood on the basis of HU. The attenuation of contrast material in the lumen of an aneurysm ranges between 110–350 HU (1), whereas the attenuation of acute subarachnoid blood is about 80 HU (1). Therefore, by manipulating the window and level on the CTA images to filter out the subarachnoid blood, the aneurysm can be clearly demonstrated in most patients, even in the presence of an acute hemorrhage.
In this case, interpretation of the reformatted images was somewhat problematic. The current study demonstrated a nebulous area of increased attenuation adjacent to the right internal carotid artery (Fig 1). The attenuation of this poorly defined area was highest near the internal carotid artery (322 HU). This was equal to the attenuation of the contrast within the lumen of the carotid artery itself and was much higher than the expected attenuation of subarachnoid blood. As one moved further from the carotid artery, the attenuation diminished gradually until it became isoattenuated relative to cerebrospinal fluid (0 HU) (Fig 1A).

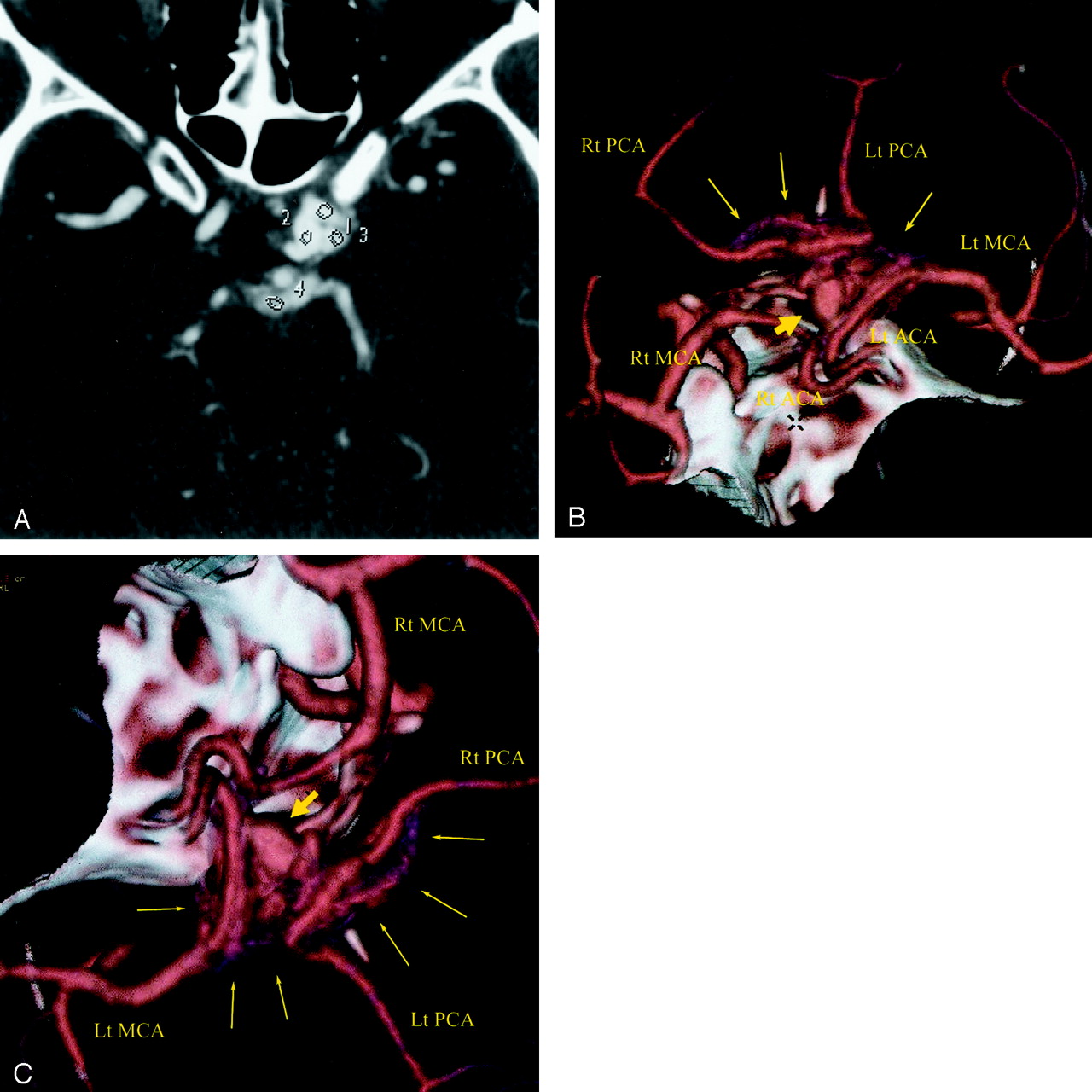
CTA of an actively bleeding aneurysm in a 35-year-old man.
A, Axial source image through the aneurysm. Region of interest 2 is in the aneurysm itself and measures 322 ± 14 (mean ± SD) HU. The other three regions of interest (1, 3, and 4) outline areas of extravasated contrast material outside the lumen of either the aneurysm or the blood vessels. The attenuations of these regions of interests are 300 ± 40, 275 ± 29, and 195 ± 15 HU, respectively. This is much higher than what is seen for blood, which is typically on the order of 80 HU. The patient did not receive contrast material before CTA was performed. This leads on to the inescapable conclusion that the only possible source of this attenuated material in the subarachnoid space is contrast material from an actively bleeding aneurysm. The attenuation measurements in the subarachnoid space (regions of interest 1, 3, and 4) are slightly below what was seen in the aneurysm and decrease as one moves further away form the aneurysm, most likely because of dilution of the contrast material with CSF.
B and C, 3D reconstruction of the CTA data. Large arrows depict the superior hypophyseal artery aneurysm. The small arrows show a nebulous area of increased attenuation in the subarachnoid space adjacent to the aneurysm that represents the actively extravasating contrast material from the bleeding aneurysm. The attenuation of this area is equal to or slightly below that of the contrast material in the vessels.
By narrowing the window to exclude most of the nebulous area that was slightly hypoattenuated relative to contrast material in the blood vessels, we were able to demonstrate a superior hypophyseal artery aneurysm (Fig 1B and C). We surmised that the nebulous area represented active bleeding and consequential extravasation of contrast material into the subarachnoid space adjacent to the aneurysm at the time of imaging. Because the attenuation in the subarachnoid space was much higher than the known attenuation of blood, and because the patient had not previously received contrast material, the inescapable conclusion was that the only possible source of this attenuation in the subarachnoid space was actively extravasating contrast material.
Immediately after CTA was performed, the patient had a grand mal seizure from which he quickly recovered. In the largest series of cases of ruptured aneurysms during conventional angiography, three of the 10 patients seized during or immediately after the injection of contrast material that demonstrated acute bleeding of the aneurysm (2). Therefore, timing of the patient’s seizure supported the radiologic findings of an actively bleeding aneurysm during revealed at CTA.
CTA was followed by a conventional angiography 1 hour later, which confirmed the suspected aneurysm. No active bleeding existed at conventional angiography. A CT scan obtained immediately after angiography showed contrast material and hemorrhage filling the subarachnoid spaces, which was confirmed by HU measurements. Because the routine head CT scan obtained before CTA did not show evidence of a hemorrhage, the presence of blood and contrast material in the subarachnoid space on this follow-up study proved that the aneurysm had bled in the interim. The only source of contrast material was from the CTA study.
The patient was taken immediately to the operating room. Neurosurgical exploration confirmed the presence of a recent hemorrhage in the subarachnoid space. Clips were placed in the aneurysm, and the patient had an uneventful recovery.
Discussion
CTA has great potential for the diagnosis of aneurysms, and we may be approaching a time when CTA could replace conventional angiography (3–5). CTA offers several advantages over conventional angiography: It is minimally invasive, faster, easier to perform, and has fewer complications, such as strokes. However, with the introduction of every new technique, pitfalls and nuances are uncovered. The actively bleeding aneurysm discovered at CTA represents such an instance. Therefore, with the expected increase in the use of CTA, it is imperative to understand the imaging characteristics of an actively bleeding aneurysm on CTA images and to quickly and accurately diagnose this potentially lethal condition.
Discovery of an actively bleeding aneurysms is uncommon even during conventional angiography (2–6); however, diagnosis is straightforward with this technique. The diagnosis of an actively bleeding aneurysm by use of CTA can, in principle, be made the same way; that is, by demonstrating the presence of contrast material in the subarachnoid space adjacent to an aneurysm, active bleeding can be confirmed. As this case shows, however, the presence of contrast material in the subarachnoid space on a CTA image makes interpretation of three-dimensional reformatted images more challenging.
In the case of CTA of a nonbleeding aneurysm, the contrast material within the lumen of the parent vessel and the aneurysm can easily be differentiated from the surrounding cerebrospinal fluid, bone, and brain tissue. Even in cases in which the aneurysm has recently bled, but is not actively bleeding during CTA, the intraluminal contrast that defines the aneurysm can be separated from the surrounding blood in the subarachnoid space on the basis of HU (1). Typically, contrast in the lumen of a vessel or an aneurysm has a value of 150–350 HU, whereas the typical value of acute subarachnoid blood is about 80 HU. In addition, blood in the subarachnoid space mixes with cerebrospinal fluid, which further reduces the value in HU.
Conclusion
The current case demonstrated a nebulous attenuation that was only slightly less attenuated than the aneurysm and the parent vessel. In addition, this attenuation diminished gradually as one moved further from the aneurysm, until it blended into the surrounding cerebrospinal fluid. We surmised that this attenuation represented active extravasation of contrast material into the subarachnoid space at CTA. The decreased attenuation was caused by mixing of the contrast material with cerebrospinal fluid, which led to dilution of the contrast material and a consequential drop in attenuation as one moved further from the ruptured, bleeding aneurysm.
Footnotes
Presented at the 39th Annual Meeting of the American Society of Neuroradiology, Boston, Mass, April 21–27, 2001.
- Received February 1, 2002.
- Accepted after revision October 1, 2002.
- Copyright © American Society of Neuroradiology





{kind=link}