
Abstract
BACKGROUND AND PURPOSE: Several approaches to the treatment of dissecting aneurysms of the vertebrobasilar system have been used. We evaluated our endovascular experience, which includes trapping and proximal occlusion.
METHODS: Thirty-five patients with intradural vertebrobasilar dissecting aneurysms presented to our institution between 1992 and 2002. Twenty-six were treated by endovascular means and two with surgery. In the endovascular group, 14 were in a supra-posterior inferior cerebellar artery (PICA) location, and three of these extended to the vertebrobasilar junction on the initial angiogram. Ten were located in an infra-PICA location, or no antegrade flow was seen in the PICA or anterior spinal artery. Two were located at the PICA with antegrade flow preserved in the branch. Twelve lesions were treated with trapping; another 14 were initially treated with proximal occlusion techniques, two of which eventually required trapping procedures. Follow-up images were obtained within 1 year of initial treatment in 24 patients. Mean follow-up for these patients was 3.5 years.
RESULTS: Initial treatments were technically successful and without complication in all 26 patients. Follow-up examinations showed complete cure in 19 of 24 patients. One patient died of global ischemia after presenting as Hunt and Hess grade 5 with subarachanoid hemorrhage. Two recurrent hemorrhages occurred in patients in the proximal occlusion group; one died, and the other underwent a trapping procedure. One patient developed contralateral vertebral dissection 24 hours after occlusion of a dissecting aneurysm of the dominant vertebral artery and died of a brain stem infarct. Another died of probable vasospasm, and the last died of an unknown cause 1 month after treatment. Two patients had recanalization despite an initial trapping procedure, both underwent further treatment. Mortality rate was 20% in the treated group (including the two patients treated surgically), with four of five deaths occurring during the initial hospital course. Mortality rate was 50% in the six patients in the untreated group who were available for follow-up.
CONCLUSION: Dissecting aneurysms of the vertebrobasilar system remain high-risk lesions because of their natural history. They can be managed by endovascular methods according to aneurysm location, configuration, collateral circulation, and time of presentation. Trapping results in better prevention of rehemorrhage. Proximal occlusion can achieve occlusion without manipulation of the affected segment when more direct endovascular occlusion or stent placement cannot be performed.
Dissecting aneurysms of the vertebrobasilar system are an uncommon but important cause of nontraumatic subarachnoid hemorrhage (SAH), accounting for 3–7% of these cases (1). Histologically, the intradural segment of the vertebral artery has a thin media and adventitia with fewer elastic fibers, so dissections of the intradural vertebral artery are more likely to result in SAH with pseuduoaneurysm compared with dissections of the extradural segment (1–5). Also, vasa vasorum are diminished (6), which may limit healing. Reported rates for recurrent hemorrhage from a dissecting vertebral artery aneurysm range from 30% to 70% (7, 8), with a high mortality rate estimated at 46% (8–10). Because of high rates of rebleeding, in most reported cases the patients have undergone surgical (5, 11–13) or endovascular therapy (13–15).
A variety of treatment strategies have been applied in small series of patients with dissecting vertebrobasilar aneurysms, including surgical reconstruction, surgical Hunterian ligation, wrapping, endovascular trapping, and various surgical bypass with occlusion strategies (5, 11–13, 16–18). Most reports have focused on a single treatment technique, procedural complications, and short-term outcomes.
The purpose of this study was to evaluate our hospital’s management of vertebrobasilar dissecting aneurysms with a multidisciplinary approach and treatment based on aneurysm location, configuration, and collateral circulation. Long-term outcomes also were reviewed.
Methods
We retrospectively reviewed the interventional neuroradiology and cerebrovascular surgery databases for 1992 through 2002 to identify patients referred for evaluation and treatment of dissecting aneurysms of the vertebrobasilar system. Only dissecting aneurysms involving the vertebral artery above C2 and/or the basilar trunk were included. No peripheral aneurysms of the posterior cerebral artery, anterior inferior cerebellar artery (AICA), superior cerebellar artery, or posterior inferior cerebellar artery (PICA) were included. Saccular berry aneurysms or atherosclerotic or fusiform aneurysms also were not included. Aneurysms were considered dissecting if one or both of the following conditions were met: 1) The aneurysm was associated with an intimal flap, or irregular or beaded parent arterial narrowing. 2) MR or CT confirmed a false lumen involving the parent artery. Medical and radiology records were reviewed and clinical information abstracted. Follow-up was determined by phone interview or from the most recent office note, and a modified Rankin score was assigned. Overall outcomes were defined as excellent, Rankin score 0–1; good, Rankin score 2; poor, Rankin score 3–4; or death, Rankin score 5.
Angiograms were assessed for size, shape, and location of the dissecting aneurysm with respect to the major branches and collaterals (ie, the presence or absence of the contralateral vertebral artery or posterior communicating arteries). Each lesion was examined for evidence of extension of the dissection into adjacent arterial segments, including the PICA and basilar artery. An attempt was made to identify perforator vessels and the anterior spinal artery. Each dissecting aneurysm was classified as follows: lesion inferior to the origin of the PICA, lesion involving the vertebral artery without antegrade filling of the PICA or anterior spinal artery visualized, lesion of the vertebral artery involving the PICA or anterior spinal artery with patency of this branch, lesion of the supra-PICA vertebral artery with or without extension into the vertebrobasilar junction, and lesion of the basilar artery.
Depending on the patient’s neurologic condition and stability, a balloon test occlusion was performed in a site to simulate best the anticipated therapeutic occlusion, without entering the dissected segment. Typically, the test occlusion was performed with a nondetachable balloon with concurrent neurologic testing but not a hypotensive challenge or ancillary imaging, for an occlusion time of 20–30 minutes. During the test occlusion, patients were systematically anticoagulated with intravenous heparin by using a standard protocol (19). Neurologic testing was performed throughout the procedure with the patient under monitored anesthesia. If patients remained at their neurologic baseline, and the follow-up angiogram demonstrated adequate collateral flow, permanent balloon occlusion of the affected artery was performed.
Endovascular treatment was based on the configuration of the dissecting aneurysm. Patients were considered for trapping of the dissecting aneurysm if the lesion did not incorporate a branch such as the AICA, PICA, or anterior spinal artery. This was accomplished with detachable silicon balloons or Guglielmi detachable coils (GDCs). If the dissected segment was deemed too risky to cross or too fusiform or narrow to accept coils, proximal occlusion was considered. Also, if the dissected segment incorporated important branches such as AICA, PICA, or anterior spinal artery, proximal occlusion was used. Lesions that extended to involve the vertebrobasilar junction were also treated by proximal occlusion. Materials used for these patients include GDC, Cordis, or Micrus coils. After occlusion, patients were monitored in the neurosurgical intensive care unit and treated for medical complications of SAH or stroke by using standard protocols. This included treatment for vasospasm with papavarine and/or balloon angioplasty in the appropriate setting.
Follow-up angiography, gadolinium-enhanced MR angiography, or CT angiography was performed at 6–12 months to determine whether the affected segment was smaller or healed. Further examinations were obtained yearly if needed.
Results
Twenty-eight of 35 patients with intradural vertebrobasilar dissecting aneurysms were treated, and the results are shown in Table 1. The demographics of the entire patient population (Tables 1 and 2) included 22 male and 13 female patients aged 17–87 years (mean, 52 years). At presentation, 29 patients had SAH, nine had thromboembolic or ischemic events, and one patient had headache (five patients had both SAH and ischemia). At the time of diagnosis, 13 aneurysms were categorized as infra-PICA or no antegrade PICA. There were five aneurysms involving the PICA with some antegrade flow, 16 supra-PICA aneurysms (four of which extended into the basilar artery on the initial angiogram), and one midbasilar dissecting aneurysm. Of the 34 lesions involving the vertebral arteries, eight involved the dominant vertebral artery, nine involved the nondominant vessel, and 17 occurred in a codominant vessel.
Treated dissecting aneurysms of the vertebrobasilar system
Untreated vertebrobasilar dissecting aneurysms
Seven of the 10 treated infra-PICA or no antegrade PICA aneurysms were treated with a trapping procedure, and the other three were treated with proximal occlusion. Two of the three treated PICA region vertebral dissecting aneurysms were initially managed with proximal occlusion, and one additional lesion was treated with clip reconstruction of a dominant vertebral artery preserving the PICA. Nine of the 14 treated supra-PICA dissecting aneurysms were managed with infra-PICA occlusions and five with trapping. The midbasilar dissecting aneurysm was treated with clip occlusion above the AICA vessels supported by collateral flow via the posterior communicating artery (20).
All arterial occlusions were technically successful. Posttreatment or follow-up angiograms showed complete cure in 19 of 24 aneurysms. Two recurrent hemorrhages occurred in patients treated with proximal occlusion. One of these patients died of the recurrent hemorrhage potentially associated with tissue plasminogen activator given through a blocked ventriculostomy catheter. The other patient underwent a trapping procedure as discussed below. Two of these patients showed recurrence or extension of their dissecting aneurysms despite initial trapping procedures. One underwent further GDC treatment, and one had PICA bypass and proximal vertebral artery occlusion. Patient 9 had extension of a contralateral vertebral dissection 24 hours after occlusion of the dominant vertebral artery and died of a brain stem infarct. Another death occurred in a patient who succumbed to global cortical injury from his initial grade 5 SAH. Another patient died of probable vasospasm, and the last patient died of an unknown cause 1 month after treatment.
Mean length of follow-up for the treated group was 3.5 years. Outcome of clinical follow-up available for 25 of the treated patients was excellent in 14, good in three, poor in three, and death in five. Mortality rate in the treated group was 20% versus 50% in the untreated group.
Seven patients did not undergo surgical exploration or endovascular embolization for one of several reasons (Table 2). Two patients died of recurrent SAH before an embolization procedure could be performed, whereas another died of severe head trauma. One patient had a stable lesion in a dominant vertebral artery. Two patients had spontaneous thrombosis of the dissecting aneurysm as confirmed by angiography and another declined treatment.
Cases
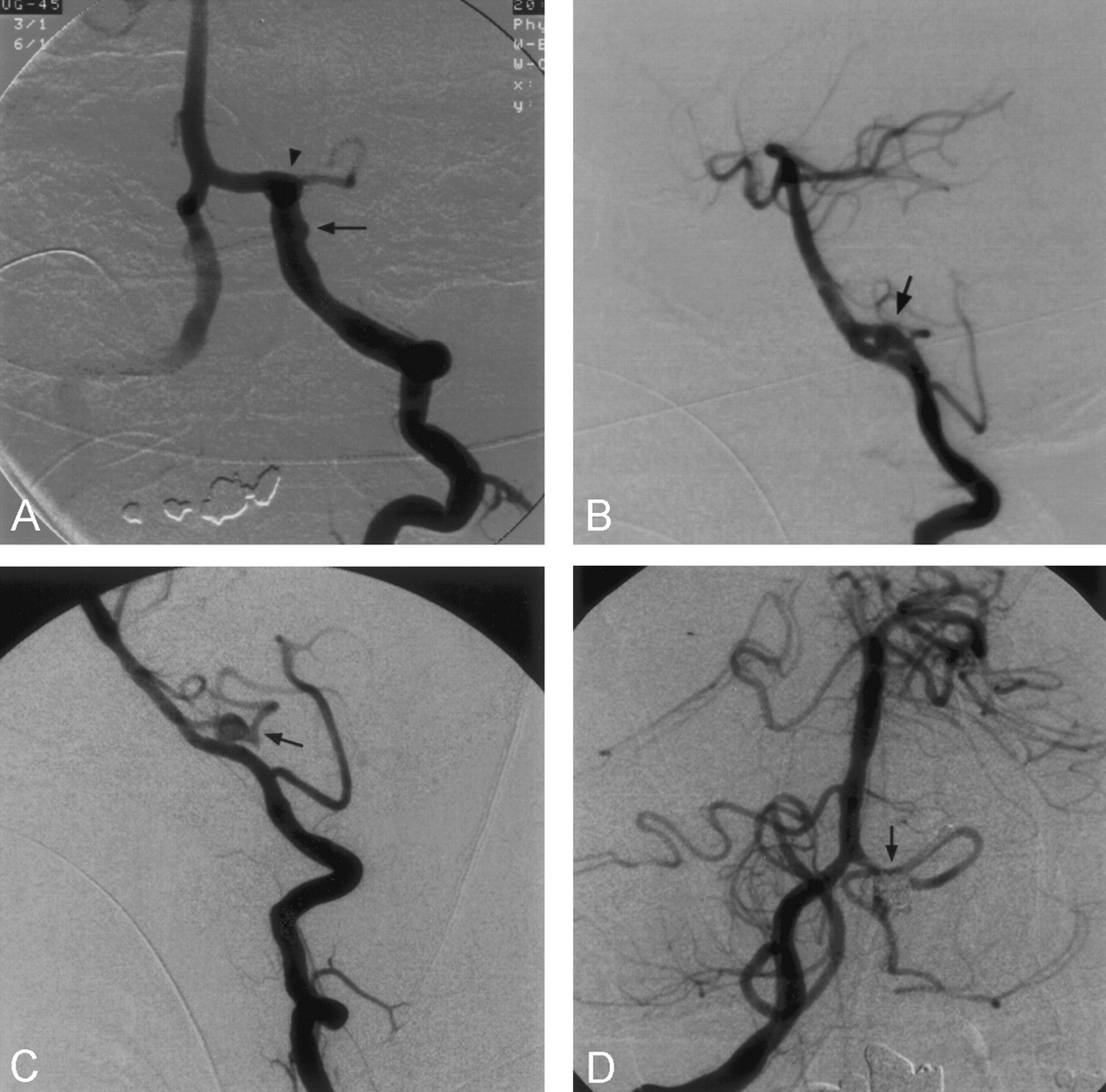
Patient 25 was a 41-year-old man who presented with acute onset of headache, nausea, and a syncopal episode. CT showed SAH in the prepontine cistern and in the lateral ventricles. Angiography revealed a dissecting aneurysm of the dominant left vertebral artery in the supra-PICA location (Fig 1A and B). There was extension to involve the basilar artery, as well as a pseudoaneurysm near the vertebrobasilar junction. Since there was good collateral flow through the left posterior communicating artery despite the right vertebral artery terminating in the right PICA, proximal balloon occlusion was performed on the left vertebral artery. Follow-up angiography (Fig 1C) demonstrated residual filling of the dissecting aneurysm and the left PICA with reversal of flow down the basilar artery. The patient was clinically stable for 2 years and then presented with episodes of headache and dizziness. CT and lumbar puncture were negative for subarachnoid blood, and MR imaging did not show evidence of infarct. The angiogram obtained at the time revealed occlusion of the dissecting aneurysm (Fig 1D). The left PICA was occluded proximally, but there was collateral supply in a retrograde pattern from the right PICA.

Patient 25.
A, Anteroposterior and B, lateral diagnostic angiograms demonstrate a dissecting aneurysm of the dominant left vertebral artery involving the supra-PICA segment and proximal basilar artery (arrow). Arrowhead indicates the pseudoaneurysm.
C, Lateral view of the left internal carotid artery injection shows good collateral circulation to the basilar artery (arrow) through the posterior communicating artery after proximal occlusion of the left vertebral artery. Arrowhead indicates the tip of the distal balloon.
D, Two-year follow-up left internal carotid artery angiogram in the lateral projection shows interval thrombosis of the pseudoaneurysm and dissected segment of the left vertebral artery. The basilar artery (arrow) appears less irregular.
Patient 27 was a 45-year-old man with a grade 3 SAH who received a diagnosis of supra-PICA dissecting aneurysm in the codominant left vertebral artery, which showed severe narrowing above the PICA and anterior spinal artery (Fig 2A). The lesion extended into the basilar trunk to incorporate the AICA vessels with a focal pseudoaneurysm at the vertebrobasilar junction (Fig 2B). The pseudoaneurysm was treated with coil embolization. The left vertebral artery was treated with proximal occlusion, since the entire lesion could not be trapped (Fig 2C). Care was taken to preserve the origins of the ipsilateral PICA and anterior spinal artery (Fig 2D).

Patient 27.
A, Anteroposterior angiogram of the left vertebral artery shows irregular narrowing of the supra-PICA segment (arrow) and a pseudoaneurysm at the vertebrobasilar junction (arrowhead). The anterior spinal artery and left PICA are not included in the abnormal segment.
B, Anteroposterior angiogram of the right vertebral artery shows a codominant vessel with full delineation of the vertebrobasilar junction pseudoaneurysm (arrowhead). The dissection extends in the basilar artery to include the AICA origins (arrow).
C, Posttreatment angiogram of the right vertebral artery shows coil occlusion of the vertebrobasilar junction pseudoaneurysm (arrowhead).
D, Posttreatment angiogram of the left vertebral artery shows proximal occlusion of the supra-PICA segment of the vessel with preservation of flow in the anterior spinal artery (arrow) and PICA.
Patient 11 was a 54-year-old man with a grade 2 SAH. Diagnostic angiography (Fig 3A and B) demonstrated a dissecting aneurysm involving the left PICA with antegrade filling of the vessel. The right vertebral artery was codominant, so proximal occlusion of the affected vessel was accomplished. Two detachable silicon balloons were placed in the left vertebral artery with reversal of flow across the vertebrobasilar junction. One week later, the patient had evidence of neurologic decline along with elevated trancranial Doppler sonograms; intraarterial papavarine administration and angioplasty of the supraclinoid internal carotid arteries and M1 segments bilaterally and the basilar artery and left P1 segment were required. However, 2 weeks after presentation, the patient had a second SAH confirmed with CT. Angiography showed the pseudoaneurysm was stable (Fig 3C). It was occluded by using GDCs with access gained across the vertebrobasilar junction (Fig 3D). Although the PICA filled slowly antegrade, a potential PICA infarct was decompressed by suboccipital craniectomy. Follow-up angiogram 4 months later showed no filling of the the supra-PICA segment or the pseudoaneurysm. The left PICA filled retrograde from collaterals.

Patient 11.
A, Anteroposterior angiogram of the left vertebral artery demonstrates irregularity of the lumen (arrow) and a 4–5-mm pseudoaneurysm (arrowhead) near the PICA origin.
B, Lateral angiogram of the left vertebral artery shows the small pseudoaneurysm (arrow).
C, Lateral angiogram of the right vertebral artery at the time of rehemorrhage 2 weeks after proximal occlusion of the left vertebral artery shows that the pseudoaneurysm (arrow) has not enlarged and the left PICA remains patent.
D, Anteroposterior angiogram of the right vertebral artery after delivery of coils across the vertebrobasilar junction into the pseudoaneurysm shows the lesion is occluded (arrow), with the PICA filling antegrade
Patient 22 was a 29-year-old woman with a grade 3 SAH. During initial angiography, she was found to have a supra-PICA dissecting aneurysm of the codominant left vertebral artery (Fig 4A). Control angiograms of the right and left vertebral arteries showed no residual aneurysm (Fig 4B and C). Angiography performed at day 3 to look for vasospasm was unchanged. However, follow-up angiography at 1 year showed recurrence or extension into the proximal left vertebral artery to the PICA region (Fig 4 D). A right-to-left PICA bypass was performed. The left vertebral artery was then trapped with GDCs.

Patient 22.
A, Anteroposterior angiogram of the right vertebral artery shows a dissection of this codominant vertebral artery (black arrow) and psuedoaneurysm (arrowhead). Note the fenestration in the basilar artery (white arrow).
B and C, Follow-up angiograms of the right (B) and left (C) vertebral arteries, respectively, show no residual aneurysm.
D, Follow-up angiogram 1 year later shows recurrence of the dissecting aneurysm (arrow) proximally in the left vertebral artery to involve the PICA. The coil mass has compacted (arrowhead).
Discussion
Dissecting aneurysms of the vertebrobasilar system are uncommon, but they must be distinguished from true aneurysms and simple dissections to enable proper treatment. Since the pathologic and radiographic appearance was first described by Yonas in 1977 (21), these lesions have been diagnosed with increasing frequency probably because of increasing awareness. Approximately 30–70% of patients with rupture will have rebleeding, while smaller percentages will stabilize or improve without treatment (5, 7, 8, 10, 12, 22). Our results demonstrate that treatment is indicated for most of these lesions. Mortality rate in the treated group was 20%, whereas that in the untreated group was 50%. There is likely a selection bias, since higher grade hemorrhages were seen more often in the untreated group. Natural history of spontaneous entrapment has been documented in a few cases in the literature (9, 23, 24) and was seen in two of our cases.
Symptoms of vertebrobasilar dissecting aneurysms depend on factors such as size and location, including whether the lesion is intradural or extadural. Typical presentations include SAH, thromboembolic events, and cranial neuropathy from mass effect. One review found that seven of 22 cases of Wallenberg syndrome (lateral medullary syndrome) were due to dissecting aneurysms of the vertebral artery (25). Cheiro-oral syndrome (26), hemifacial spasm (27), and Foville syndrome (brain stem infarct) (28) can all be related to vertebrobasilar dissecting aneurysms.
Most cases of dissecting aneurysm are idiopathic in origin, but numerous causes have been reported in the literature including trauma, hypertension, syphilis and other arteritides, fibromuscular dysplasia, and polyarteritis nodosa (29). Various pathologic findings have been reported, many of which indicate idiopathic medial necrosis (30). However, in a review of nine cases, Mizutani et al (3) indicate that injury to the intima was the predominant factor. They found that lesions could be categorized by whether the lesions have entrance only or entrance and exit through the intima communicating with the pseudoaneurysm. Entrance-only lesions appear to have a higher occurrence of rehemorrhage, suggesting that unrelieved pressure and pulsation have an adverse effect. One animal model suggests that chemical injury to the intima with lathrogens may lead to dissecting aneurysms in the aorta of rats (31, 32).
Angiography and immediate diagnosis are essential. The most common finding in our series was a pseudoaneurysm with irregular vessel lumen narrowing proximally. Treatment can be chosen after assessing location and configuration of the dissecting aneurysm, adjacent branches, collateral circulation, and time of presentation. Among patients at highest risk are those with lesions involving the dominant vertebral artery without adequate collateral circulation from the contralateral vertebral artery or posterior communicating arteries.
Results of multiple series (5, 11–15, 18) suggest surgical ligation or coil embolization to occlude directly the affected segment of artery as the appropriate therapy for vertebral artery dissecting aneurysms. In some instances, complicated and technically demanding surgical procedures have been required, such as saphenous or radial artery bypass (12) or PICA side-to-side reanastamosis (17). Vessel wrapping for intradural lesions was ineffective in the small number of documented cases (11, 16).
The most complete treatment of a dissecting aneurysm would be to exclude the segment with a trapping procedure. Although coil occlusion of the affected segment is one strategy, it poses the risk of occlusion of side branches, further injury to the vessel wall, or dislodging emboli. If the lesion extends to the basilar artery, only a segment may be coiled. Of 26 patients in our study who were treated by endovascular means, 12 were initially treated with the trapping technique. The procedures were successful and without complication. In two patients, lesions recurred and required further treatment. After treatment, one severe complication occurred that was related to extension of the dissecting aneurysm of the patient’s dominant right vertebral artery to the left vertebral artery with thrombosis of the basilar artery. Despite thrombolysis, the patient had a lethal brain stem stroke.
The alternative strategy of proximal occlusion limits the risk of catheter and wire manipulation across a narrow or irregular segment and may allow for better collateral circulation, especially when lesions involve the origin of the PICA or anterior spinal artery. It should also be considered for lesions with configurations unlikely to hold coils in a stable position. These include fusiform or wide-necked pseudoaneurysms. This strategy was initially used in 14 of our 26 endovascular cases. There were no extensions of dissection to the contralateral vertebral or basilar arteries resulting from treatment. However, there were two cases of rehemorrhage documented by CT. One patient died of a rebleed 1 week following proximal occlusion of a dissecting aneurysm. It is unclear whether this may have been related to tissue plasminogen activator used to clear the patient’s ventriculostomy catheter. In the other patient, rehemorrhage was a spontaneous event at 2 weeks after proximal occlusion. The dissecting aneurysm had not significantly enlarged, and the patient was successfully treated with a trapping procedure with access across the vertebrobasilar junction. Other deaths in this group included one patient who died in a delayed fashion of unknown cause, one patient who died of vasospasm, and a fourth who succumbed to global cortical injury related to his initial grade 5 SAH. Overall, these techniques may be an alternative when more direct endovascular techniques cannot be performed safely.
When patients present in a delayed time course, reevaluation with angiography is indicated. Specifically, one should look for extension of dissection, growth of the pseudoaneurysm, and vasospasm. Balloon test occlusion may be of benefit to determine if the collateral circulation is limited anatomically or compromised by vasospasm. These patients have undergone a physiologic test of time that may allow for a more inclusive set of treatment options, including embolization, neurosurgical bypass and trapping, combined procedures, or conservative close follow-up.
Follow-up for most cases should be performed at 12 months if the lesion is initially treated to complete obliteration. If the occlusion is stable, it is considered cured. If proximal occlusion was performed or there is residual filling at the time of initial therapy, 6-month follow-up could be considered. CT angiography can be used if balloon occlusion was performed and gadolinium-enhanced MR angiography can be used in many cases to follow treated lesions, but conventional angiography remains the definitive test.
Alternative methods of treatment for these dissecting aneurysms include trapping procedures with approaches that use proximal occlusion of the vertebral artery combined with distal occlusion across the vertebrobasilar junction to avoid the affected segment if the anatomy allows. Flexible intravascular stents followed by coil embolization of the pseudoaneurysm may be used to preserve the lumen especially if the dominant vertebral artery is affected. A group of seven dissecting aneurysms was treated with this method with no additional stroke or rehemorrhage (33). Risks of passing the device through the affected segment as well as injury at the edges of the stent would need to be considered.
Conclusion
Dissecting aneurysms of the vertebrobasilar circulation present challenging treatment issues. Categorization of lesions according to location, the dominant vertebral artery, collateral circulation, and adjacent branches is an important consideration. Trapping procedures with direct occlusion of the segment should be done when possible. This does not preclude the possibility of recurrence in our experience. Proximal occlusion techniques can be used to allow for collateral circulation, avoiding direct injury to the abnormal segment of artery but with a risk of rehemorrhage. Regardless of treatment choice, these patients need to be followed up closely.
Footnotes
Presented at the 37th annual meeting of the American Society of Neuroradiology, San Diego, 1999.
References
- Received March 21, 2002.
- Accepted after revision March 16, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Endovascular sacrifice of the proximal posterior inferior cerebellar artery for treatment of ruptured intracranial aneurysms
- Endovascular parent vessel sacrifice in ruptured dissecting vertebral and posterior inferior cerebellar artery aneurysms: clinical outcomes and review of the literature
- Republished: Monotherapy with stenting in subarachnoid hemorrhage (SAH) after middle cerebral artery dissection
- Elderly patients with intracranial aneurysms have higher quality of life after coil embolization: a decision analysis
- Deconstructive and Reconstructive Techniques in Treatment of Vertebrobasilar Dissecting Aneurysms: A Systematic Review and Meta-Analysis
- Monotherapy with stenting in subarachnoid hemorrhage (SAH) after middle cerebral artery dissection
- Natural Course of Dissecting Vertebrobasilar Artery Aneurysms without Stroke
- Safety of Unilateral Endovascular Occlusion of the Cervical Segment of the Vertebral Artery without Antecedent Balloon Test Occlusion
- Multiple overlapping stents as monotherapy in the treatment of 'blister' pseudoaneurysms arising from the supraclinoid internal carotid artery: a single institution series and review of the literature
- Subarachnoid haemorrhage with bilateral intracranial vertebral artery dissecting aneurysms treated by staged endovascular stenting
- Pipeline Embolization Device in Aneurysmal Subarachnoid Hemorrhage
- Novel use of Onyx for treatment of intracranial vertebral artery dissection
- Incidence and Risk Factors of Recurrence After Endovascular Treatment of Intracranial Vertebrobasilar Dissecting Aneurysms
- Reconstructive Endovascular Treatment of Intracranial Fusiform Aneurysms: A 1-Stage Procedure with Stent and Balloon
- Endovascular Strategies for Vertebrobasilar Dissecting Aneurysms
- Clinical and Angiographic Follow-Up of Stent-Only Therapy for Acute Intracranial Vertebrobasilar Dissecting Aneurysms
- Stent-Assisted Reconstructive Endovascular Repair of Cranial Fusiform Atherosclerotic and Dissecting Aneurysms: Long-Term Clinical and Angiographic Follow-Up
- Mechanically-induced proximal arterial occlusion and stent-within-a-stent technique for the treatment of bilateral vertebral artery dissecting aneurysms.