
It has been 10 years since percutaneous vertebroplasty (PV) was introduced clinically into the United States. The procedure has grown in acceptance and is becoming the standard of care for pain associated with compression fractures of the spine (1). It has proved effective for this purpose and is generally safe when used by well-trained and prudent physicians. We have learned of many pitfalls along the way, and students and physicians can learn from these lessons early in their careers to avoid complications and bad outcomes. This article will focus on 1) the avoidance of complications, 2) the optimization of procedure technique, and 3) the application of PV to difficult case situations.
Complication Avoidance
Fortunately, complications with PV (Table 1) have been for the most part uncommon. Awareness of the potential for complications and attention to detail will allow one to avoid these in most circumstances.
Vertebroplasty complications
Cement Leaks
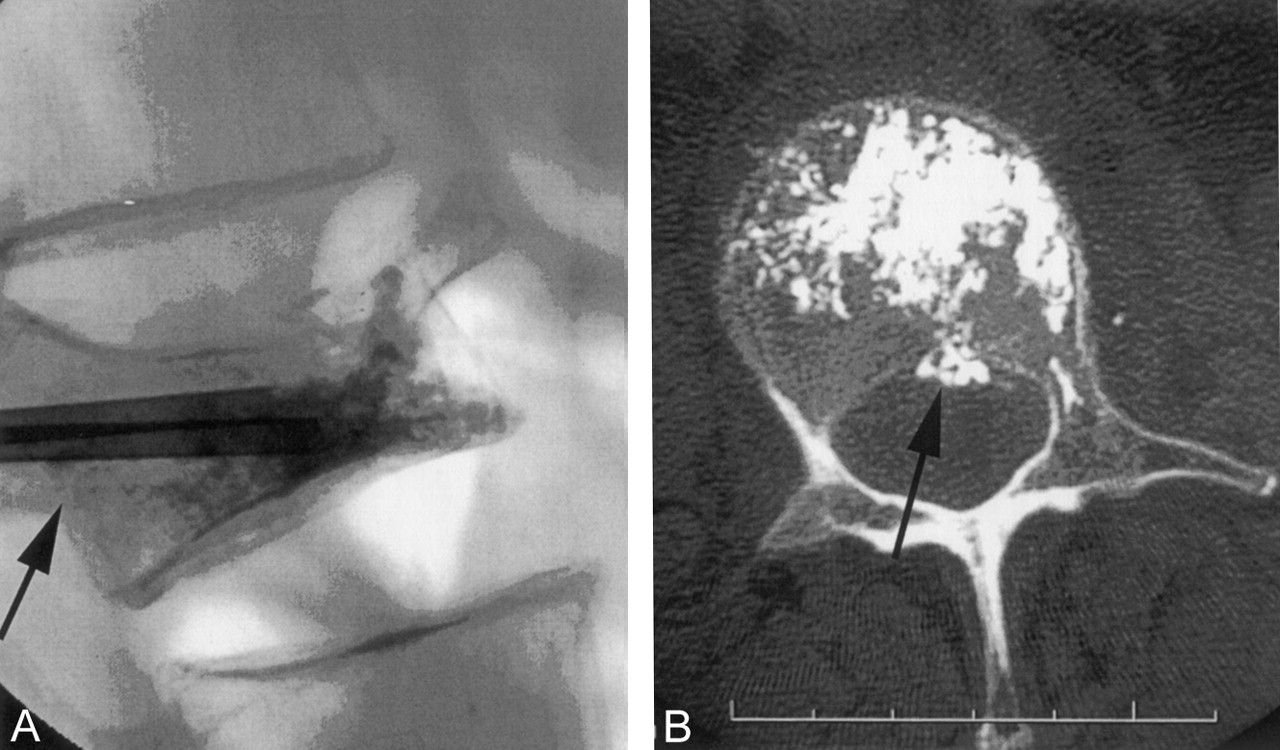
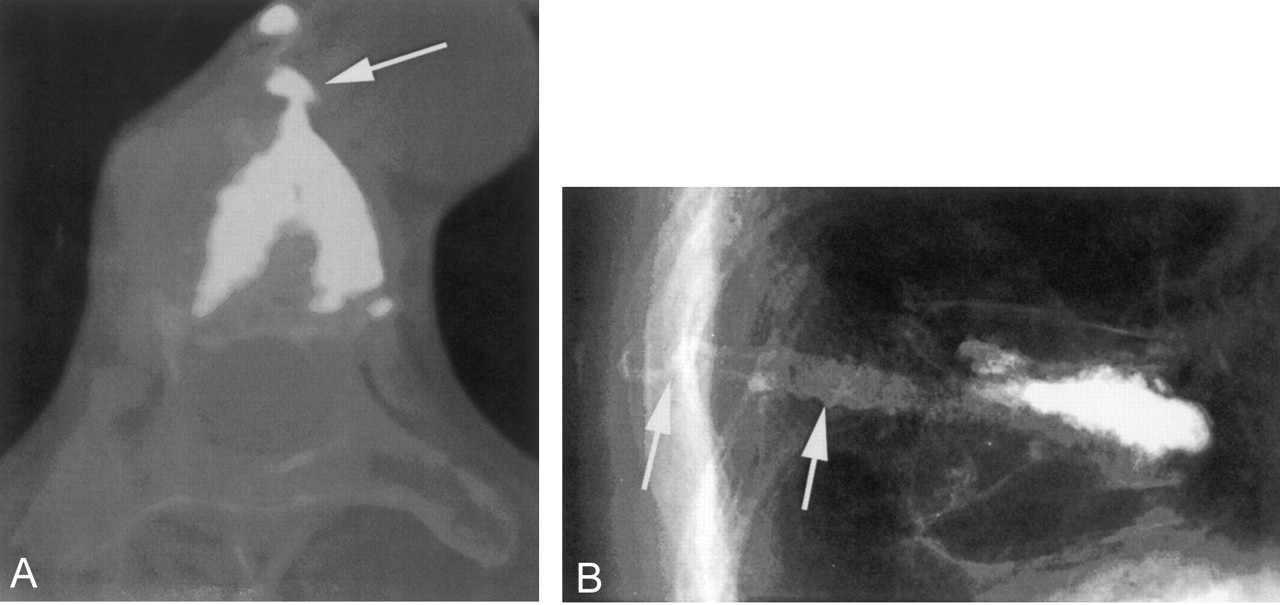
Without question, cement leaks account for most of the symptomatic complications resulting from PV (1–3). When treating osteoporotic compression fractures, symptomatic complications are expected less than 1% of the time. This increases to 2–5% when osteolytic metastatic disease is treated (1). In both clinical situations, the resultant complications are most often associated with cement leakage from the vertebra and its subsequent compression of adjacent neurologic structures or embolic effects on the lungs. Cement leaks may be seen in 5–15% of routine cases. These leaks are generally small and are usually of no clinical consequence (Fig 1). This is the case regardless of the location of the leak. In healthy individuals, the lungs will tolerate small emboli without symptoms (Fig 2). A large cement leak, however, can cause a pulmonary infarct and multiple emboli may lead to pulmonary compromise or even death (4).

A, Lateral radiograph during vertebroplasty showing cement extending to the posterior vertebral margin (black arrow).
B, Post-PV CT scan demonstrates a small leak into the epidural venous plexus (black arrow). This leak was asymptomatic.

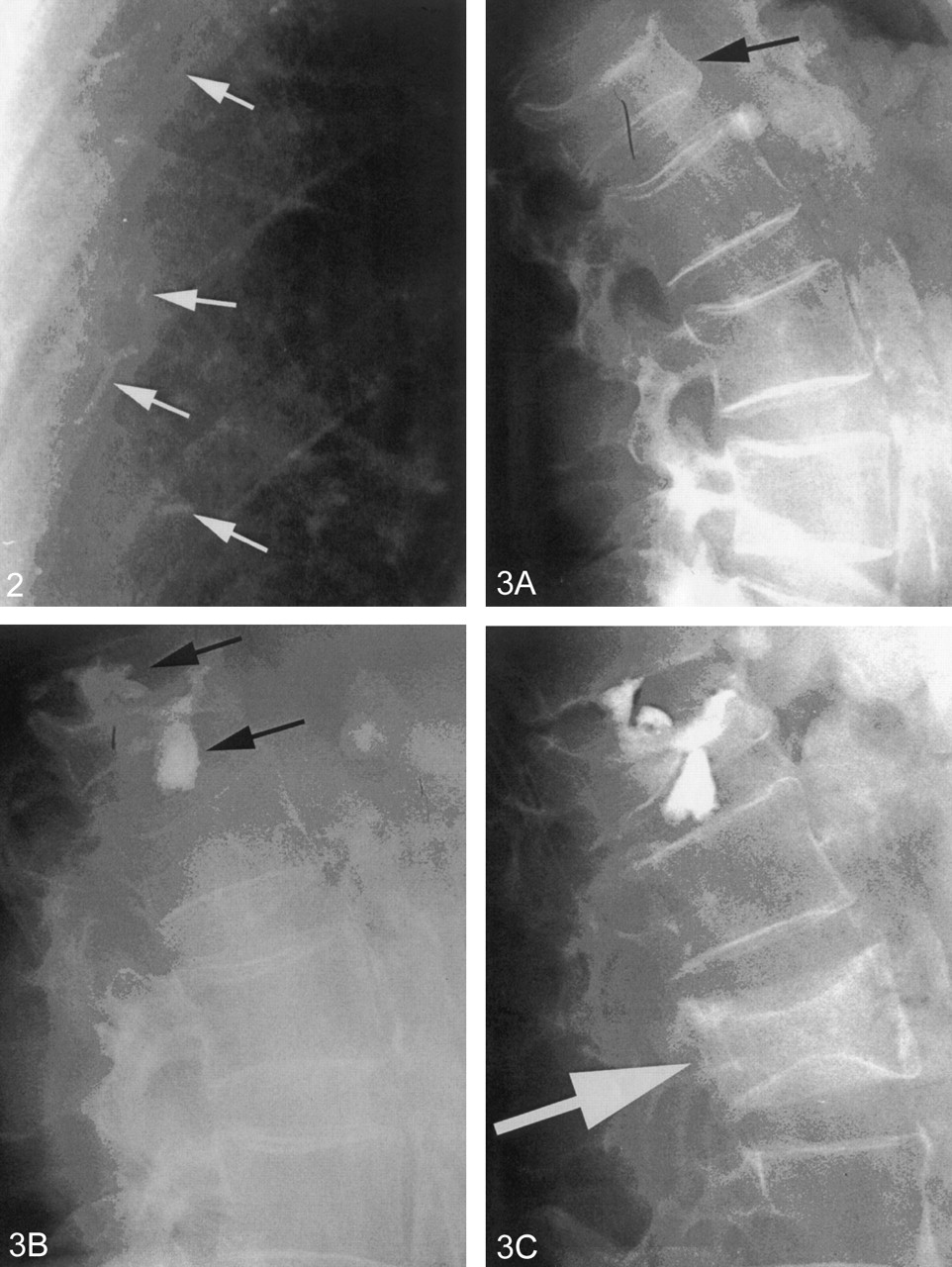
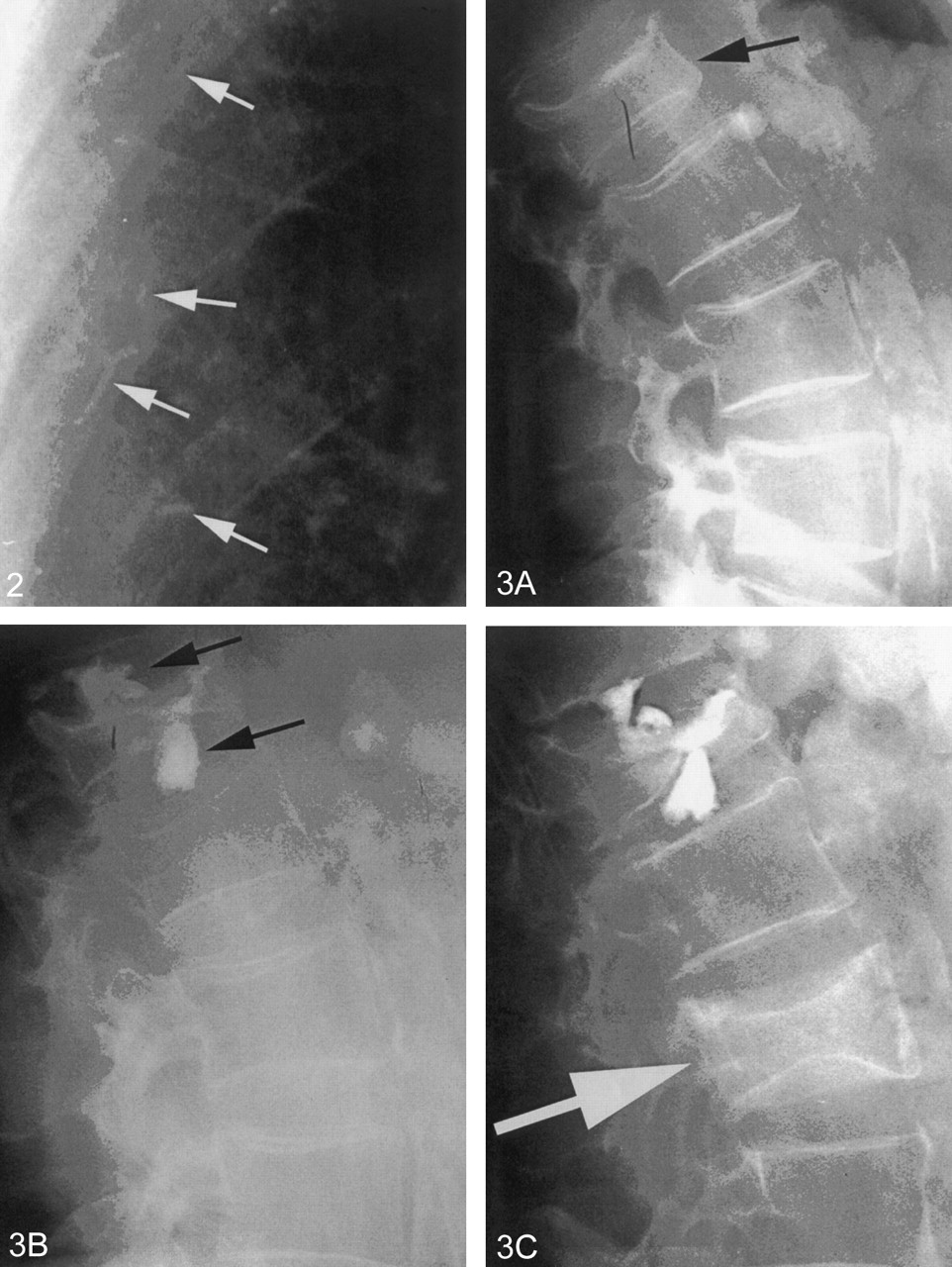
Portion of a chest radiograph after PV showing small radiopaque cement emboli (white arrows) in peripheral pulmonary vessels. This patient had no pulmonary symptoms.
Cement can also leak into the disk space. This accounts for 25% or more of the total leaks. These are not of consequence if small. There has been speculation that large disk leaks may predispose the adjacent vertebra to collapse. This has not been proved, however, and I have not seen this effect in my practice. Figure 3 demonstrates a subsequent fracture that occurred away from a large disk leak. If a cement leak into the disk predisposes to an adjacent fracture, the statistical confirmation will be hard to obtain, because adjacent-level fractures after PV are known to occur without leak (5, 6).

A, Lateral radiograph of the spine showing a moderately compressed vertebra (black arrow).
B, Postvertebroplasty, there are large leaks of cement (black arrows) into the adjacent disk spaces.
C, Six months later, the patient returned with a second fracture (white arrow). This fracture is not an adjacent level. Adjacent levels did not fracture despite the large disk leaks.
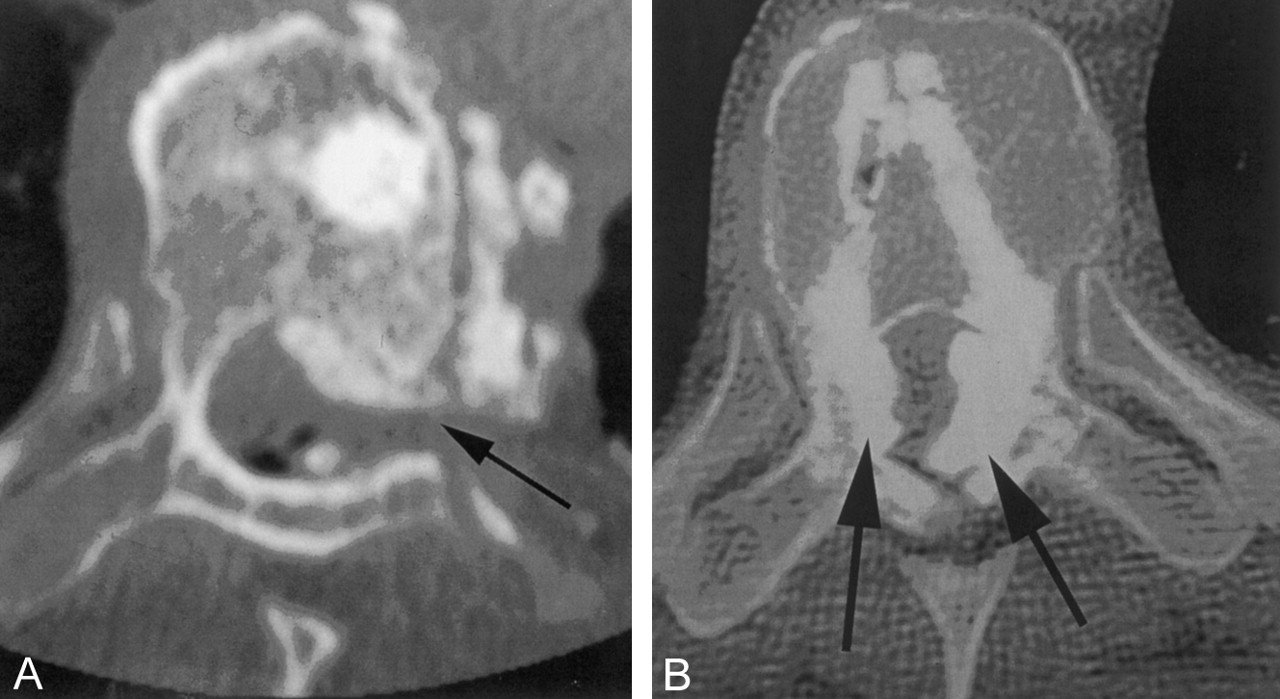
The most common consequence of a severe symptomatic cement leak occurs locally, producing nerve root irritation (resulting in radiculopathy) or cord compression (resulting in myelopathy) (Fig 4). Nerve root irritation may be transient and treatable with nonsteroidal anti-inflammatory drugs or local steroid injections. Persistent pain, however, may require surgical removal of the cement. Cord compression may result in paresis or paralysis. Serious and permanent complications have occurred with both PV and balloon-assisted PV (kyphoplasty; Fig 4). Substantial local cement leaks may also result in local pain exacerbation (7; Fig 5). With any worsening of the clinical situation, a CT scan should be obtained to assess the size and location of a suspected cement leak. A neurologic deficit should trigger an immediate neurosurgical consult. Severe cord compression (resulting in paralysis) and death due to respiratory compromise (caused by large cement pulmonary emboli) have occurred. These complications should be rare or nonexistent and generally result from poor operator technique.

A, Postvertebroplasty CT scan demonstrates large cement leaks into the spinal canal, neural foramin (black arrow), and perispinus region. This patient had paresis and radiculopathy.
B, Postkyphoplasty CT scan shows large leaks into the spinal canal (black arrows), which created paraplegia.

A, Postkyphoplasty CT scan. The lateral wall was disrupted by the balloon inflation, and a large cement leak into the mediastinum resulted (white arrow). For weeks following the procedure, this patient had severe, persistent pain.
B, Lateral radiography after vertebroplasty with a slow-set PMMA. The needles were withdrawn and the cement was still liquid enough to flow into the needle tracts and into the soft tissue (white arrows). This created local discomfort to pressure.
One may prevent substantial cement leaks by using 1) high-resolution fluoroscopy (or rarely CT), 2) adequate cement opacification, and 3) interrupting or terminating the cement injection on first recognition of a leak. Modern fluoroscopic equipment generally has adequate capability for the average PV case. Heavy individuals, severe osteoporosis, osteolytic destruction of the vertebra, and anatomic locations that preclude good visualization (eg, high thoracic vertebra obscured by the shoulders in the lateral projection) may warrant the use of other imaging techniques such as combined CT and fluoroscopic guidance. Biplane fluoroscopy is not a necessity for PV, but it does make visualization in two projections simpler and faster (1). One must visualize the treated vertebra from two projections numerous times during the procedure regardless of whether single or biplane fluoroscopy is used.
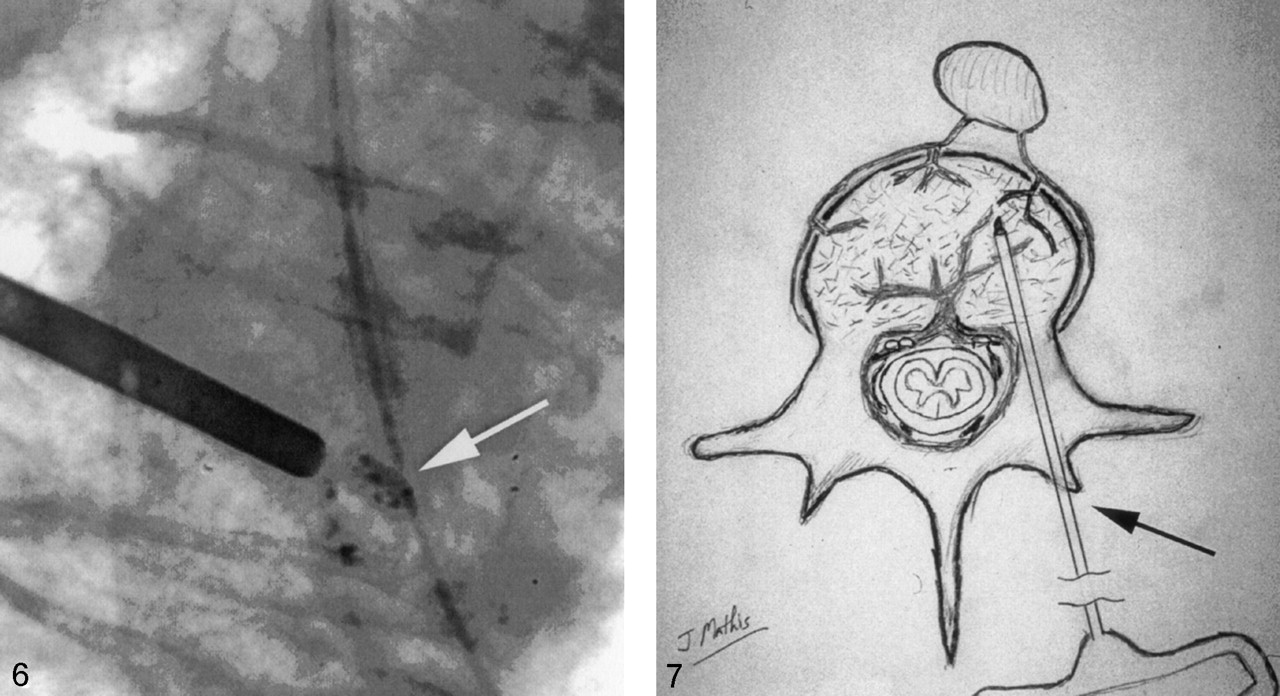
Good cement opacification is also crucial to being able to recognize an early cement leak while it is small. Because there is presently no cement specifically made and optimized for PV in the United States, the addition of an opacification agent is required. In the United States, the opacification agent of choice has been barium sulfate. Sterile barium sulfate is added to bring the barium quantity to 30% by weight (8, 9). This allows one to see adequately even small quantities of cement during fluoroscopy (Fig 6).

Radiograph showing appropriately opacified cement (white arrow) that can be easily seen even in very small quantities.
With high-resolution fluoroscopy and adequate cement opacification, one can see early leaks and interrupt or terminate a problematic cement injection. Early termination of the injection will limit the size of the leak and usually prevents it from becoming significant. Venography, originally touted as helping to predict leaks, is generally no longer a routine part of the PV procedure (10, 11). It has been recognized that venography does not accurately predict the path of cement because of the marked difference in the flow characteristics of radiographic contrast material used for venography and bone cement (9). PV has been performed in large numbers of patients without venography with no increase in risk or complication (10). It is not a routine part of most busy practices today.
Pain Exacerbation
An idiopathic pain flare or pain increase can uncommonly be seen following PV without an associated cement leak or hematoma (7). This occurs immediately after the procedure and may require narcotic analgesics for control. As with any complication or untoward result, a CT scan should be immediately obtained to ensure that there is no mechanical cause for the pain (eg, leak into neural foramina and nerve root compression). The etiology of this idiopathic pain may be local ischemia or increased pressure in the intertrabecular space during injection. If the CT shows no leak, however, the pain can be expected to be self-limiting, with resolution occurring within a few hours.
Infection
Infection following PV has been rare, with only one case reported in the medical literature (12). As with any surgically implanted device (in this case, bone cement), it seems prudent to administer intravenous antibiotics immediately before PV. A common choice is 1 g of cephazolin. The low incidence of infection generally does not warrant adding antibiotic to the bone cement. Whereas this practice was found beneficial in immunocompromised hip-replacement patients (13), in patients with a normal immune system the added expense and resultant alteration of the mechanical properties of the cement outweigh the benefits.
Bleeding
Venous bleeding after PV can be substantial along the needle tracts (following needle removal); however, local pressure for 3–5 minutes will minimize subcutaneous hematoma and local tenderness following the procedure. Patients with a coagulopathy or receiving anticoagulation medication (especially with coumadin) should have bleeding abnormalities corrected before PV (9).
The transpedicular approach places the needle entry site into the bone along the dorsal aspect of the vertebral posterior element and in a position easily compressed with local skin pressure (Fig 7). This approach, therefore, offers the greatest margin of safety for being able to control local bleeding easily. Parapedicular and posterior-lateral approaches place the needle entry site more laterally and may make hemostasis with local pressure more problematic.

Drawing depicting the needle entry site into the bone (black arrow) for a transpedicular approach. Following removal of the needle, local pressure allows one to easily achieve hemostasis in this situation.
Technique Optimization
As already discussed, high-quality imaging equipment and appropriate cement opacification are a basic requirement to successful and safe PV. Additional issues should be observed, as well, to refine the procedure to the fullest extent.
Patient Comfort
Modern PV is almost always performed in patients who are awake and must lie prone on the radiographic or operative table for 30–60 minutes. Patient comfort on the table is therefore an essential preparatory requirement. This may be accomplished by providing added padding to the table and by using arm supports that position the arms comfortably for a prolonged period (9).
Conscious sedation is commonly employed during PV, by using a combination of fentanyl (Sublimase; Abbott Labs, Chicago, IL) and midazolam (Versed; Roche, Manati, PR), titrated to the individual patient’s needs (1, 9). Many elderly patients have comorbidities (such as cardiac and pulmonary disease) that increase their risk with heavy conscious sedation. Judicious use of local anesthetics can reduce (and in some cases eliminate) the need for intravenous sedation. This requires that local anesthetics be used in adequate quantities and injected into the skin, subcutaneous tissue, and periosteoum of the bone at the needle entry sites. It is well known that a reduction in the discomfort associated with the introduction of the local anesthetic is obtained by mixing the anesthetic with bicarbonate. The resultant mix is still substantially painful. A “no-sting” mix is available (Table 2) and is recommended. It is used in our department for all procedures requiring a local anesthetic.
“No-Sting” Anesthetic Mixture
Needle Technique
It has been established that adequate biomechanical augmentation of a compressed vertebra can be obtained with a single-needle introductory system as long as the cement fill crosses the midline (14). This technique has been used clinically with success with an adequate fill obtained approximately 70% of the time with a single needle. The single-needle technique, however, fails often enough that I still teach and recommend a two-needle technique for the routine PV, especially for the less-experienced operator. Placing a second needle takes only an additional 3–5 minutes and allows much more flexibility during the cement injection. If a less than optimum cement spread or cement leak is experienced, the operator can move to the second needle and finish the injection without having to mix cement a second time. When using a single needle, less optimum cement fills and larger leaks are tolerated while trying to finish the procedure through the one cannula.
Cement Selection
All PV cases are presently performed with polymethylmethacrylate (PMMA) as the bone cement. Several types of cement are available, although no cement is presently approved for use specifically for PV in the United States. PMMA cements fall into two general categories: rapid set (eg, Simplex P; Howmedica, Rutherford, NJ) or slow set (eg, Cranioplastic; DePuy, Blackpool, England) types. Most inexperienced operators initially feel more comfortable by using the slow-set varieties, because these materials allow more working time of the cement at room temperature; however, the rapid-set materials offer definite advantages that quickly surface as one experiences the inevitable cement leaks common with this procedure. When a leak occurs while using a rapid-set cement, waiting only 1–2 minutes will usually allow sufficient polymerization of the injected cement to plug the leak and allow additional cement to be injected safely. This is less often the case with the slow-set material. Also, the slow-set cements stay liquid longer in the body and therefore retain their potential for leak longer (Fig 5), even along the needle tract if the needle is removed too soon. If CT guidance is elected, the slow-set material is advantageous, because the procedure is usually prolonged compared with PV with fluoroscopic guidance. Experience with both cements can be a definite advantage, and appropriate selection can simplify certain difficult situations.
Difficult Case Situations
Dealing with difficult or complex-case situations also falls under the general heading of technique optimization. Apart from the techniques used for the routine PV case, there are technical considerations that will aid these special situations that are more difficult or have specific potential pitfalls. These case situations will be dealt with individually in this section.
Clefts and Cavities.—
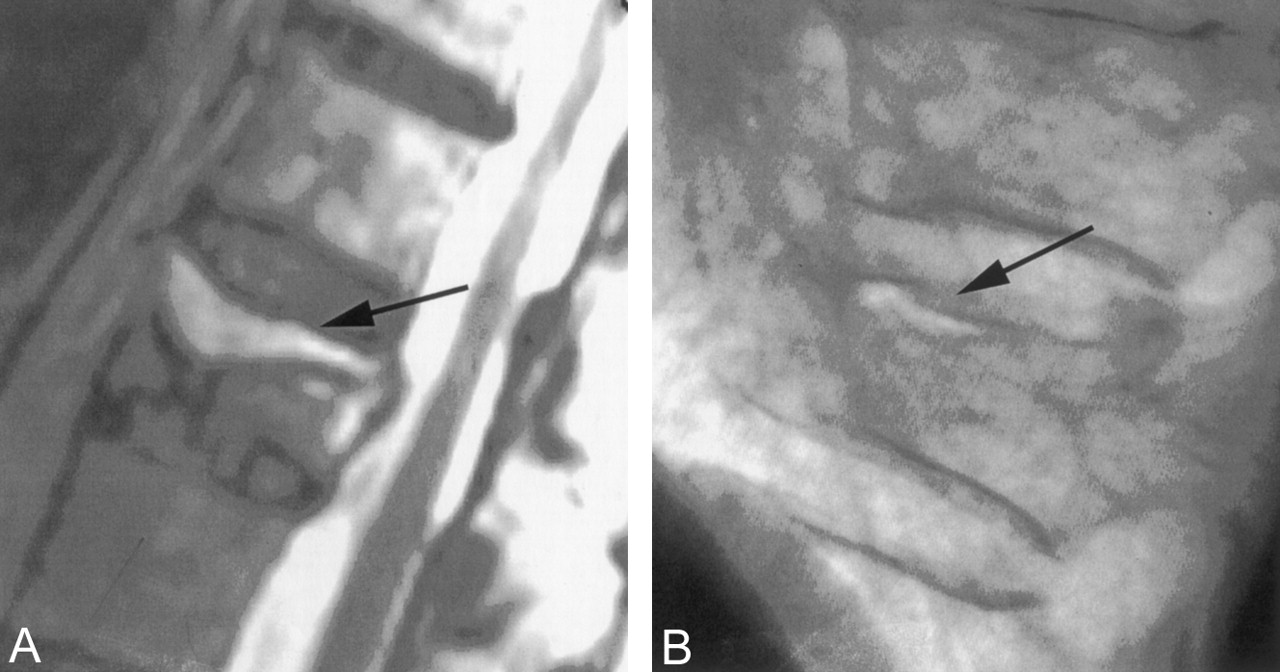
Cavities in the vertebral body can form as a result of compression trauma. These areas are often seen on MR imaging (T2 weighting) as bright bands below the endplate (Fig 8A; 15, 16). These cavities are fluid-filled spaces that probably result from local rebound of the endplate following compression, leaving a space that ultimately fills with air or fluid. When filled with air, this cavity (or cleft) can be seen fluoroscopically or radiographically (Fig 8B). These clefts may be an indication of nonunion of the bone and can demonstrate movement of the bone with change in patient position or respiration (17). This motion can be responsible for persistent (or permanent) pain lasting many months after the actual fracture. To treat these fractures adequately, the cavity must be completely filled with bone cement. Fortunately, this is usually easy to accomplish, because the cement often seeks the cavity preferentially, regardless of position of the needle tip (Fig 9). This pathologic situation also presents an excellent opportunity to achieve some vertebral height restoration during the PV procedure (Fig 10; 18); however, the important point here is that the cleft or cavity must be sufficiently filled to prevent future motion. With this accomplished, these cavities are dependably good responders for pain relief after PV.

A, T2 sagittal MR imaging demonstrating a high signal intensity collection (black arrow) below the superior endplate of this compressed vertebra. This represents a fluid-filled vertebral cleft.
B, Lateral radiograph showing an air-filled cleft (black arrow) in a compression fracture.

A, Lateral radiograph showing early cement filling of a cleft below the superior endplate (black arrow) of a compressed vertebra. Note that the needle tips are separated from the cleft and the cleft is filling preferentially.
B, Anterioposterior view of the same vertebra at completion of the vertebroplasty. The cleft (black arrow) has been completely filled with cement. Relatively little cement has been deposited into the rest of the vertebra. This typically results in good pain relief without the need for repeat filling of the noncleft portion of the vertebra.

A, Lateral radiograph demonstrating marked compression of a lower thoracic vertebra. Note the 18° of kyphosis before vertebroplasty.
B, With mild extension of the body, some height was restored to vertebra during vertebroplasty. This postvertebroplasty image shows that the kyphosis has been reduced to 9°.
Osteolytic Metastases.—
Destructive metastatic lesions can present some of the most challenging and complication-prone problems that will be faced during a PV. Osteolytic metastatic involvement, almost by definition, creates destruction of the vertebra and produces a situation where cement leaks are very possible (2, 3). It is not just the possibility of cement leaking into the spinal canal that carries risk. Tumor may be displaced into the canal, even without leak of cement, and this can also create cord or nerve root compression (19). It is generally not a good idea to attempt PV if there is already extension of tumor into the spinal canal.
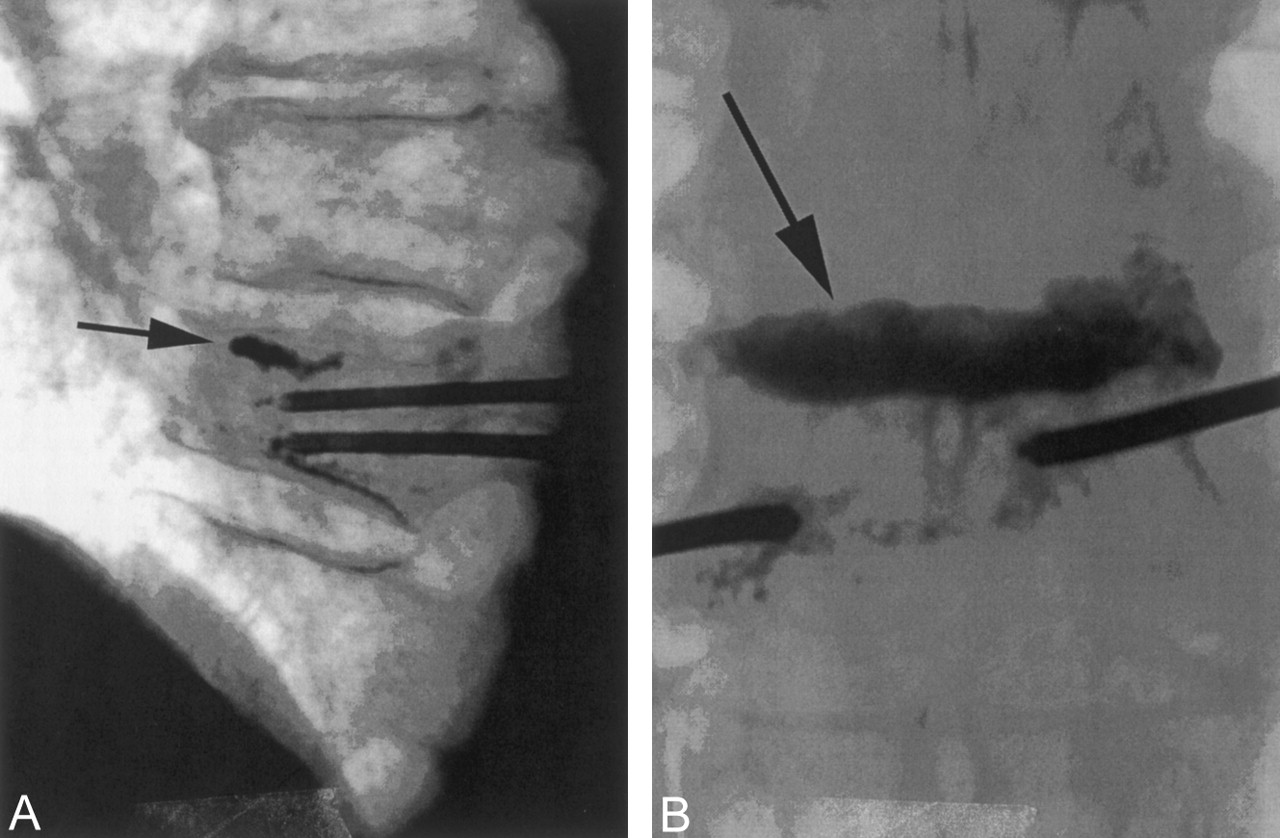
To monitor the effect of the cement injection on the spinal canal and neural elements, one may mark the thecal sac by introducing myelographic contrast before the PV. In the lumbar area it is easy to capture the contrast and still use fluoroscopic guidance during the cement injection (Fig 11A). In the thoracic and cervical areas, however, CT becomes very effective for monitoring the injection and looking for cement or tumor that may be displaced into the canal (Fig 11B). CT does not allow easy real-time monitoring of the cement injection, but by using slow-set cement, one can inject small aliquots of cement (0.1–0.2 mL) followed by imaging to observe the effect. Even with a cement leak, these small quantities will allow early recognition without much risk of a clinical complication.

A, Lateral radiograph during vertebroplasty of a compression fracture due to breast carcinoma. Note that the thecal sac was first opacified with myelographic contrast. This allows one to watch for deformation of the thecal sac that would indicate tumor displacement during cement introduction.
B, With the thecal sac opacified, axial CT scans provide the most sensitive method to monitor PV for thecal sac compression created by tumor displaced during cement injection.
Vertebral Collapse.—
Extremely compressed vertebra pose a technical challenge for percutaneous cement augmentation. When compressed more than 75%, just getting a needle into the vertebral body can be difficult; however, we have learned that many of these vertebrae can be treated successfully with PV and produce good pain relief (19, 20). In addition, a vertebra that appears almost completely collapsed may have substantial sparing of its height laterally. This occurs because many vertebrae collapse more in the center than they do along the lateral edges (Fig 12). With care, it is quite common to be able to get a 13-gauge needle system into the lateral aspect of these vertebrae and successfully perform PV (Fig 13). Because of the marked central collapse, a bipedicular approach is useful, because it allows better bilateral vertebral filling.

A, Sagittal T1 MR imaging (midline) showing complete central compression of T11.
B, Sagittal T1 MR imaging (lateral vertebral margin) reveals considerable residual marrow space that could be filled with cement during vertebroplasty.

A, Lateral radiograph of an extremely collapsed lower thoracic vertebra. Superior and inferior endplates are identified (black arrows). There is a small air-filled cleft; 13-gauge needles are being introduced via transpedicular route.
B, A lateral image showing one 13-gauge needle in good position before vertebroplasty.
C, Final image after bipedicular vertebroplasty. Good filling of the vertebra was achieved despite the severe collapse. The patient had a good pain response to the procedure.
Patients presenting with pain associated with an extreme vertebral collapse should have an attempt at treatment. The amount of cement for this treatment will be smaller than for less compressed vertebra. It is obvious that, because of the challenging technical nature of these compressions, they should not be one’s first case. They can, however, present a good opportunity for successful pain relief (20).
Refracture after PV.—
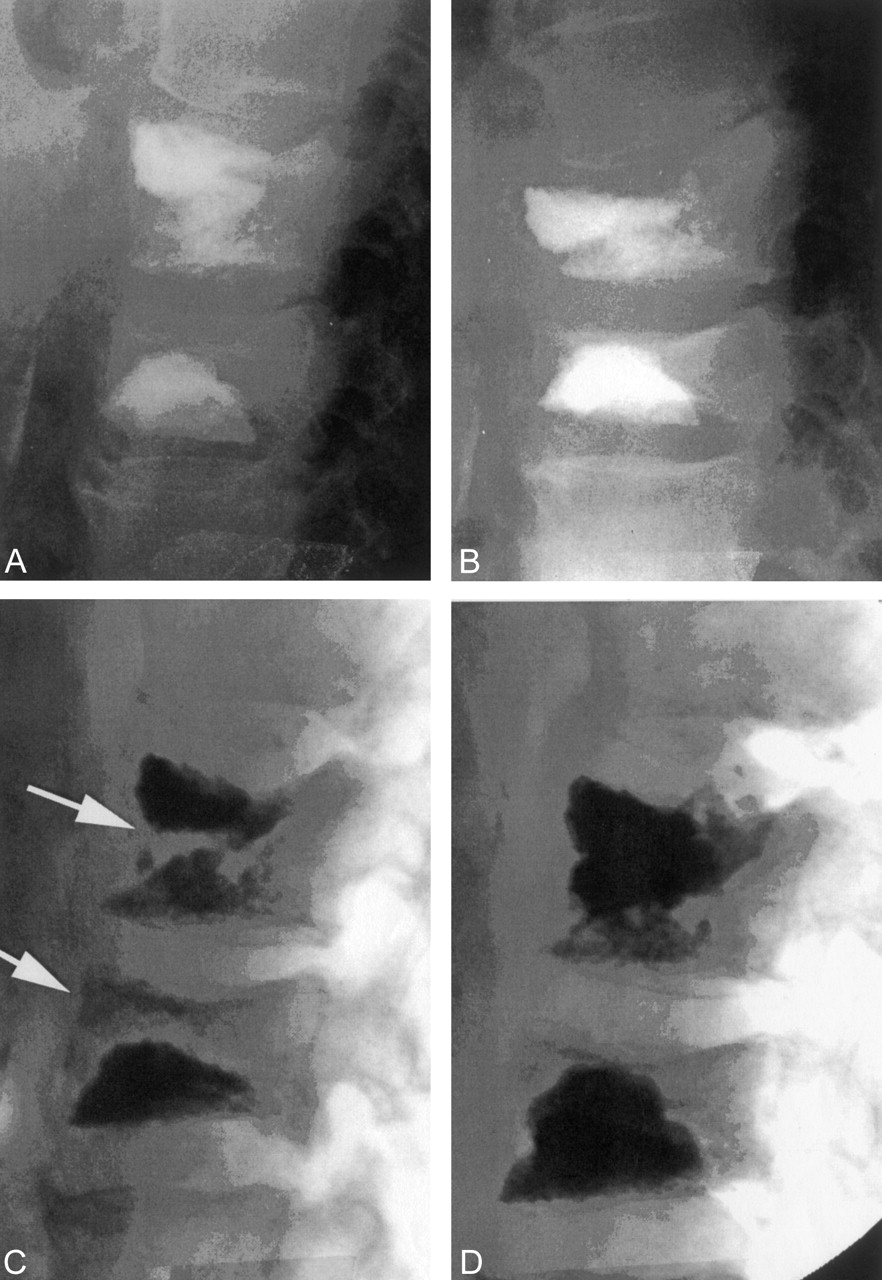
The literature contains little discussion of vertebral refracture following PV. Fracture of other vertebra after PV is not unusual and may require treatment of several levels over the course of months or years. As our treatment numbers have increased, however, we occasionally see vertebra that refractured after treatment with PV. This may occur when too little cement is injected, resulting in less than optimal biomechanical reinforcement the vertebra. Belkoff et al performed an ex vivo study on osteoporotic cadaver vertebrae, randomized to various injection volumes, to determine the quantity of cement needed to restore the original vertebral strength after fracture. This indicated about 2.5–3.0 mL in the upper thoracic spine, 3.0–4.0 mL in the thoraco-lumbar junction, and 6.0–8.0 mL in the lower lumbar spine (21). We know that pain relief has been poorly correlated (if at all) with the quantity of cement injected. This is not the case with biomechanical reinforcement. Some vertebra prove to be so fragile that even with reasonable amounts of cement injected to produce pain relief, there is still a risk of refracture. Figure 14 shows such a case of refracture and a successful repeat PV.

A, Lateral radiograph following a two-level vertebroplasty.
B, Follow-up lateral radiograph after refracture of both previously treated levels. Both levels show height loss compared with image shown in panel A.
C, With the patient placed in mild extension on the angiographic table, the two vertebrae show height restoration and the development of internal clefts (white arrows).
D, The final image following vertebroplasty retreatment. The clefts shown in panel C have been filled with cement. The procedure eliminated the patient’s pain, and this fixation has been durable for more than 2 years.
Repeat imaging and physical examination is needed to establish that there is no new fracture that would better explain the patient’s recurrence of symptoms. When a recurrent fracture is diagnosed, it should be retreated with PV. This can be challenging, because the initial cement can pose a substantial problem for needle placement and injection; however, these vertebrae can be successfully retreated with good pain relief.
The potential for a refracture of a vertebra after PV should be considered when the appropriate imaging and examination findings are obtained. The presentation would include new pain consistent to the site of prior PV, progression of height loss in the vertebra since the PV, and MR imaging findings that show recurrence or increased marrow edema in the treated vertebra. Obviously, MR imaging should demonstrate no other cause of the recurrent pain (eg, new fracture).
Multilevel Therapy.—
The primary indication for PV has been, and remains, pain relief. This has generally limited the indication for PV to treating vertebral fractures that are deemed to be painful by ancillary tests including imaging and physical examination. Compression fractures or metastatic involvement to the vertebra without associated pain are not, as yet, believed to be good indications for PV. At present, multilevel therapy is reimbursed only when there are indications of acute fractures with associated pain. Multilevel therapy, however, is a real issue to be dealt with on a regular basis. Some 20–30% of cases present with two or more acute compressions that need therapy. Usually all acute injuries must be treated to get adequate pain relief. In addition, new fractures are common in patients with osteoporosis and may lead to multiple therapies and ultimately multilevel PV. This can occur with metastatic involvement of the vertebra as well.
The question often arises as to why we do not initially treat multiple levels in an attempt to slow or stop the cascade of fractures that may occur in the severely osteoporotic patient. The reasons are numerous. First, we do not, as yet, have any way of predicting the sites of future fractures. Some clustering is known to occur, but it is just as frequent to see fractures occur away from the original fracture or treatment site. Second, there is some risk to multilevel therapy that presently is not quantified. By virtue of their hydraulic nature, all cement injections push marrow material (or, less likely, cement) out of the vertebra, and this ultimately ends up in the lungs. Small quantities are well tolerated, but in large quantities (or small quantities with preexisting pulmonary compromise) this can create symptomatic events. Anecdotal reports of death secondary to pulmonary compromise following multilevel therapy are known. We do not know an absolute safe number of vertebrae that can be treated without risk of pulmonary side effects. Our general rule has been to treat three or fewer vertebra at a single session. In addition, the central marrow space (of which the spine is a primary component) becomes the location of hematopoiesis is older adults. Filling all or most of the vertebra could lead to anemia or extramedulary hematopoiesis.
Multilevel therapy can be accomplished successfully when approached with caution. Mathis et al reported the first seven-level therapy in 1998 in a 35-year-old lupus patient with multiple compressions secondary to high-dose steroid therapy (22). The treatments were divided, and the patient has had many years without pain or subsequent fracture (with lupus under control and no longer receiving high-dose steroids). I have treated as many as ten levels in a single individual with good results but always dividing therapy into multiple sessions (Fig 15). Prophylactic therapy is still avoided.

Anterioposterior radiograph showing six vertebrae treated with vertebroplasty. Ultimately, 10 levels were treated in this patient.
Conclusion
PV is becoming common in many practices internationally. It has been embraced by physicians and patients alike as a needed and welcome therapy for painful compression fractures of the spine where generally no good therapy existed. It is now becoming the standard of care for these compression fractures in the United States. PV is a simple procedure and is often performed on an outpatient basis. Pain relief has been high and risks low, when performed by experienced physicians who exercise good judgment. With this growing experience, we will be able to tackle and treat successfully more complex cases and expand the utility of this procedure.
References
- Received March 13, 2003.
- Accepted after revision April 9, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pulmonary cement embolisation after percutaneous vertebroplasty
- Republished: Retained needle after cement injection during vertebral augmentation and its management strategy
- Use and evaluation of a semi-permeable mesh implant in vertebral augmentation for the treatment of painful osteoporotic vertebral compression fractures
- Retained needle after cement injection during vertebral augmentation and its management strategy
- Kyphoplasty and Vertebroplasty Produce the Same Degree of Height Restoration