
Abstract
BACKGROUND: Diagnosing TIA can be difficult, since evidence of brain ischemia is habitually lacking on CT and conventional MR imaging. It has been suggested that patients with acute brain infarction on neuroimaging should be considered stroke cases instead of TIA, regardless of duration of symptoms, implying that optimal diagnostic methods need to be utilized. We therefore postulated that perfusion-weighted MR imaging (PW imaging) would be useful in the diagnosis of TIA.
METHODS: Retrospective analysis of 22 patients with reversible neurologic symptoms lasting less than 24 hours, assessed with DW and PW imaging.
RESULTS: MR imaging was abnormal in 15 patients (68%): 12 had abnormal DW imaging, four had both DW and PW imaging defects (all with a mismatch) and three had an isolated PW imaging abnormality. There were no differences in symptom duration, stroke etiology or cardiovascular risk factors between patients with abnormal MR imaging and those with unremarkable scan. Patients with mismatch were more likely to need conventional angiography or other cerebrovascular procedures.
CONCLUSION: The combined use of DW imaging and PW imaging provided evidence of brain ischemia in most patients with clinical diagnosis of TIA. Prospective studies using follow-up MR imaging are required to determine the outcome of affected tissue, as well as the clinical implications of DW–PW imaging abnormalities.
It is difficult to establish that transient neurologic symptoms correspond to brain ischemia, because most patients appear normal neurologically at the time of initial assessment and often relate vague complaints. In addition, head CT and conventional brain MR imaging may not provide objective evidence of brain ischemia to support the diagnosis. Although a detailed diagnostic work-up may disclose the presence of diseases associated with ischemic stroke and transient ischemic attack (TIA), such findings do not necessarily prove that the cause of symptoms was indeed brain ischemia. On the other hand, the traditional 24-hour defining limit of TIA has recently been challenged by arguing that a diagnosis of ischemic stroke should be assigned to all patients with evidence of acute brain infarction on neuroimaging, regardless of the duration of symptoms, implying that optimal diagnostic tools need to be utilized systematically in TIA to rule out acute brain infarction (1).
Although diffusion-weighted (DW) imaging can detect signs of acute brain ischemia in 29–67% of patients with TIA (2–8), limited information regarding the added value of perfusion-weighted (PW) imaging is currently available (9–15). PW imaging does not usually provide quantitative measures of cerebral blood flow, but it does allow rapid evaluation of relative hemodynamics in the same scanning session as DW and conventional MR imaging (13, 16, 17). Most PW imaging defects accompany (13, 16, 17) or even precede (14) the development of DW imaging abnormalities in a substantial proportion of patients with brain ischemia. Therefore, the purpose of the current study was to test the hypothesis that PW imaging would substantiate the diagnosis of brain ischemia in an additional proportion of patients with transient neurologic symptoms.
Methods
Patients
Patients admitted to our hospital from January 1996 to August 2003 with reversible neurologic symptoms lasting <24 hours (clinically diagnosed as TIA by one of two neurologists [L.R., R.J.W.]), were retrospectively identified from a computer registry. The query retrieved 179 cases, from which 22 (12%) had brain MR imaging with DW and PW imaging as part of their diagnostic work-up. The MR imaging protocol and acquisition of clinical data were approved by the local IRB.
None of the patients had treatment with thrombolysis (IV or IA), percutaneous angioplasty, mechanical disruption of the occluding thrombus, or induced hypertension before the MR imaging. Clinical and demographic variables, as well as information regarding symptom onset, were gathered from the chart of every patient. Exact time of MR imaging examination was available for all cases, but documentation of the exact onset of symptoms (i.e., date, hour and minute) was available for 17 patients. The remaining five patients did not have an exact time of symptom onset specified in the chart, although the notes of the attending physician remarked that symptoms lasted less than 24 hours in all of these cases.
MR Imaging Examination
Images were acquired on a 1.5 T GE Signa scanner with echo-planar (EPI) capability (GE Milwaukee, WI). The MR imaging protocol has been detailed elsewhere (16, 17). Briefly, it consists of conventional T1, axial fast-spin-echo T2-weighted and axial fluid-attenuated inversion-recovery (FLAIR), time-of-flight MRA (head and neck), DW and PW imaging. Apparent diffusion coefficient (ADC) maps were generated and reductions in ADC were used to confirm acute brain ischemia. PW imaging was obtained by using dynamic first-pass bolus tracking of gadolinium with a multi-section axial gradient-echo scan.
Cerebral blood flow (CBF), mean transit time (MTT) and time-to-peak (TTP) maps were generated and qualitatively assessed by an investigator. Volumes of DW imaging and TTP abnormalities were manually delineated by region-of-interest, by using Scion Imaging (Scion Corporation, 1998). The areas of abnormality in cm2 on each section were summed, and the sum multiplied by the interslice spacing, to determine the volume in cm3. Hypoperfusion was defined as a region with >2.5 seconds delay on TTP maps, compared with a homologous area of the contralateral hemisphere. This threshold is based on evidence suggesting that neurologic function correlates with the volume of brain regions exhibiting a TTP delay of >2.5 seconds (16, 17).
We defined DW–PW imaging mismatch as a TTP volume defect greater than its related DW imaging lesion. We chose this threshold because it reflects the reality of our practice: MR imaging is assessed by a team of physicians without immediate access to volumetry. Therefore, the involved team made clinical decisions based on a qualitative assessment of TTP sequences. We measured the magnitude of mismatch as (TTP volume - DW imaging volume / TTP volume) × 100 = % mismatch. According to this definition, the mismatch group does include patients with isolated TTP abnormalities.
Statistical Analysis
Patients were divided into three groups for comparison: Unremarkable MR imaging, abnormal MR imaging (abnormal DW or PW imaging) and DW imaging–PW imaging mismatch. Differences between clinical characteristics of patients with and without MR imaging abnormalities were explored with Chi-squared and Student’s t test. Differences between more than two variables were analyzed with one-way ANOVA; they were significant at P < .05.
Results
Average patient age was 62 ± 14 years, and half of the patients were female. A total of 15 patients (68%) had DW or PW imaging abnormalities. Of these, eight had isolated DW imaging lesions, three had isolated PW imaging defects, and four had both DW and PW imaging changes. Thus, we considered that the last seven patients had a mismatch. The magnitude of the mismatch was typically large (Range: 44–100%, average: 84%). The region of restricted diffusion overlapped with the larger TTP defect partially on two of the four patients with both DW and PW imaging changes (Fig 1). The other two patients with both DW and PW imaging changes had an area of diffusion restriction totally encompassed by the TTP defect. The head CT revealed signs of acute infarct on only one of these patients. Average lesion volume was 17 ± 27 cm3 for the DW imaging lesions and 112 ± 173 cm3 for the PW imaging defects. All the DW and PW imaging abnormalities involved the anterior circulation of the brain.

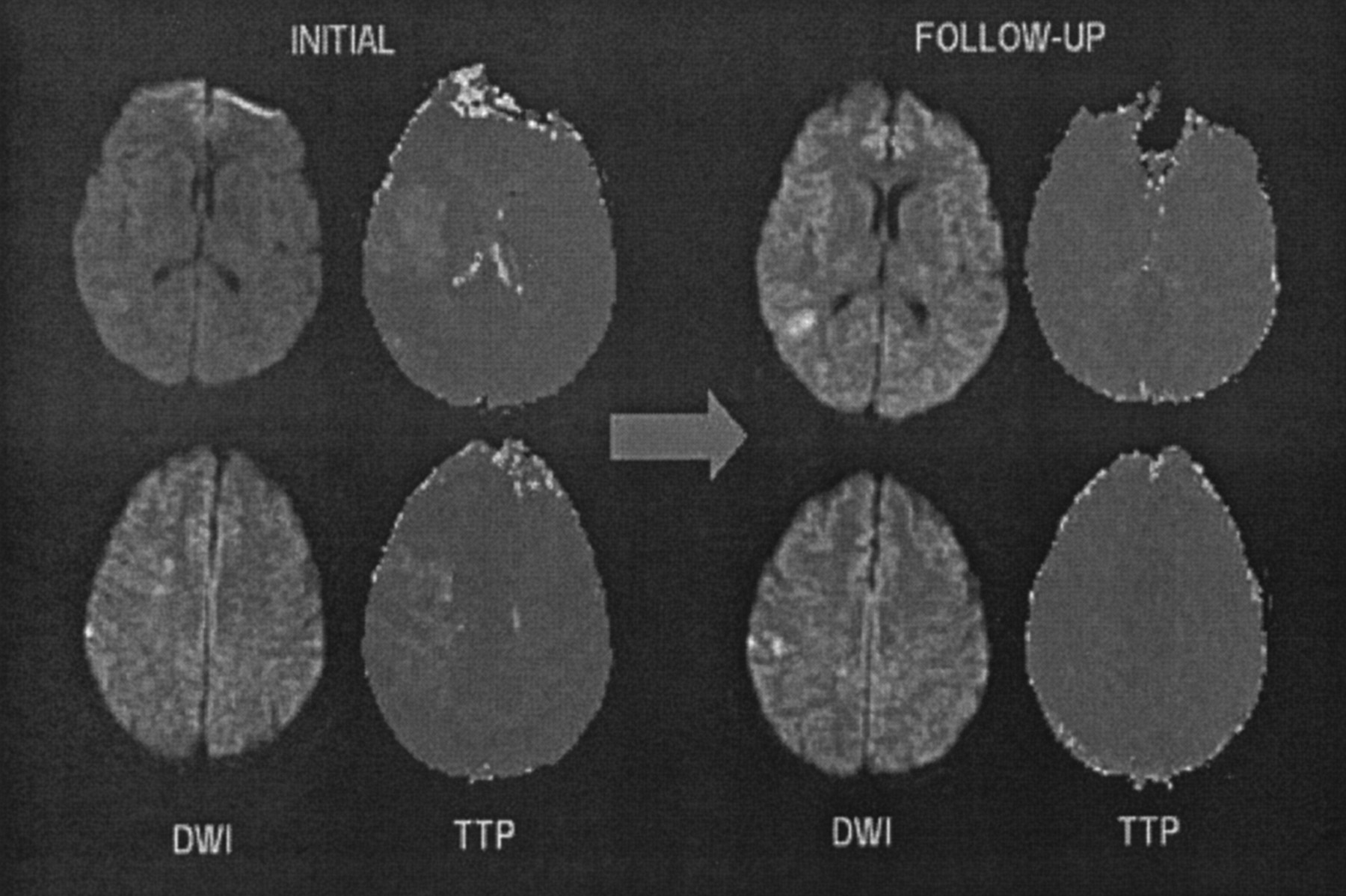
Brain MR imaging of case 1. Left, Initial images show faint DW imaging hyperintensities in the right temporal lobe (top) and frontoparietal junction (bottom). Right, Follow-up images obtained 6 days later show slight expansion of the DW imaging abnormalities but complete resolution of the PW imaging defects.
There was no difference in the prevalence of cardiovascular risk factors between patients with abnormal DW–PW imaging as compared with those with unremarkable scan (table 1). However, patients with mismatch were more likely to have coronary artery disease (P = .032) and hyperlipidemia (P = .045) than the rest of the patients. All lesions noted on MR imaging were consistent with the focal neurologic symptoms reported by the patients. Hemiparesis was significantly associated with abnormal findings on MR imaging (i.e., abnormal DW or PW imaging, P = .047). However, other neurologic symptoms were not predictive of MR imaging abnormalities. The duration and number of episodes of transient neurologic dysfunction did not differ between patients with abnormal DW–PW imaging when compared with those patients with unremarkable scan. The presumptive cause of TIA was large artery atherosclerosis (LAA) in eight patients, cardioembolism in three patients, other cause (aortic atherosclerosis) in three patients and unknown cause in eight cases. There was a significant association between LAA and mismatch (6/7 patients, P = .02). Table 2 provides a summary of the clinical characteristics of the mismatch cases.
Clinical and demographic variables
Clinical characteristics of mismatch cases
Time to MR imaging did not differ between patients with abnormal MR imaging compared with those with unremarkable scan. Mean length of stay in the hospital was 5 ± 3 days for patients with abnormal DW imaging or PW imaging, 6 ± 3 days for patients with mismatch and 3 ± 3 days for those with normal MR imaging, which did not reach statistical difference. None of the patients developed clinical stroke during the hospitalization. None of the mismatch cases reported a stroke after several follow-up visits at the out-patient clinic. Only two patients (both with mismatch) had follow-up MR imaging at the hospital, one showing resolution and the other persistence of the PW imaging defect (cases 1 and 3, respectively; see below). Conventional angiography was performed in 5/7 patients with mismatch, whereas none of the other patients required such procedure. Patients with mismatch on MR imaging were more likely to have a surgical or endovascular procedure than patients without mismatch (5/7 versus 1/15; P = .001). Two of the patients with mismatch were treated with percutaneous balloon angioplasty (without stent), two had carotid endarterectomy and one had intracranial–extracranial bypass. The following is a report of three illustrative cases:
Case 1
A 56-year-old gentleman with history of coronary artery disease, hypertension, diabetes and hyperlipidemia, was noted to develop dysarthria and left hemiparesis during percutaneous coronary angioplasty. He received heparin, midazolam and fentanyl before the procedure. His blood pressure was 140/70 and the NIH stroke scale score was 11. The neurologic deficits, however, completely resolved in 20 minutes. The head CT was unremarkable. Brain MR imaging is shown on Figure 1. Initial MR imaging obtained 5 hours after the neurologic deficits resolved demonstrated faint DW imaging hyperintensities involving the right temporal lobe and frontoparietal junction. The PW imaging exhibited a larger area of relative hypoperfusion involving the right middle cerebral artery territory (perfusion–diffusion mismatch). Follow-up MR imaging, obtained 6 days later, demonstrated slight expansion of the DW imaging abnormalities but complete resolution of the PW imaging defects. Intracranial MRA, Carotid duplex and transthoracic echocardiograms were unremarkable. The patient was admitted to the stroke unit, where he had a recurrence of symptoms lasting less than 20 minutes, coinciding with an episode of hypotension. He received intravenous normal saline and all anti-hypertensives were withheld to keep mean arterial blood pressure >100 mm Hg. Therapy with intravenous heparin was also initiated. He remained asymptomatic thereafter and was discharged to home on oral aspirin and warfarin. We believe that this case is consistent with an embolic brain infarction manifested by TIA.
Case 2
A 61-year-old gentleman was noted to develop cephalalgia, speech difficulties and “confusion” on postoperative day 2 after coronary artery bypass surgery (CABG). He underwent surgery because of persistent angina after myocardial infarction, despite intensive medical therapy. Past medical history was notable for two prior ischemic strokes, known left internal carotid artery (ICA) occlusion despite of bilateral carotid endarterectomy, prior CABG, peripheral vascular disease and hypertension. The neurologic examination was remarkable for fluent aphasia with difficulty understanding commands. However, the neurologic deficits completely resolved in 20 minutes. The brain MR imaging, obtained 7 hours after symptoms resolved, is shown on Figure 2. The FLAIR sequence (left, up) reveals two areas of leukomalacia in the right antero-lateral temporal lobe and temporo-occipital junction. The MRA (left, down) demonstrates absent left internal carotid artery with reduced caliber of the middle cerebral artery, which fills out through the anterior communicating artery. Large posterior collaterals can also be appreciated. The DW imaging (middle) did not demonstrate areas of hyperintensity. However, the PW imaging (right) revealed a large region of perfusion delay affecting most of the left hemisphere. No follow-up MR imaging was obtained. The following day, the patient complained of right upper extremity paresthesia, although his neurologic examination was unremarkable. He was treated with oral warfarin, while all anti-hypertensive medications were withheld. The patient was discharged to home on postoperative day number 8. This case is consistent wit a hemodynamic TIA in the setting of ICA occlusion.

Brain MR imaging of case 2. Top, upper cut images; bottom, lower cut images.
Case 3
A 63-year-old gentleman experienced a fall because of sudden weakness on the right leg. He reported innumerable previous episodes of right leg weakness, always lasting 15–20 seconds, for almost one year. However, he had never fallen as consequence of these. Sometimes the episodes would occur several times per day and feature ipsilateral hand clumsiness. Past medical history was significant for hypertension, hyperlipidemia and diabetes. His physician suspected TIA and treated him with clopidogrel and warfarin, which did not ameliorate the symptoms. The neurologic examination was normal. Brain MR imaging and MRA (shown on Fig 3), obtained eight days after patient’s last TIA, demonstrated hyperintensities on FLAIR involving the anterior cerebral artery (ACA) territory bilaterally. Although DW imaging shows hyperintensities in the same locations, the apparent diffusion coefficient was locally increased, suggesting that the lesions were old (i.e., T-2 “shine-through”). PW imaging demonstrates a defect involving the left ACA territory. The MRA shows severe stenosis of the left intracranial ICA and tandem stenosis involving both A1 and A2 segments of the ACAs. MR imaging did not change after ICA angioplasty. A conventional angiography showed high-grade stenosis of the left intracranial ICA, just proximal to the anterior choroidal artery. The left middle cerebral artery filled out from the right side through the anterior communicating artery and A1 segment of the anterior cerebral artery. The patient underwent balloon angioplasty of the left ICA. He remained asymptomatic during his hospital stay and was discharged to home on warfarin, aspirin and atorvastatin. This case is an example of hemodynamic TIA, in association with severe intracranial stenosis.

Brain MR imaging of case 3. The MRA shows severe stenosis of the left intracranial ICA (arrow) and tandem stenosis involving both A1 and A2 segments of the ACAs (arrowheads).
Discussion
This study suggests that the addition of DW and PW imaging to the conventional MR imaging protocol can enhance detection of brain ischemia or hypoperfusion in patients presenting with transient focal neurologic symptoms. Specifically, TTP maps identified ischemic tissue not detected on conventional or DW imaging sequences in 32% of our patients with TIA. This is relevant because of two main reasons: firstly, it has been suggested that patients with transient focal neurologic symptoms should be diagnosed with ischemic stroke instead of TIA whenever there is evidence of acute brain infarction on neuroimaging, implying that optimal diagnostic methods need to be utilized systematically in the routine diagnostic work-up of TIA (1). Such point of view is endorsed by evidence suggesting that patients with TIA with acute brain infarction may have poorer outcomes than those patients with unremarkable neuroimaging (18). Secondly, transient neurologic symptoms are often vague, causing untoward confusion among practitioners regarding the true pathophysiologic nature of the clinical picture. In this study, the diagnostic yield of MR imaging with DW imaging and PW imaging was superior to noncontrast CT, detecting evidence of brain ischemia or hypoperfusion in almost 3/4 of patients. Therefore, an abnormal MR imaging with DW imaging and PW imaging can help the clinician to substantiate the diagnosis of TIA when the symptoms are nonspecific. Despite the advantages of MR imaging over CT, the former is used in less than 5% of TIA cases seen in American emergency rooms (19).
The use of PW imaging permitted the detection of regions of abnormal signal intensity in seven of our patients (four with and three without concomitant DW imaging changes), indicating the presence of tissue at risk for infarction and, theoretically, with a potential for clinical deterioration. Furthermore, MR with PW imaging identified a subset of patients who required conventional angiography, having an impact on patient management. Thus, MR imaging could assist the clinician in the selection of patients that should be admitted to the hospital for close observation, instead of being discharged after a rapid diagnostic evaluation. This argument is endorsed by our observation that most patients with DW–PW imaging mismatch frequently necessitated surgical or endovascular procedures, whereas all controls were treated medically. Although none of the patients in our cohort sustained an ischemic stroke (regardless of the presence of mismatch), we speculate that the interventions performed on them may have prevented a poor outcome.
TIAs are not benign. Patients presenting with reversible neurologic defects have a 30% risk of ischemic stroke within 90 days, particularly during the first 48 hours (20). In addition, there is a 15% annual risk of death and a similarly increased risk of myocardial infarction, angina, arrhythmia and congestive heart failure (20, 21). There is abundant evidence suggesting that TIA itself is associated with structural brain damage (2–9). Furthermore, patients with TIA develop more “silent” infarcts and cortical atrophy on follow-up brain MR imaging than age-matched controls (22, 23).
Only a few studies have used MR imaging-based cerebral blood flow or perfusion estimates in patients with TIA. The largest study did not detect any blood flow abnormalities, which contradicts our findings (9). However, the employed technique was a 2D phase-contrast flow measurement, which may not optimally reflect regional brain perfusion. Another study demonstrated PW imaging abnormalities (using relative cerebral blood volume, CBF and MTT) in patients with ICA stenosis or occlusion, including four cases presenting with TIA (10). This is in agreement with our findings that PW imaging abnormalities in TIA patients are associated with the presence of large-artery atherosclerosis. Two additional reports have suggested a relationship between delayed TTP and TIA in patients with nonatherosclerotic large-vessel disease, such as moya-moya (11, 12).
Isolated PW imaging changes in TIA have been observed by other investigators (13–15). At least two patients with TIA imaged with DW–PW imaging 2 hours after symptom onset, have exhibited an isolated region of signal intensity abnormality on PW imaging with unremarkable DW imaging (13, 14). Follow-up MR imaging showed an acute infarct on DW imaging in one case (14), whereas the other patient had no subsequent DW or PW imaging abnormalities (13). Another case report described a patient with DW and PW imaging abnormalities that resolved on follow-up MR imaging (15). Our observations add to the literature new cases of TIA imaged with PW imaging, particularly using TTP maps, demonstrating DW–PW imaging mismatch in almost 1/3 of patients.
Our study is limited by its retrospective nature and lack of systematic follow-up neuroimaging. The last constraint prevents a direct assessment of the outcome of tissue with abnormal signal intensity on DW imaging and PW imaging. Although most DW imaging abnormalities progress irreversibly to infarcts featuring T-2 signal intensity hyperintensity, instances of complete resolution of diffusion restriction have been well documented (2, 5, 8). On the other hand, PW imaging abnormalities may not progress to infarction and resolve spontaneously (13). Nevertheless, clinical indicators can be used as surrogate markers of tissue injury and recovery. For instance, all patients from our cohort returned to their neurologic baseline in less than 24 hours and left the hospital in excellent condition, suggesting that structural brain damage was modest, if any.
In addition, the optimal PW imaging technique is subject of controversy. We utilized TTP, which is widely used and appears to correlate well with other techniques, such as MTT (24). TTP has good contrast-to-noise ratio, which is an estimate of the conspicuity of abnormal signal intensity, facilitating the identification of lesion boundary (24). Another constraint of this study is a selection bias, since not all patients with TIA managed at our institution routinely undergo diffusion and perfusion MR imaging studies. A prospective study by using DW–PW imaging in all patients presenting with TIA would be needed to better assess the effectiveness of this diagnostic test.
Although our results endorse previous studies showing that transient hemiparesis is associated with MR imaging abnormalities (4), we could not identify other clinical characteristics which could predict DW–PW imaging changes. Our patients with abnormal DW–PW imaging had more numerous and prolonged episodes of transient neurologic dysfunction, but this difference did not reach statistical significance. This suggests that clinical characteristics of TIA may not be useful to triage patients for MR with DW and PW imaging. Although the patients with mismatch had an overrepresentation of coronary artery disease and hyperlipidemia, the number of cases was small. Another issue is whether or not the presence of DW–PW imaging abnormalities herald grim outcomes, but this question transcends the constraints of the present study.
Conclusion
This retrospective study of patients with TIA shows that MR with DW and PW imaging can improve the documentation of brain ischemia and may have the potential to determine which patients have brain tissue at risk for infarction and therefore, may require close observation in the hospital or need aggressive intervention. A prospective study by using follow-up neuroimaging is required to confirm the validity of these suggestions.
Acknowledgments
This article is dedicated to the enduring memory of Carlos J. Abad “Whom the gods love dies young” Plautus, The Two Bacchises.
Footnotes
Supported in part by a Beginning Grant-in-Aid (Number: 0265450U) from the Mid-Atlantic Affiliate Research Committee of the American Heart Association (to L.R.), grants from the NIH (T32CA09630 to M.A.J and P41RR15241 to P.B.B.) and a gift from the Rogers Wilbur foundation (to R.J.W).
References
- Received December 15, 2003.
- Accepted after revision May 18, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Acute Transient Vestibular Syndrome: Prevalence of Stroke and Efficacy of Bedside Evaluation
- Imaging Recommendations for Acute Stroke and Transient Ischemic Attack Patients: A Joint Statement by the American Society of Neuroradiology, the American College of Radiology, and the Society of NeuroInterventional Surgery
- Perfusion MR Predicts Outcome in High-Risk Transient Ischemic Attack/Minor Stroke: A Derivation-Validation Study
- Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association
- Automated Perfusion Imaging for the Evaluation of Transient Ischemic Attack
- Acute Perfusion and Diffusion Abnormalities Predict Early New MRI Lesions 1 Week After Minor Stroke and Transient Ischemic Attack
- Multiple Inflow Pulsed Arterial Spin-Labeling Reveals Delays in the Arterial Arrival Time in Minor Stroke and Transient Ischemic Attack
- Early Diffusion Weighted MRI as a Negative Predictor for Disabling Stroke After ABCD2 Score Risk Categorization in Transient Ischemic Attack Patients
- Validation and Refinement of the ABCD2 Score: A Population-Based Analysis
- Definition and Evaluation of Transient Ischemic Attack: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease: The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists.
- Does Diffusion-Weighted Imaging in Transient Ischemic Attack Patients Improve Accuracy of Diagnosis, Prognosis, or Both?
- Yield of combined perfusion and diffusion MR imaging in hemispheric TIA
- Comparing two methods for assessment of perfusion-diffusion mismatch in a rodent model of ischaemic stroke: a pilot study
- Systematic Review of Associations Between the Presence of Acute Ischemic Lesions on Diffusion-Weighted Imaging and Clinical Predictors of Early Stroke Risk After Transient Ischemic Attack
- Perfusion MRI Abnormalities in Speech or Motor Transient Ischemic Attack Patients