
Abstract
Summary: Congenital or nonatherosclerotic dolichoectasia is a rare condition; its etiology, natural history, and indications and technique of treatment are not yet clarified. During a workup for recent headaches and left-sided paresthesia in a 48 year-old female patient, brain MR imaging and cerebral angiography showed a large dolichoectasia of the P2 segment of the right posterior cerebral artery (PCA). The patient passed endovascular testing for occlusion of P2 with both balloon test occlusion and selective amytal testing. Endovascular coil occlusion of the right PCA dolichoectasia was successfully performed with hydrogel coils.
Dolichoectasia, which is elongation and fusiform dilatation of the intracranial vessels, has an incidence of 0.06–5.8% (1–4). Several types of dolichoectasia are distinguished—atherosclerotic and congenital types—the latter seen in younger patients without atherosclerosis or other known causes of cerebral aneurysms (5–7). A third type, resulting from dissection, can present with a dolichoectactic appearance (8–9). Atherosclerotic dolichoectasia is the more common type and is seen predominantly in the proximal vertebrobasilar arteries followed by internal carotid arteries. The age at onset is usually greater than 40 years with a male predominance (1, 3, 6, 10, 11). The congenital type is more rare and generally found in people younger than 40 years, with a female predominance; it more frequently involves distal branches of the cerebral arteries and is possibly more common in the posterior cerebral arteries (PCAs; 5, 6, 7, 12).
Atherosclerotic dolichoectasia presents with symptoms resulting from mass effect on adjacent brain stem and cranial nerves, with stroke from thromboembolism and thrombosis of perforating branches, and rarely with subarachnoid hemorrhage from rupture. Others present with nonlocalizing symptoms of headaches, seizures, and dementia (1, 3, 7). Congenital and dissecting dolichoectasia presents with similar symptoms but possibly with a greater proportion with subarachnoid hemorrhage, 17–27% versus 10% (1, 7–9, 12). Management is controversial, with options reported that include observation with follow-up, proximal occlusion, proximal and distal occlusion (trapping), resection with reanastomosis, transposition, and wrapping (7, 8, 12, 13).
Case Report
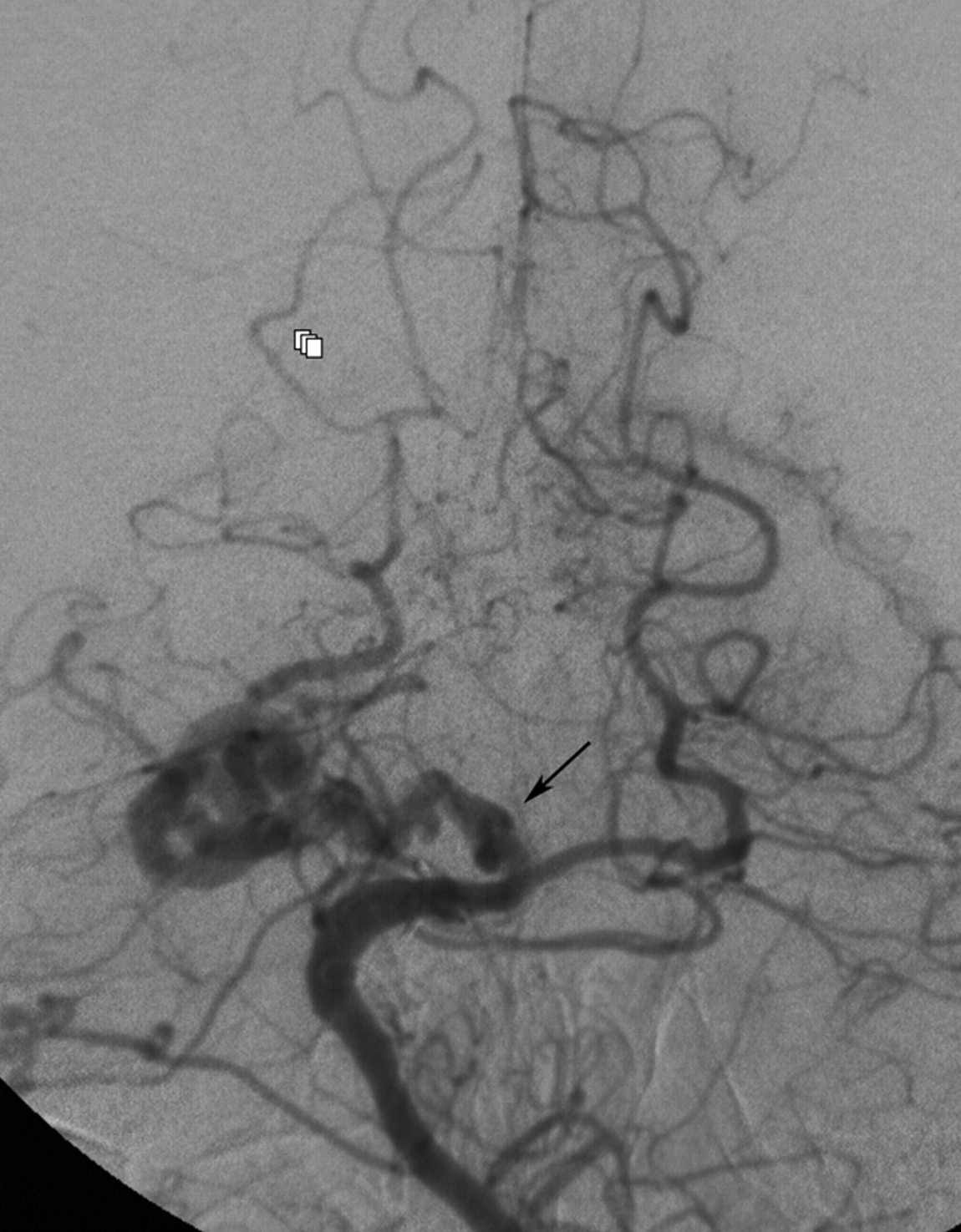
A 48-year-old right-handed female patient with a right aortic arch and history of tetralogy of Fallot repair as a child presented with recent episodes of severe headaches that resolved and episodes of left-sided numbness. On examination, the patient had no neurologic deficit. MR imaging of the brain was performed, which demonstrated tortuous dilated vessels in the right perimesencephalic region and mass effect on the brain stem. Cerebral angiography demonstrated a right proximal PCA dolichoectasia of the P2 segment supplied by a patent P1 segment and posterior communicating artery (Fig 1). Other areas of milder dolichoectasia were present with mild enlargement and tortuosity involving the right intracranial internal carotid artery, basilar artery, and distal right anterior inferior cerebellar artery.

Anteroposterior left vertebral angiogram demonstrates the right PCA dolichoectasia (arrow) just distal to the P1 segment. Mild dolichoectasia of the basilar artery and distal right anterior inferior cerebellar artery is also present.
After consultation with neuroscience specialists with backgrounds in neurology, neurosurgery, and interventional neuroradiology, a diverse range of management options were considered. Those who felt observational follow-up to be appropriate felt from their experience with a limited number of patients with this disorder, that the risk of subarachnoid hemorrhage was low and that the main risk of the disease was progressive increase of mass effect. Others saw this entity to be like a saccular aneurysm, with a propensity for catastrophic rupture. These options were presented to the patient with the uncertainty of the natural history based on current medical knowledge. The patient preferred endovascular occlusion after a series of endovascular testing to confirm a low therapeutic risk.
A balloon test occlusion was performed (Hyperform balloon 4 mm × 7 mm; Micro Therapeutics, Irvine, CA) in the proximal aspect of the P2 segment followed by selective Wada testing performed by injection of 30 mg of sodium amytal in the same location. The patient developed only a left homonymous hemianopsia during the selective Wada testing. Therefore, coil occlusion was performed of the PCA dolichoectasia with three hydrogel coils (Microvention, Aliso Viejo, CA). The patient developed no complication and had no recurrence of her presenting symptoms.
Discussion
Dolichoectasia defined as dilatation and elongation, and thus tortuosity of the vessel, may be the end product of different pathologies that weaken the vessel wall. Histologic findings suggest distinct etiologic subtypes of dolichoectasia, an acquired type from atherosclerosis and a congenital type with additional deficiencies in the muscular media layer (2, 5, 10, 14, 15). A third type resulting from dissection demonstrates intramural hemorrhage (8, 9).
Although thought to be rare, the risk of subarachnoid hemorrhage with dolichoectasia specifically with the congenital type, may be higher than previously thought (7, 12, 15). In a series of 31 patients with dolichoectasia, two presented with subarachnoid hemorrhage. The type of dolichoectasia was not identified (1). In a more recent series of 11 patients with congenital dolichoectasia, three presented with subarachnoid hemorrhage (7). Furthermore, in a large series of 120 fusiform aneurysms, of which 111 were nonatherosclerotic, 20% present with subarachnoid hemorrhage. Although, some of the cases may in fact have been giant saccular aneurysms rather than dolichoectasia, some evidence suggests giant saccular aneurysms belong to the spectrum of the same disease (10, 12, 13). A dissecting aneurysm would be another possible diagnosis and may account for the high rate of subarachnoid hemorrhage in some series with relatively low rates of subarachnoid hemorrhage in actual congenital dolichoectasia (7–9). Our case did not have the appearance of dissection with intramural hemorrhage, and similar but less extensive morphological analysis in other vessels in this patient suggests a congenital origin.
The patient opted for endovascular treatment rather than follow-up. Proximal occlusion of the PCA has been performed surgically and is usually well tolerated (7, 12). Complications from occlusion of the P2 segment may develop secondary to occlusion of a perforator or from distal hemodynamic failure. Thus, double testing was performed; a balloon test occlusion of P2 at the origin of the dolichoectasia demonstrated excellent collateral from the middle cerebral artery pial anastomosis. Also, the amytal test, performed by injection of amytal at the origin of the dolichoectasia, resulted in hemianopsia but no other motor, sensory or memory deficit, which suggests that no perforator arose from the dolichoectasia.
Conclusion
Congenital dolichoectasia, a rare cerebrovascular disorder, has an uncertain natural history and experience is limited. Parent artery occlusion may offer effective low risk treatment if test occlusion is carefully performed.
References
- Received January 30, 2004.
- Accepted after revision March 7, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}