
Abstract
Summary: An 18-year-old female patient with unilateral hearing loss underwent evaluation with CT and MR imaging. A partially ossified, enhancing lesion in the bony labyrinth, with replacement of adjacent structures, was identified. Surgical biopsy revealed a meningioma arising primarily within the bony labyrinth. To our knowledge, this entity has not been previously described.
Meningiomas of the temporal bone can arise in various locations, with affected areas ranging from involvement of the cerebellopontine angle (CPA) cistern and internal auditory canal (IAC) to isolated involvement of the geniculate ganglion and middle ear (1–3). Although cases of inner-ear extension from IAC meningiomas have been reported (4–7), a meningioma arising primarily within the otic capsule has not been described, to our knowledge. This report describes a case of intralabyrinthine meningioma investigated with CT and MR imaging.
Case Report
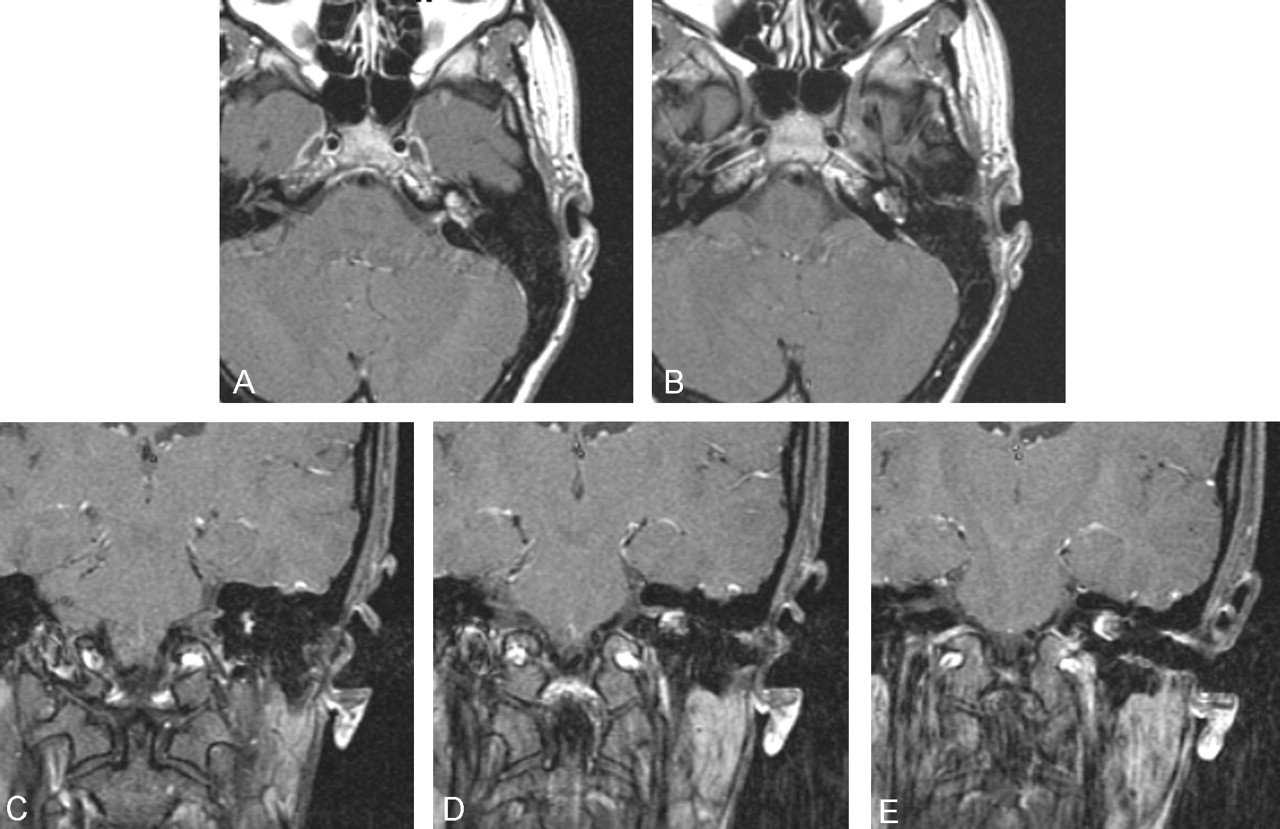
An 18-year-old female patient presented with complaints of tinnitus and subjective hearing loss involving the left ear. An audiogram was obtained at presentation and revealed mild sensorineural hearing loss on the left side. After a 4-month observation period, both her symptoms and audiographic findings were unchanged. Gadolinium-enhanced MR images of the temporal bones were then obtained. These demonstrated an enhancing lesion in the left bony labyrinth (Fig 1 and 2). High-resolution CT of the temporal bones was then performed to assess cochlear involvement. The lesion was shown to involve both the cochlea and the vestibule (Fig 3).

Dedicated thin-section, axial, T1-weighted (750/14/2/256 × 192/18 cm/2.5 mm/0.4 mm [TR/TE/NEX/matrix/FOV/section thickness/skip]) gadolinium-enhanced MR images show enhancement of the left labyrinthine lesion with minimal enhancement in the adjacent IAC.

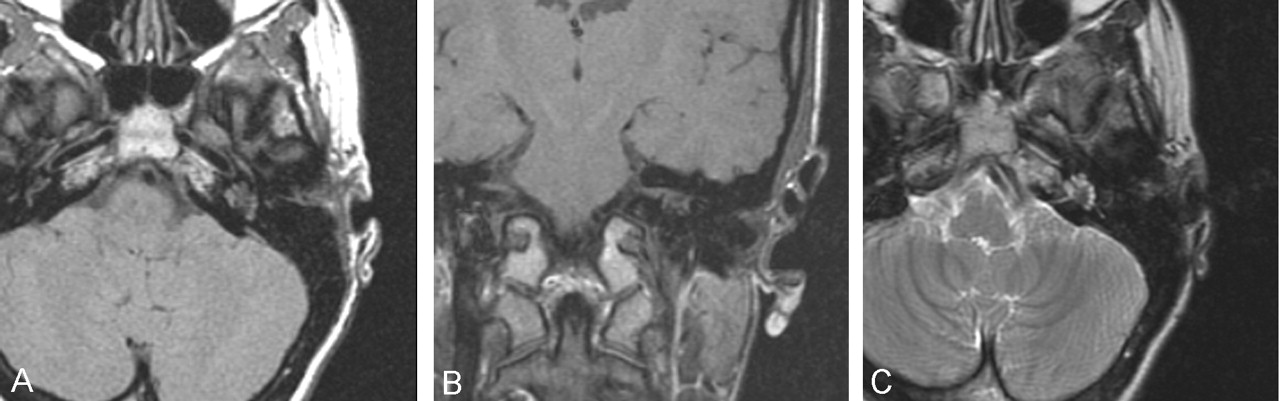
Dedicated thin-section axial (A) (750/14/2/256 × 192/18 cm/2.5 mm/0.4 mm [TR/TE/NEX/matrix/FOV/section thickness/skip]) and coronal (B) (600/14/2/256 × 192/18 cm/2.5 mm/0.4 mm) T1-weighted MR images obtained before gadolinium enhancement and axial fast spin-echo T2-weighted image (C) (5050/84/3/320 × 256/24 cm/5 mm/2.5 mm) demonstrate the labyrinthine mass, which is isointense to hypointense on both T1- and T2-weighted images.

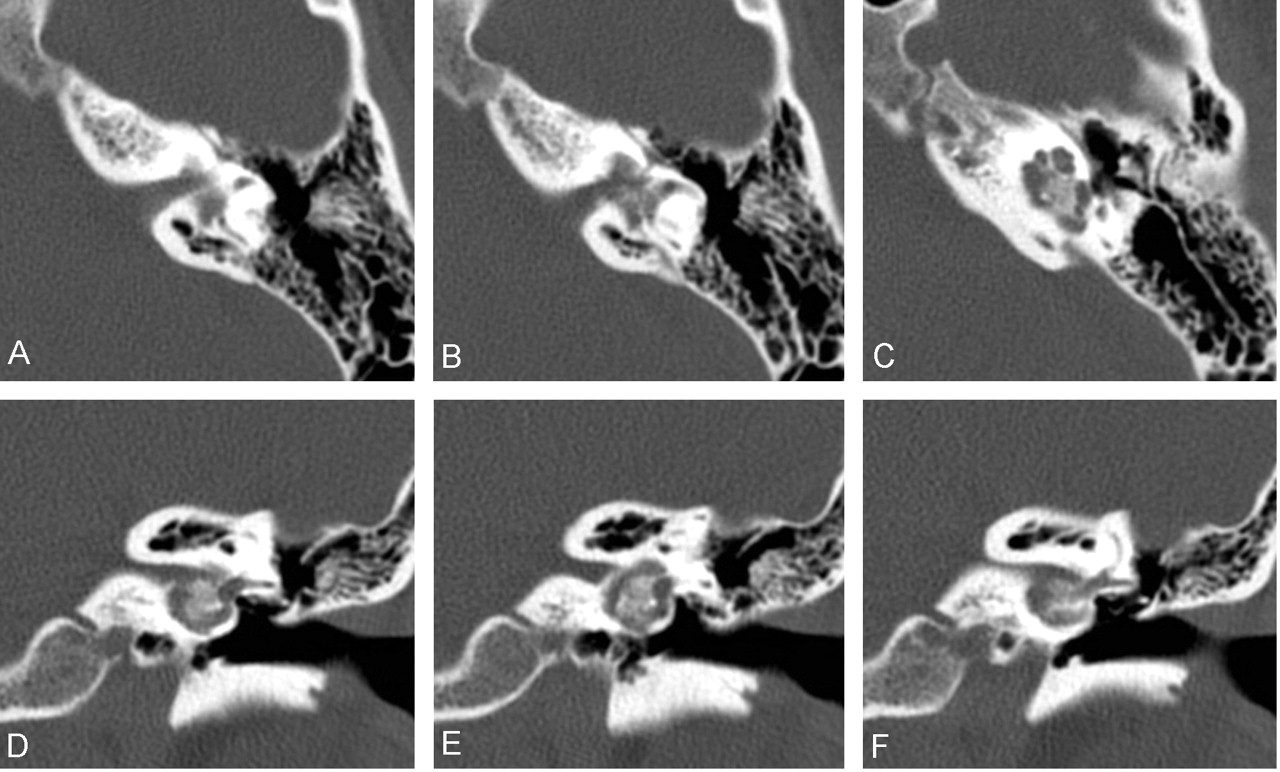
Direct axial (A–C) and coronal (D–F) 1-mm CT images of the left temporal bone obtained by using a bone algorithm. A partially ossified lesion, centered within the bony labyrinth, replaces the normal modiolus, vestibule, and basal turn of the cochlea. (1-mm section thickness, 512 × 512 matrix, 9.6-cm field of view, 9.6 cm/kV, 120/mAc 300).
Because the imaging results did not yield a definitive diagnosis, the patient was referred for surgical biopsy. Pathologic examination of the tissue yielded a diagnosis of meningioma. As complete sensorineural hearing loss was not yet present in the affected ear, complete resection was not performed at that time. When this report was written, the treatment plan was to follow up the patient with serial examinations until total hearing loss occurred or until significant growth of the lesion was observed.
Discussion
Differential Diagnosis
Our initial differential diagnosis centered on a vascular lesion (hemangioma) versus a chronic inflammatory or infectious process, although neither seemed completely consistent with the imaging findings.
Ossifying hemangioma, so named because of the spicules of new-bone formation within the tumor substance, was considered because of the osseous intratumoral matrix seen in the current case. However, the osseous component in this case was more homogeneous than that usually seen with an osseous hemangioma. Bony changes seen with a hemangioma in the surrounding bone have been described as having a honeycomb appearance (due to bony spicules) or as having a permeative pattern. The margins of these lesions are also characteristically indistinct (8). None of these features are present in the current case.
Intratemporal hemangiomas predominately occur in two areas—the geniculate ganglion and the fundus of the IAC—although a prior case report described primary adherence to and involvement of the vestibular nerve within the IAC (9, 10). The location of the current mass, within the bony labyrinth itself with little if any involvement of the IAC fundus, is not consistent with this diagnosis. Some reports describe extension of a hemangioma from the geniculate ganglion to involve the bone of the ampullary portions of the superior and the lateral semicircular canals, as well as the basal turn of the cochlea. However, the labyrinthine portion of the facial nerve and the geniculate ganglion were normal in our case (11).
Chronic inflammatory lesions of the labyrinthine structures may result in abnormally increased attenuation of the membranous labyrinth. Labyrinthitis ossificans may result from unresolved infection in the perilymphatic fluid, which leads to a fibrotic reaction due to the inflammation and subsequently ossifies. Most cases do not result in a tumefactive mass, but rather, increased attenuation of the labyrinthine structures.
Mulder et al (12) described three cases of a tumefactive fibroinflammatory lesion involving the inner ear, referred to as fibroinflammatory pseudotumor of the ear. Unlike our patient, all three of their patients presented with inflammatory involvement of the middle ear. Two of their patients had mild expansion and remodeling of the fundus of the IAC on CT examination. All three had findings of a soft-tissue mass, which replaced the normal labyrinthine structures. The inflammatory process predominantly involved the vestibule and central labyrinth, with less-severe involvement of the cochlea, similar to our case. The soft tissue enhanced after the intravenous administration of contrast material, simulating a neoplastic process. However, it did not demonstrate calcific or ossific attenuation, as it did in our case. The authors stated that the pathogenesis of this tumefactive fibroinflammatory process was unknown but also that it was likely related to different stimuli, especially chronic infection. Our patient had no evidence of middle-ear involvement and no history of an associated infectious or autoimmune illness that could be linked with labyrinthitis.
By definition, intralabyrinthine schwannomas arise in the labyrinth. However, their growth is confined by that part of the bony labyrinth from which they arise. Some bone expansion or remodeling may occur, but the lesions are not associated with bony destruction or ossification, a feature which eliminates them as a possible cause (13). A primary bone tumor such as an osteogenic sarcoma was believed to be unlikely in this case, partly because of the slow progression of symptoms. Metastatic disease to the inner ear occurs rarely, although the patient’s youth and the lack of a primary carcinoma did not suggest this diagnosis.
Intratemporal Meningioma
From an imaging standpoint, the characteristics of this tumor are well correlated with those of meningiomas seen in intracranial locations. That is, the tumor is isointense on T1-weighted images, isointense to hypointense on T2-weighted images, and homogeneously enhancing after the administration of a gadolinium-based agent. The tumors also demonstrate intratumoral ossification or an osseous matrix, along with remodeling of the adjacent bone.
The presence of ectopic meningiomas has been well documented in the literature, the most common location being the orbit (14). Proposed etiologies have centered on two hypotheses: Embryonal arachnoid cell rests may occur along the fusion lines of primitive bones and along cranial nerves (from whence meningiomas arise), and differential maturation of pluripotential mesenchymal cells may occur in these locations. Results of histopathologic studies have supported the former hypothesis, and studies to specifically evaluate the temporal bone have been performed (1, 2).
In a histologic review of 200 specimens of temporal bone, Guzowski et al (2) identified ectopic arachnoid cell rests at the petrous apex, the sulcus of the greater superficial petrosal nerve, and the impression of the trigeminal nerve. Arachnoid tissue, which does not represent a true arachnoid granulation, was found in the IAC, and arachnoid tissue was present in one temporal bone in the middle ear. In another study, Nager (1) found arachnoid granulations in the IAC, in the region of the geniculate ganglion, and in the jugular foramen. In several prior publications (3), isolated ectopic meningiomas have been described in the middle ear, as well as in the region of the geniculate ganglion, with no apparent spread from the intracranial compartment or IAC.
Psammoma bodies represent small, rounded concretions and are thought to arise from arachnoid cell rests within the brain and cranial nerve sheaths. These bodies may provide additional information about where meningiomas could arise within the temporal bone. The distribution of psammoma bodies in 27 temporal-bone specimens were evaluated in an autopsy study (15). The distribution of these concretions within the IAC, specifically in relation to the seventh and eighth cranial nerves and their divisions, was described. Psammoma bodies were identified as involving all cranial-nerve divisions within the region, with the largest overall number within the fundus of the IAC. Psammoma bodies were identified within the singular canal around the ampullary nerve (a branch of the inferior vestibular nerve) and around the labyrinthine portion of the facial nerve. Psammoma bodies were not identified lateral to the lamina cribosa or along the tympanic segment of the facial nerve.
A review of the literature revealed cases of possible intralabyrinthine meningiomas in which the origin of the lesion was either unknown or represented extension from the adjacent IAC. In one case report from 1980 (4), investigators described a 2-mm meningioma located in the ampulla of the posterior semicircular canal. The mass was incidentally diagnosed at pathologic evaluation after total labyrinthectomy had been performed. Contrast-enhanced CT scans of the temporal bone were reportedly normal. This same patient later underwent myelography of the posterior fossa to identify a mass in the IAC, which was later determined to be a meningioma in the CPA cistern and IAC on the same side. The authors assumed that the 2-mm lesion in the ampulla of the posterior semicircular canal represented intralabyrinthine extension of the IAC meningioma. The interval between initial surgery and the subsequent finding of the IAC and CPA mass at myelography is not clear. Since psammoma bodies were found around the region of the ampullary nerve, it is conceivable that the initial meningioma arose within the ampullary region of the posterior semicircular canal and that the IAC-CPA tumor represented a recurrence.
An additional case review of intratemporal meningiomas describes an IAC meningioma with involvement of the inner ear, but it does not elaborate on the structures involved or provide any images (5). In more recent case reports, Asaoka et al (6) and Ishikawa et al (7) describe intralabyrinthine extensions from IAC meningiomas, the latter case involving abnormal enhancement in the inner ear on preoperative imaging. In that case, the vestibular component appeared to be separated from the IAC component at surgery. The components may have been separate lesions, although this finding was not stated with certainty.
Conclusion
In this report, we illustrate the unusual case of a meningioma arising from, or at least centered within, the bony labyrinth. Although histologic investigations have not demonstrated arachnoid cells in the region of the cochlea or vestibule, we suspect that it is possible to have aberrant arachnoid tissue along small branches of the nerves supplying the inner ear. This may be the origin of the meningioma in our case. An origin from the distal aspect of the ampullary nerve within the bony labyrinth is also a possibility, given the presence of psammoma bodies in this location and the mentioned case report. Given the minimal enhancement seen on the gadolinium-enhanced MR images within the IAC, primary growth of this lesion into the bony labyrinth from an origin in the fundus of the IAC also remains a possibility. Future surgical resection of this lesion will hopefully assist in elucidating its true origin.
Acknowledgments
We would like to acknowledge D. E. Brackmann, who performed the surgical biopsy at the St. Vincent Medical Center in Los Angeles. We would also like to acknowledge Drs Donald L. Tschirart and Sandy S. Wu, who performed the pathologic analysis.
References
- Received December 6, 2002.
- Accepted after revision March 11, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.