
Abstract
Summary: We present the non-contrast-enhanced CT finding of high attenuation within metastatic regional lymph nodes in two patients with stage I or II tongue carcinoma during a follow-up period. The attenuation values of these lesions were approximately 70 HU or more. One patient had a level I node, and the other had a level II node. Contrast-enhanced CT failed to reveal these hyperattenuated areas within the nodes. Histopathologic examination revealed that these hyperattenuated areas were strongly correlated with the area of marked keratinization of metastatic foci. If contrast-enhanced CT had been the only imaging technique used, these lesions might have been overlooked. The clinician should be aware of the characteristic findings of non-contrast-enhanced, as well as contrast-enhanced, CT when investigating lymph node metastases at an early stage in patients with stage I or II tongue carcinoma during the follow-up period.
The presence of regional lymph node metastases has a major influence on the prognosis of patients with tongue carcinoma (1). Occult lymph node metastases can be expected in more than 30% of patients with T1 and T2 tumors and N0-stage necks (1). Watchful observation followed by salvage surgery for subsequent metastases is one approach that has been advocated in the management of patients with N0-stage necks. Others have advocated elective neck dissection for the initial management of patients with T1 and T2 tumor. Despite that the frequency of regional recurrence has been reduced by elective neck dissection, its beneficial effects on survival remain controversial when compared with the benefit of watchful observation (2–5).
It has recently been reported that marked keratinization of tumor foci within metastatic nodes in patients with tongue carcinoma had higher attenuation than did surrounding soft tissue on non-contrast-enhanced CT images (6). Nevertheless, our search of the literature did not yield reports of notable non-contrast-enhanced CT findings of lymph node metastases in patients with tongue carcinoma during a follow-up period. The aim of this report is to present two cases of hyperattenuated non-contrast-enhanced CT findings within metastatic lymph nodes and to assess the significance of non-contrast-enhanced CT in detecting cervical lymph node metastases at an early stage during a follow-up period in patients with stage I or II carcinoma.
CT Examination
All CT images were obtained with a helical CT scanner (Xvigor Real; Toshiba, Tokyo, Japan). Patients were placed in a supine position and 3-mm-thick non-contrast-enhanced conventional scanning was performed parallel to Reid’s baseline (the anthropologic baseline) followed by contrast-enhanced helical scanning. By using a power injector (Autoenhance; Nemoto Kyorindo, Tokyo, Japan), contrast material (100 mL of iopamidol 300 or 75 mL of ioversol 320) was administered at a rate of 1.5 mL/s. Helical scanning of a primary lesion and cervical lymph nodes was started 45 seconds after the initiation of contrast material infusion. The scan data were acquired by using a collimation of 3 mm and a table speed of 3 mm/s (pitch 1/s) and were reformatted into 3-mm-interval axial images. All images were evaluated with a soft tissue algorithm (window width, 240 HU; window level, 40 HU). Follow-up CT was recommended when findings of monthly repeated follow-up sonography suggested possible lymph node metastases. All cervical lymph nodes shown by CT were classified according to lymph node levels. Level I corresponded to the submandibular and submental areas. Levels II, III, and IV were defined as three equal parts medial to the sternocleidomastoid muscle around the internal jugular vein. Level II corresponded to the high jugular and jugulodigastric lymph nodes. Level V was posterior to the sternocleidomastoid muscle (posterior triangle).
Case Reports
Case 1
A 79-year-old woman was referred in September 2000 because of an ulceration on the left side of her tongue. The primary lesion was classified as stage I (T1N0M0) according to the classification system of the Union Internationale Contrele Cancer (UICC) staging (1997). No regional metastatic findings were observed by use of either CT or sonography at initial examination (Fig 1A). Partial glossectomy was performed, and squamous cell carcinoma was verified histopathologically. A first follow-up, CT was performed 1 month after surgery, because follow-up sonography revealed an enlargement of the left level I node (Fig 1B). The minimal axial diameter of the node was measured as 10 mm on a CT image. On the non-contrast-enhanced CT image, the lymph node was completely hyperattenuated (Fig 1C), which was a finding that was not observed at initial examination. A contrast-enhanced CT image obtained concomitant with Figure 1C did not show any hyperattenuation (Fig 1D). Radical neck dissection on her left side was performed. After neck dissection, the surgeon oriented unfixed specimens, and the locations of lymph nodes were recorded on a cervical anatomic figure. By recording the location and the size of all lymph nodes, it was possible to correlate individual lymph nodes with each lymph node level, but we were unable to correlate each lymph node with that found in the surgical specimen except for the largest one of each lymph node level. The dissected specimen was examined histopathologically and only one level I node was proved to have metastatic foci. Because the histopathologically metastatic lymph node was the largest one of level I, side-by-side comparison between the hyperattenuated lymph node detected on CT and the histopathologic specimen was confirmed without difficulty. Histopathologic examination suggested that the lymph node was completely replaced by metastatic tumor, and hyperattenuation on non-contrast-enhanced CT images involved marked keratinization within metastatic foci (Fig 1E).

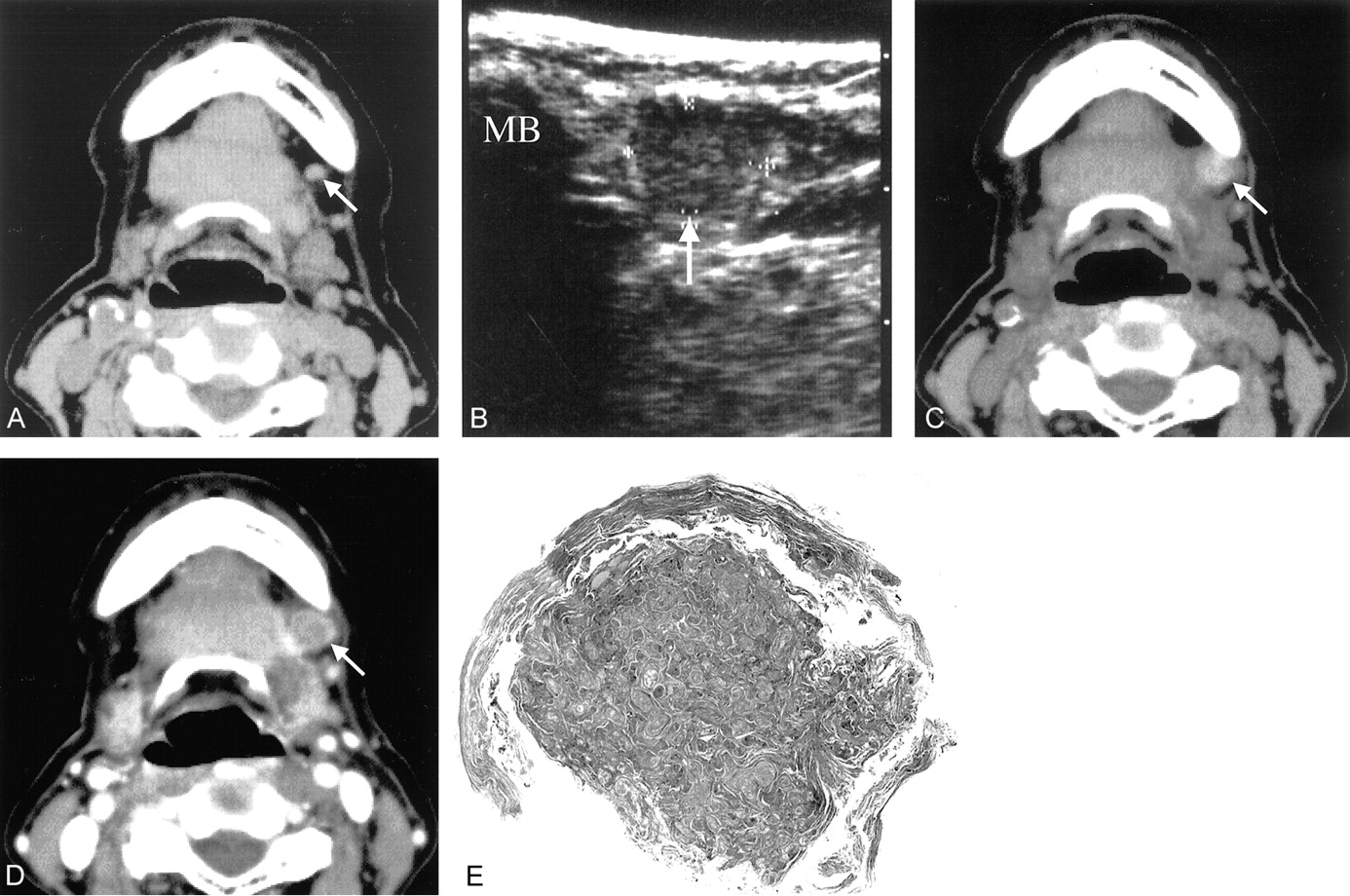
Case 1, a 79-year-old woman with squamous cell carcinoma of the left side of her tongue.
A, Non-contrast-enhanced CT image obtained at initial examination of a level I node (arrow); no hyperattenuation is evident.
B, First follow-up sonogram at the level I node obtained 1 month after surgery of the primary tumor (transverse section). Note an enlarged lymph node (arrow) with heterogeneous internal echo. MB indicates mandible.
C, Non-contrast-enhanced CT image at the level I node obtained 1 month after surgery of the primary tumor. Hyperattenuation entirely occupies the node (arrow). The size of the node has increased, and the minimal axial diameter of the node is 10 mm.
D, Contrast-enhanced CT image obtained at the same level and time as that of A. Hyperattenuation within the node (arrow) is obscured after the administration of contrast medium.
E, Photomicrograph (stain, hematoxyllin-eosin; original magnification, ×2.5) shows the level I node is entirely replaced by the area of marked keratinization (arrows). The non-contrast-enhanced CT finding of hyperattenuation is likely correlated with this marked keratinization.
Case 2
An 80-year-old woman was referred in January 2001 because of an irritation on the right side of her tongue. The primary lesion was classified as stage II (T2N0M0) according to the UICC staging system. No regional metastatic CT or sonographic findings were observed at initial examination (Fig 2A). Partial glossectomy was performed, and squamous cell carcinoma was verified histopathologically. A first follow-up CT examination was performed 7 months after partial glossectomy because the ninth follow-up sonographic examination revealed enlargement of the left level II node (Fig 2B). The minimal axial diameter of the node measured on a CT image was 9 mm. Non-contrast-enhanced CT clearly showed hyperattenuation at the margin of the level II node (Fig 2C), which was not observed at initial examination. Contrast-enhanced CT performed concomitant with Figure 2C failed to show hyperattenuation (Fig 2D). The patient underwent radical neck dissection on her right side. The dissected specimen was examined histopathologically, and only one level II node proved to have metastatic foci. Because the histopathologically metastatic lymph node was the largest one of level II, side-by-side comparison between the hyperattenuated lymph node detected by use of CT and histopathologic analysis was confirmed without difficulty. Histopathologic examination suggested that the hyperattenuation on non-contrast-enhanced CT images involved marked keratinization within metastatic foci (Fig 2E).

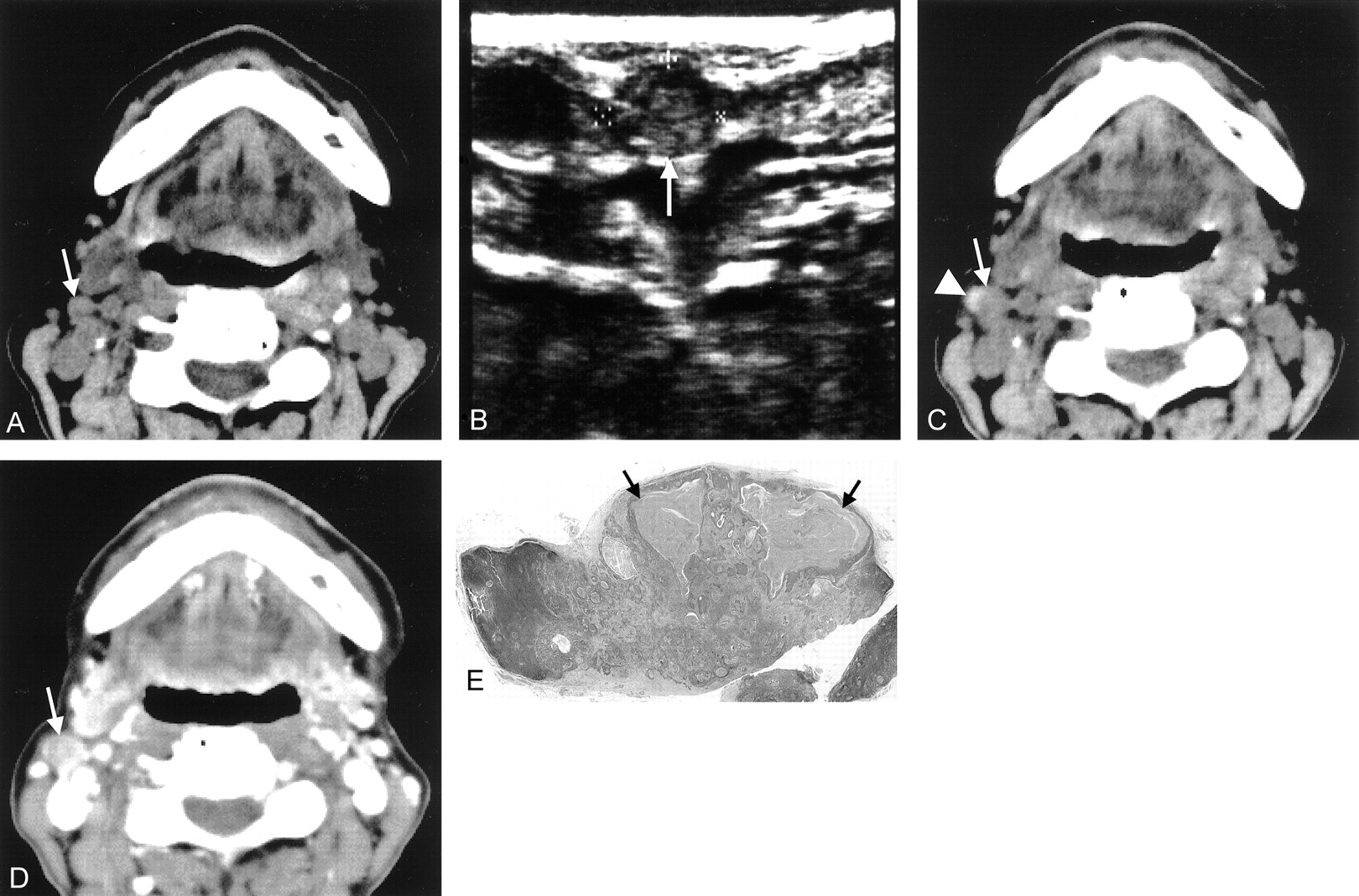
Case 2, an 80-year-old woman with squamous cell carcinoma of the right side of her tongue.
A, Non-contrast-enhanced CT image at a level II node (arrow) obtained at initial examination; hyperattenuation is not evident.
B, Ninth follow-up sonogram at the level II node obtained 7 months after surgery of the primary tumor (transverse section). Note an enlarged lymph node (arrow) with heterogeneous internal echo.
C, Non-contrast-enhanced CT image at the level II node obtained 7 months after surgery of the primary tumor. Note the hyperattenuation (arrowhead) at a lateral margin of the node (arrow). The size of the node increases and the minimal axial diameter of the node is 9 mm.
D, Contrast-enhanced CT image obtained at the same level and time as that of C. The level II node (arrow) enhances, and hyperattenuation is obscured after the administration of contrast medium.
E, Photomicrograph (stain, hematoxyllin-eosin; original magnification, ×2) demonstrates the area of marked keratinization (arrows) within metastatic foci at the marginal portion of the largest one of level II node. The non-contrast-ehnahced CT finding of hyperattenuation appears to be correlated with this marked keratinization within metastatic foci.
Discussion
CT is the widely used technique for neck staging (7). The most accurate CT sign of metastasis is the contrast-enhanced CT finding of central necrosis, which has been reported to have a specificity of 100% (8). Nevertheless, our search of the literature did not yield any notable reports of hyperattenuated non-contrast-enhanced CT findings related to lymph node metastasis in patients with N0 necks during a follow-up period.
In squamous cell carcinoma of the head and neck, the degree of keratinization of the metastatic tumor within cervical lymph nodes is varied (9) and well correlated with that in primary tumor (10); however, little is known about CT findings relating to keratinization of metastatic tumor. Nakayama et al (6) have reported that metastatic foci with marked keratinization demonstrate high attenuation on CT images. They proposed that high attenuation with the CT value lower than that of calcification might be a sign of metastatic nodes. In their case, the CT value of metastatic nodes exceeded 300 HU. Although the CT value of hyperattenuated areas within metastatic nodes in the present cases was lower than that of previous reports, we could accurately detect metastatic nodes because hyperattenuated areas, which had not been observed at initial CT examination, newly appeared on a follow-up CT study. It was suggested that metastatic nodes in an early stage of metastases could be identified by careful observation of non-contrast-enhanced CT images.
Tuberculosis or metastatic papillary thyroid carcinoma commonly causes nodal calcification (11). Calcification might resemble hyperattenuated areas within the lymph nodes; however, it might not be so difficult to distinguish metastatic hyperattenuated areas from calcification by monitoring the clinical course of each patient during a follow-up period.
Elective neck surgery can be performed to increase survival; however, such treatment remains controversial in patients with an early stage of tongue carcinoma (2–5). We suggest watchful observation instead of elective surgery to avoid unnecessary invasive procedures. However, watchful observation should be chosen over surgery only when follow-up imaging examinations can be performed carefully. We recommend performing repeated follow-up sonography at maximum intervals of 1 month, and, if possible, every 2 weeks (12).
Increased radiation exposure is the major disadvantage of adding non-contrast-enhanced CT at follow-up examination. At sonography, extended keratinization is correlated with a central echogenicity within lymph nodes (13). The major disadvantage of sonography, however, is a lack of definitive findings. We suggest that non-contrast-enhanced CT could be omitted during follow-up if careful, periodic sonography is performed. Further studies are needed to clarify the detectability of the keratinization by comparing non-contrast-enhanced CT and sonographic findings.
Conclusion
We have suggested that the non-contrast-enhanced CT finding of hyperattenuation within regional lymph nodes during a follow-up period might be an additional predictor of metastases, because hyperattenuation might be overlooked when only contrast-enhanced CT is used. Clinicians should be aware of the characteristic findings of non-contrast-enhanced as well as contrast-enhanced CT when investigating lymph node metastases at an early stage in patients with stage I or II tongue carcinoma during the follow-up period.
References
- Received October 30, 2001.
- Accepted after revision February 13, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.