
Abstract
Summary: Sinus pericranii is an unusual venous anomaly characterized by communication of pericranial varicosities with an underlying dural sinus. We report two cases of spontaneous partial thrombosis of sinus pericranii presenting as focally tender, nonreducible mass lesions different in character from the baseline venous abnormality. CT, CT angiography, and CT venography (CTV) were performed in both cases. CTV was essential in depicting thrombi within the varicosities. MR (in one case) demonstrated the anomaly well, but the thrombus was not evident. Conservative therapy was instituted in both cases.
Anomalous communication between the intracranial dural sinuses and dilated epicranial venous structures is known as sinus pericranii. The varicosities are intimately associated with the periostium, are distensible, and vary in size with changes in intracranial pressure (1). Symptoms are infrequent but include headache, vertigo, feelings of fullness, or local pain (2). Thrombi within resected portions of sinus pericranii have been encountered, but to our knowledge, the clinical and imaging features of partial thrombosis have not been addressed. We describe the clinical and imaging findings of two cases of sinus pericranii presenting with marked focal tenderness and partial loss of compressibility secondary to spontaneous partial thrombosis.
Case Reports
Case 1
A 31-year-old woman with sinus pericranii diagnosed at the age of 12 years presented with a sudden increase in prominence and nonreducibility of a varicosity located along her left temporal region, associated with significant overlying scalp tenderness. The painful portion was firm at palpation and measured approximately 1.5 cm in diameter. A smaller partially compressible nodule was present as well.
Surgical ligation of the varicosities via a bicoronal incision had been attempted 8 years before. Percutaneous alcohol ablation of pericranial sinuses had been attempted 3 years prior. These steps had been taken primarily for cosmetic purposes, but also for pain and tenseness of the varicosities upon awakening. Neither treatment was successful. The attempted alcohol ablation resulted in a sixth cranial nerve palsy that has since resolved. The varicosities have continued to enlarge slowly.
Unenhanced head CT demonstrated thinning of the calvaria in the left parietal and temporal regions. The soft tissues along the left parietal and temporal bones had attenuation characteristics similar to blood. Multiphasic CT angiography (CTA) was obtained. The initial acquisition was performed with a 15-second injector delay, a 3-mL/s injection rate, and 1.25-mm section thickness. The patient was then repositioned with her head extended and dependent (below the level of her heart) while direct coronal imaging was performed. A final delayed axial CT venogram (CTV) was necessary to image the vertex, because it was not covered in the coronal CT. The data were then processed with multiplanar volume reformatting and volume rendering on a GE Advantage workstation (GE Medical Systems, Milwaukee, WI). CTA showed focal enhancement of the portion of the sinus pericranii nearest the connection with the sagittal sinus (Fig 1A). CTA also allowed the depiction of the actual transosseous and diploic abnormalities (Fig 1B). The remainder of the pericranial sinuses remained unopacified because of the slow flow status of some of the connections (Fig 1C). No arterial abnormalities were appreciated.

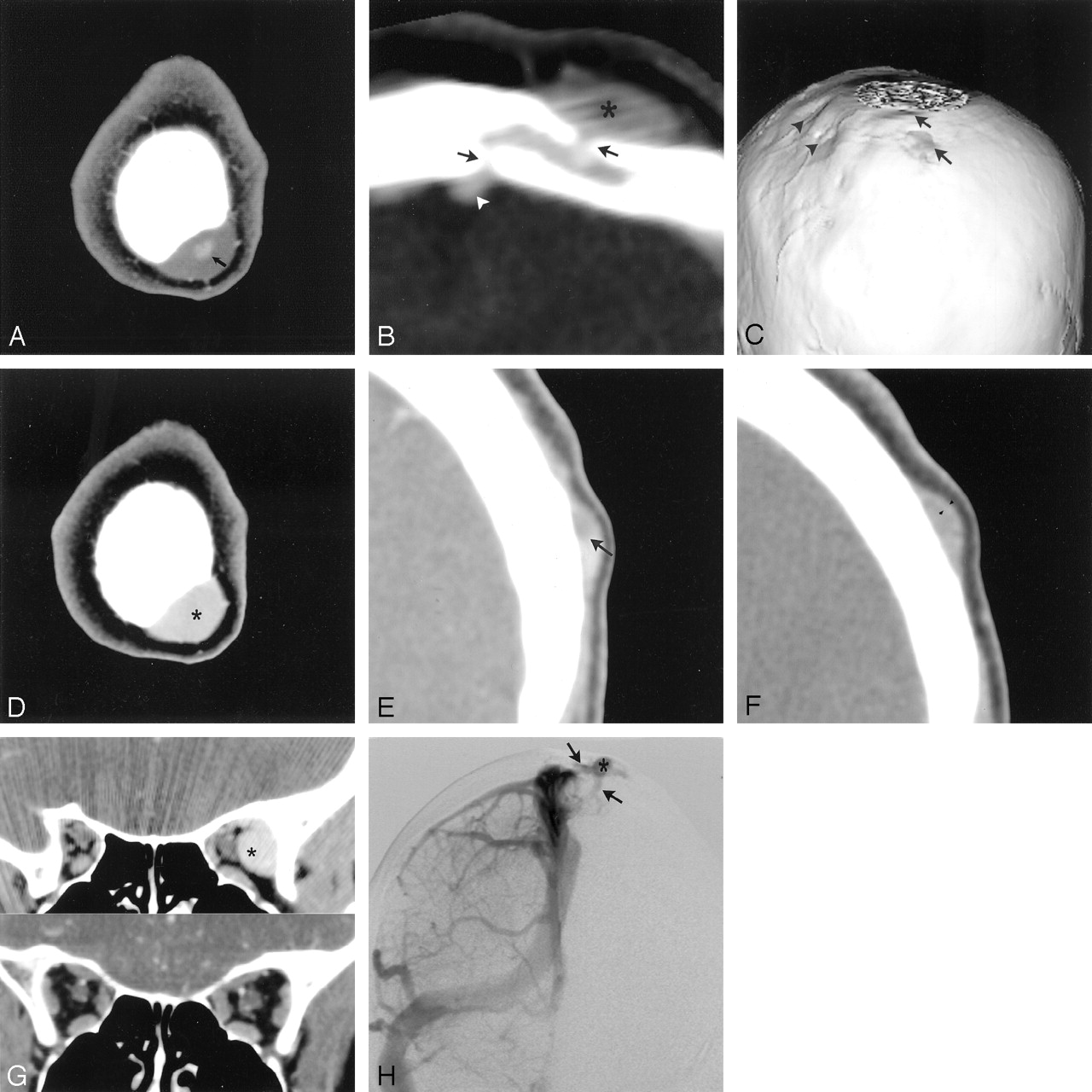
31-year-old woman with sinus pericranii and sudden onset of pain and swelling over the left scalp.
A, Source image from CTA (first pass) demonstrates only partial filling of a varicosity with contrast (arrow).
B, Reformatted oblique coronal CT through the earliest filling varicosity (asterisk) demonstrating defects within both the inner and outer tables (arrows) of the calvaria and filling of the diploe with venous blood. The connecting intracranial vein is denoted by the white arrowhead.
C, Volume-rendered CTA of the calvaria viewed from behind. Multiple calvarial depressions are seen along the left parietal and temporal bones (arrowheads). These depressions underlie slow-filling varicosities. The varicosities with the more direct connections to the dural sinuses already show enhancement (arrows).
D, Source image from the axial CTV through the same level as in A. The varicosity (asterisk) now demonstrates homogeneous enhancement.
E, Delayed coronal CT image demonstrates a sharply demarcated filling defect within a varicosity (arrow). The higher signal intensity represents flowing venous blood.
F, Delayed coronal CT through the region of greatest tenderness demonstrates only peripheral enhancement (arrowheads). This was only minimally compressible.
G, Coronal CT image (above) acquired with the head extended and dependent demonstrates an orbital varix (asterisk). A coronally reformatted CT image (below) shows the same region, but without the venous anomaly.
H, Angiographic anteroposterior view (venous phase) of a selective right internal carotid artery injection demonstrates the venous connections (arrow) to a pericranial varicosity (asterisk). Flow is both into and out of this pericranial varicosity.
Delayed imaging, or CTV, in the axial and coronal planes demonstrated homogeneous enhancement throughout the varicosity (Fig 1D) with the exception of two well-demarcated, nonenhanced areas located along the left frontotemporal region (Fig 1E and F). These nonenhancing areas correlated with the two acutely tender lesions detected by palpation and were felt to represent acute thrombosis.
In addition, CT with dependent positioning of the head revealed a left orbital varix (Fig 1G) that was not suspected on any of the prior studies.
Digital subtraction cerebral angiography (DSA) confirmed the transosseous connection with flow of blood from the sagittal sinus to the overlying pericranial varicosity and from the varicosity to an adjacent intracranial vein (Fig 1H).
The patient was reassured that no tumor or other significant abnormalities were present. She was treated conservatively with nonsteroidal medications and warm compresses with subsequent improvement of her symptoms within a month.
Case 2
A 53-year-old woman with a left frontal vascular anomaly diagnosed as a cavernous hemangioma during her childhood presented with complaints of increasing headaches. MR imaging performed at an outside facility demonstrated enhancement of the scalp, calvaria, and dura without invasion of the underlying brain. A left frontal lobe cavernous angioma and an adjacent developmental venous anomaly (venous angioma) were incidentally demonstrated. The decision was made to obtain a follow-up MR image in 1 year unless significant changes occurred. One month later, she returned to the clinic with exquisite focal pain and nonreducible components of her hemangioma. Because of this dramatic change, surgical resection was planned.
MR imaging was performed the day before planned resection, with an intraoperative navigation protocol (sagittal spin-echo T1-weighted, axial and coronal gradient T1-weighted imaging; all sequences performed after intravenous contrast medium administration) to assist in localization. This MR demonstrated an extracalvarial mass with extension through the right frontal bone, consistent with sinus pericranii. Minimal heterogeneity was evident on the sagittal spin-echo T1-weighted and gradient T1-weighted postcontrast sequences within the pericranial varicosity (Fig 2A). No distinct thrombus was demonstrated.

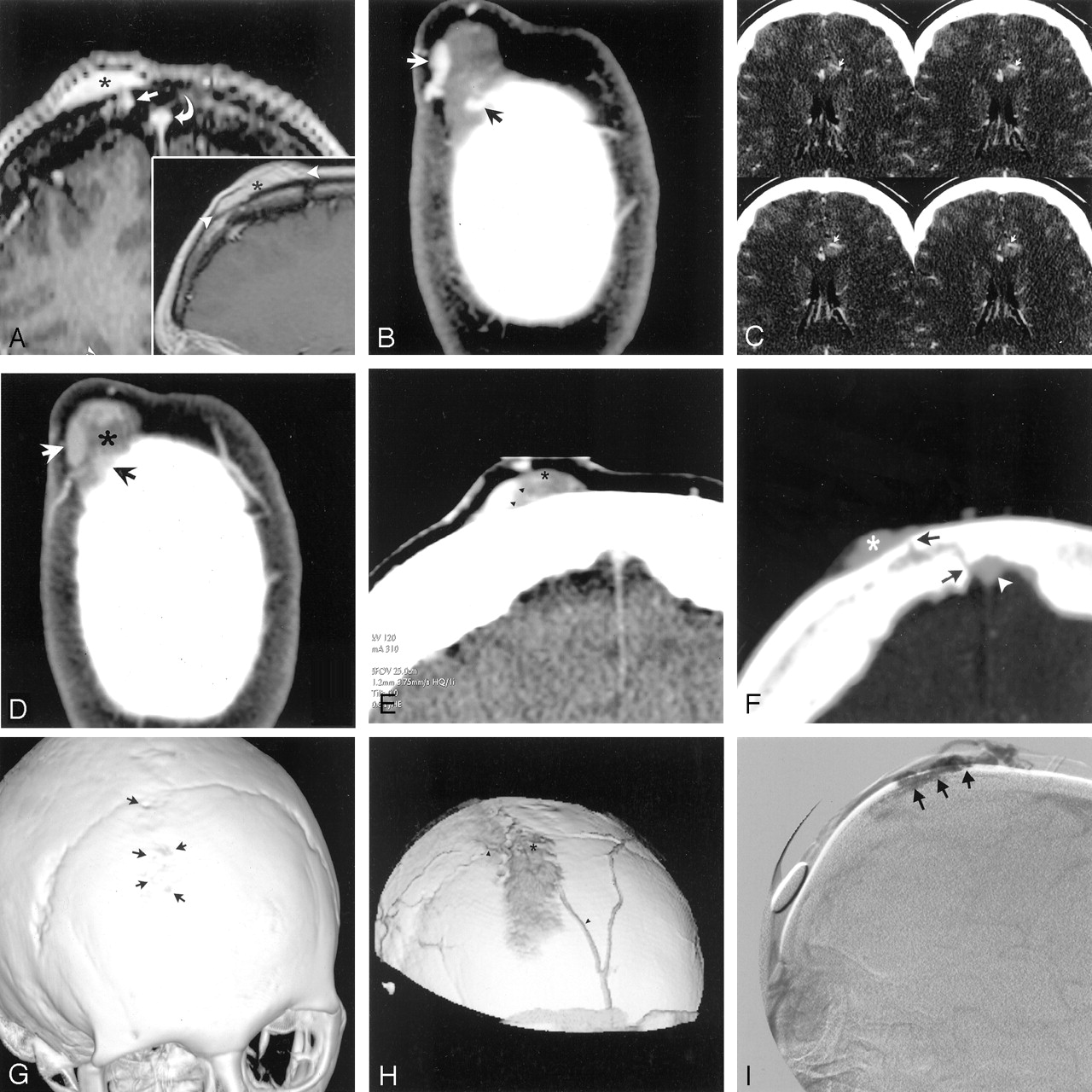
53-year-old woman with sinus pericranii and extreme pain involving the right forehead and scalp.
A, Coronal postcontrast gradient T1-weighted (full image) and sagittal postcontrast spin-echo T1-weighted (inset) MR images demonstrate the homogeneous appearance of the pericranial varicosity (asterisks). The coronal image clearly demonstrates one of the trans-osseous connections (arrow) as well as the adjacent superior sagittal sinus (curved arrow). The arrowheads in the inset demarcate the extent of the varicosity.
B, Source image from a CTA through the right frontal mass shows enhancement of preferential channels of flow (arrows) with most the varicosity remaining unenhanced.
C, Axial source images from the CTA demonstrating a small developmental venous anomaly just adjacent to a cavernous angioma. The arrows point to the single draining venous trunk while the cavernous angioma is of increased attenuation just posterior to the vein.
D, Source image from the axial CTV through the same region as Fig 2B. The varicosity is largely thrombosed (asterisk) in this portion. The patent channels of flow have become less distinct (arrows), and the anterior aspect now demonstrates enhancement.
E, Coronal postcontrast CT clearly depicts (arrowheads) the flowing venous blood from the adjacent thrombus (asterisk).
F, Reformatted oblique axial image from the CTV data through the inferior aspect of the pericranial varicosity. One of the transosseous pathways from the superior sagittal sinus (arrowhead) to the pericranial varicosity (asterisk) is clearly demonstrated. The defects within the inner and outer table of the frontal bones are denoted by arrows.
G, Volume-rendered image of the skull viewed obliquely from the front. Multiple small defects (arrows) are seen within the outer table of the right frontal bone. Compare this image to Fig H.
H, Volume-rendered image from CTV data shows the pericranial varicosity and adjacent scalp veins (arrowheads). The region of the clot is demarcated by an asterisk. The view is similar to that depicted in Fig 2G with the calvaria tilted more to the left.
I, Late venous phase image (lateral projection) from a selective injection of the left internal carotid artery depicting the pericranial varicosity (arrows).
During the preoperative physical assessment performed the night before surgery, the region of acute tenderness and firmness was less remarkable than at her prior clinic visit, both objectively and subjectively. CT, CTA, CTV, and conventional angiography were then performed in the same manner as case 1. Surgery was cancelled.
Unenhanced CT of the head demonstrated hyperostosis frontalis interna and focal thinning of the calvaria along the right frontal bone. Superficial to the calvarial thinning was a prominent soft tissue mass. Also noted, was a rounded region of increased attenuation within the left frontal lobe corresponding to the known cavernous angioma.
CTA demonstrated no arterial abnormalities. The pericranial varicosities demonstrated focal enhancement with marked heterogeneity in attenuation (Fig 2B). The left frontal lobe cavernous angioma and adjacent developmental venous anomaly (venous angioma) were demonstrated (Fig 2C).
The CTV demonstrated a slightly more homogeneous appearance of the varicosity (Fig 2D) with the exception of an irregular but sharply demarcated filling defect (Fig 2E) thought to represent a subacute thrombus. Reformatted CTV data were able to demonstrate one of the transosseous routes of flow (Fig 2F). Volume-rendered imaging displayed the calvarial anomalies (Fig 2G) as well as the varicosity and adjacent draining scalp veins (Fig 2H).
DSA confirmed the presence of the pericranial varicosity (Fig 2I) filled via transosseous veins.
Surgical resection was offered to the patient, but she declined. The abnormality was above the hairline and not otherwise bothersome to her. As in case 1, nonsteroidal medications and warm compresses were prescribed.
Discussion
Aptly donned sinus pericranii in 1850 by Stromeyer (3), the venous anomaly is a collection of nonmuscular venous blood vessels adhering tightly to the outer surface of the skull and directly communicating with an intracranial venous sinus through diploic veins. The venous collections receive blood from and drain into the intracranial venous sinuses (1).
Most cases appear to be congenital in nature and are frequently associated with other venous anomalies and syndromes (4), as were the cases presented in this report. The primary concern is often cosmetic, but common symptoms include headaches, sensations of pressure or fullness, or local pain (5). In rare cases, severe symptoms such as bradycardia, bradypnea (6), or hearing loss (7) have been described. The varicosities tend to increase in size slowly, although there has been a report of spontaneous regression (8). Treatment, when necessary, is surgical in most cases, although, as in case 1, endovascular therapy has been performed (9).
Thrombi within the resected portions of sinus pericranii have been noted (10, 11) at pathologic examination, but the imaging characteristics and distinct clinical presentation of acute thrombosis have not been previously described. The occurrence of partial thrombosis is not unexpected, because of the slow flow of blood within these lesions as well as the common occurrence of thrombi within venous malformations elsewhere in the body (12).
A sudden alteration in character of the lesion from soft and painless to firm and painful is of concern to both the patient and physician. Previously undiagnosed or improperly diagnosed vascular lesions with rapidly changing character and the onset of atypical pain may suggest an underlying neoplasm or infection. The pathologic appearance of luminal thrombi within venous malformations can be misleading. Reactive intravascular papillary endothelial hyperplasia can occur in this setting (11–13) and has previously been referred to as Masson’s vegetant intravascular hemangioendothelioma or Masson’s pseudoangiosarcoma. It is important that this benign process not be confused with similar-appearing malignant processes such as endovascular papillary angioendothelioma, Kaposi sarcoma, or angiosarcoma.
CTA with early and delayed imaging has a very characteristic appearance and can demonstrate filling defects within the varicosities that correspond to the sites of focal tenderness on physical examination. CTA in both of the presented cases demonstrated paracranial collections with contrast enhancement in the immediate vicinity of the transosseous connections and higher flow regions on the first pass. CTV demonstrated homogeneous enhancement throughout the varicosities with the exception of the tender portions where filling defects were demonstrated in both cases. The delayed imaging is critical for the correct delineation of the normal slow flowing blood from the adjacent clot. CTV performed with the head dependent did not contribute additional information except for depiction of an orbital varix in case 1.
An MR image in the case presented by Bigot et al (13) demonstrated a sharply demarcated varicosity at postcontrast T1-weighted imaging. Upon pathologic examination, thrombus was noted within the resected tissue. The patient in that case was an infant, and acute signs or symptoms were not remarked upon by the authors.
MR in case 2 of this report was less helpful. Contrast-enhanced MR demonstrated a homogeneously enhancing mass lesion extending through the calvaria. The absence of differential signal intensities within the varicosities is concerning but understandable. The T1 hyperintense nature of the subacute clot on T1-weighted images did not allow discrimination of the thrombus from that of the enhancing, nonclotted venous blood. Precontrast imaging was not performed in this case and it is unknown what contribution this may have had to delineation of clot versus free-flowing blood.
Angiography in both cases was diagnostic, demonstrating connections between the epicranial varicosities with an underlying dural sinus. Direct venography via direct puncture of the scalp was not necessary for diagnosis in these cases but can be useful if conventional angiography is equivocal or nondiagnostic (14).
The filling defects demonstrated by CTV were not biopsied or excised. The possibility that these may be fibrous septations or other soft tissue exists; however, the T1 hyperintense characteristics on MR (case 2), in addition to the transient relationship with focal pain (cases 1 and 2) make this unlikely. Case 1 is complicated by having undergone prior surgery and attempted endovascular ablation. Both interventions had occurred years earlier and would unlikely account for the sudden appearance of atypical pain.
Conclusion
Rare, seldom symptomatic, and often misdiagnosed, sinus pericranii is a challenging diagnosis. Partial thrombosis of the pericranial venous component adds complexity to these lesions and results in focal pain and noncompressibility with palpation. CTV proved to be essential in depicting intraluminal thrombi from adjacent slow-flowing blood.
References
- Received April 8, 2003.
- Accepted after revision April 28, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}