
Abstract
Summary: Intrathoracic meningocele is rare and is usually associated with neurofibromatosis type I. Most of the reported thoracic meningoceles are not strictly anterior in location, but also lateral or anterolateral. We report a case of true anterior thoracic meningocele with no associated generalized mesenchymal dysplasia.
A spinal meningocele is a herniation of the meninges through a foramina or a defect in the vertebral column and is frequently located posteriorly in the lumbosacral area. An anterior spinal meningocele is rare and is generally described in the thoracic or sacral region. These frequently occur as a manifestation of generalized mesenchymal dysplasia such as neurofibromatosis type 1 (NF-1) or Marfan syndrome and rarely as an isolated defect. We report the imaging findings of a patient with an isolated anterior thoracic meningocele.
Case Report
A 12-year-old boy complaining of palpitation and shortness of breath aggravated by exertion was found to have diminished breath sounds in the upper chest. No focal neurologic signs or clinical evidence of NF-1 or Marfan syndrome were found on physical examination. Laboratory findings were within normal limits. The chest radiograph showed a round homogeneous mass in the upper mediastinum along with multiple vertebral segmentation anomalies and widening of the spinal canal between T5–T11 vertebrae. CT and MR imaging confirmed the spinal canal widening, the presence of multiple thoracal vertebral segmentation anomalies and a large anterior meningocele herniating in to the thoracic cavity through a bone defect at the level of T7–T10 vertebrae (Figs 1 and 2). The cystic cavity was adjacent to the right main bronchus and the main vessels of the mediastinum, and it displaced the heart into the left hemithorax.

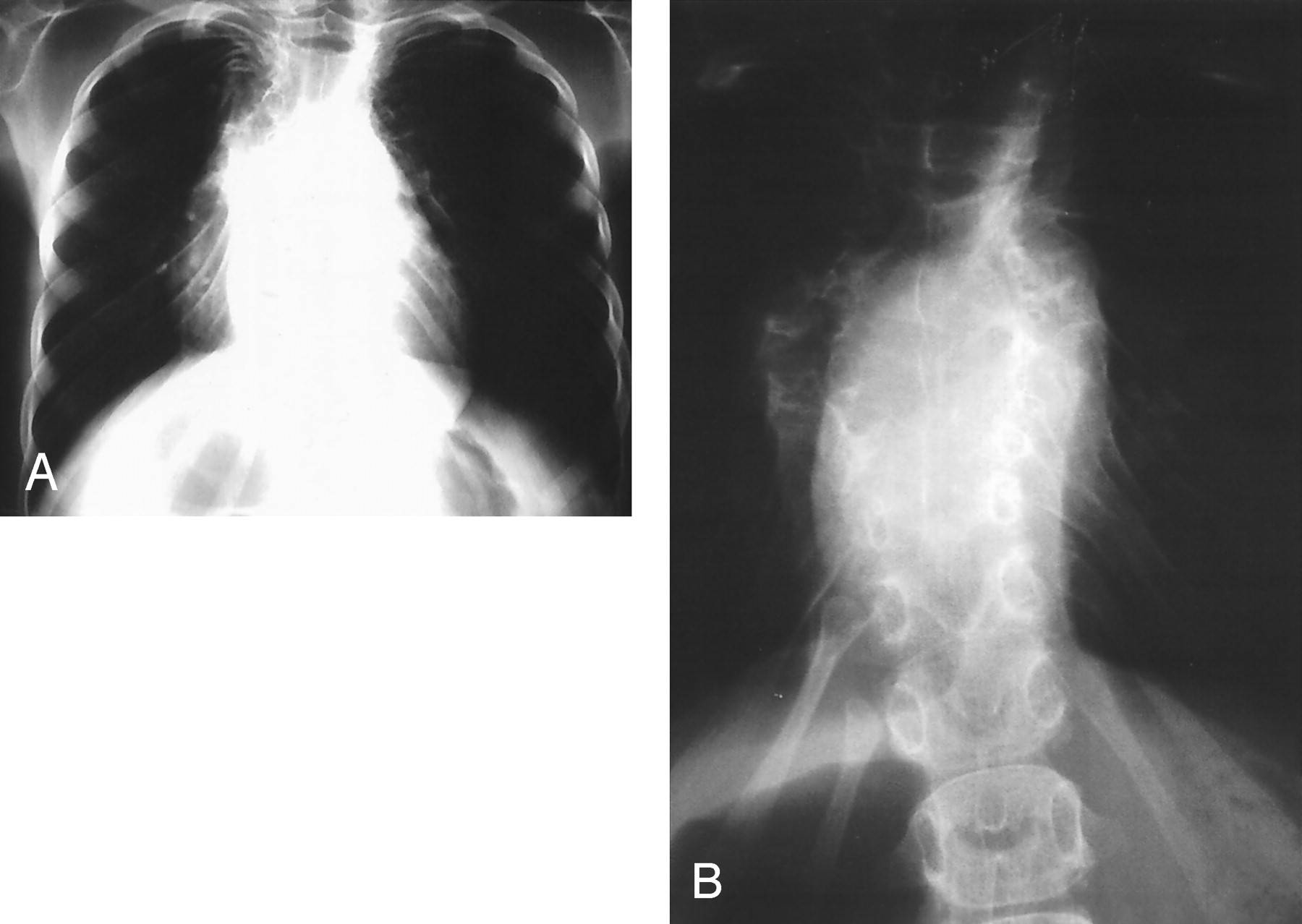
Conventional radiograph (A) shows a round homogeneous mass in the upper mediastinum. Thoracal roentgenogram (B) clearly depicts the underlying vertebral segmentation anomalies along with widening of the spinal canal at the same level.

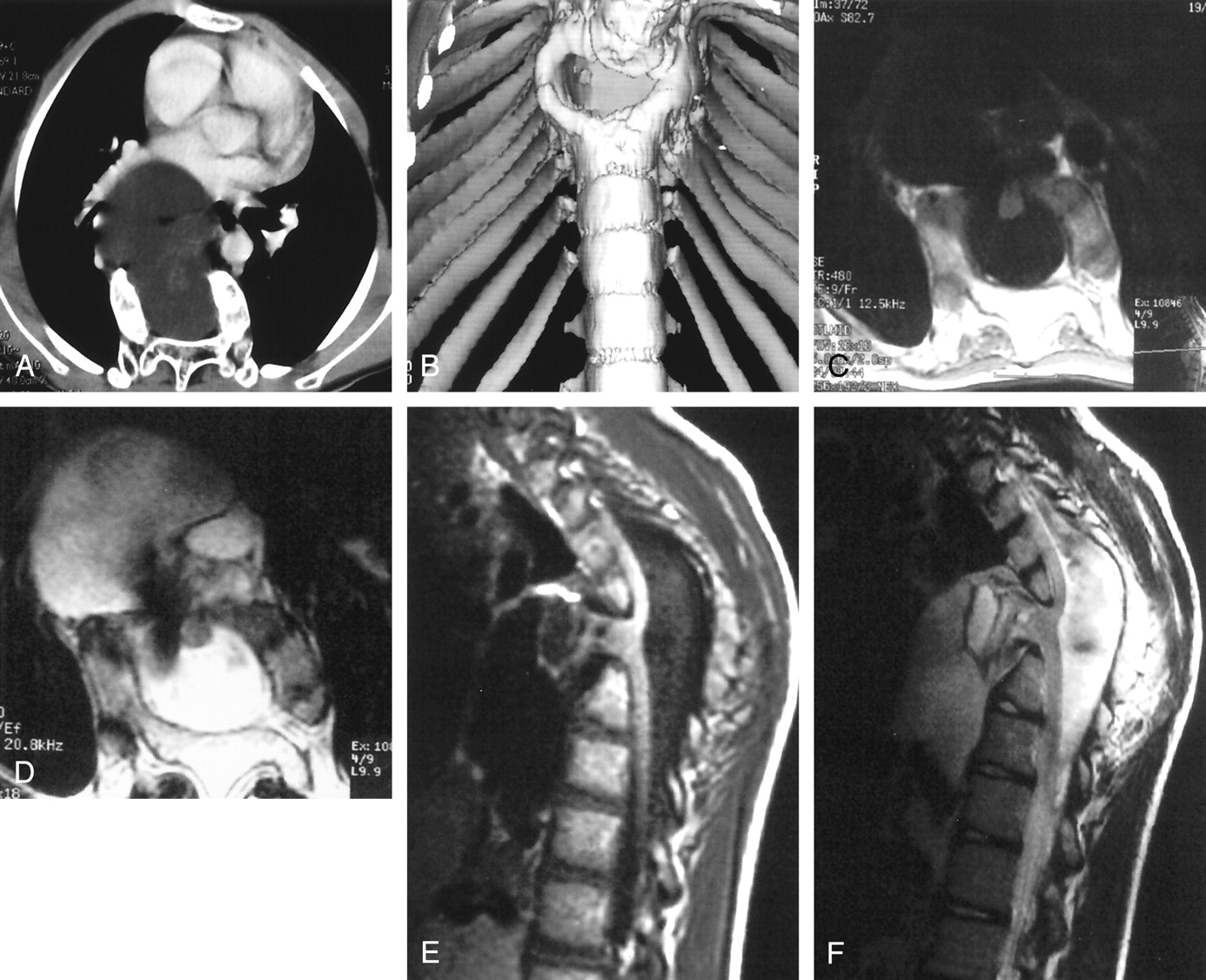
Axial CT image (A), 3D view generated from the CT images (B), axial T1 and T2-weighted images (C and D), sagittal T1 and T2-weighted images (E and F) clearly demonstrate multiple segmentation anomalies and a large anterior meningocele herniating through a bone defect at the level of T7–T10 vertebrae. The meningocele is at a close neighborhood of the right main bronchus, the main mediastinal vessels and slightly displaces the heart into the left hemithorax. The spinal cord is displaced toward the neck of the meningocele with a second smaller anterior cyst with fibrous tissue and septa.
The spinal cord was displaced anterior to the neck of the meningocele at the level of T8 vertebra. A second, smaller cyst, closely located at the anterior part of the cord, surrounded with fibrous tissue and septa, was also present. No apparent parenchymal signal intensity change or syrinx was observed in the spinal cord. In light of its size and location, the meningocele was treated surgically with an anterior approach. Following a right anterolateral thoracotomy the cystic mass adherent to the T8 vertebra corpus was exposed. The cystic mass was extirpated, and the dura was closed with sutures. A distraction cage was applied between the thoracal vertebrae that showed fusion anomaly (Fig 3). Following surgical intervention, the dyspnea and palpitation disappeared, and the patient remained asymptomatic.

In axial CT (A), sagittal T1-weighted (B), and axial T2-weighted (C) MR images obtained 2 months after surgery, the meningocele cavity is no longer observed and the bone defect is now obstructed by the distraction cage applied. The spinal cord is still displaced anteriorly in the spinal canal. Note the artifacts generated by the surgical implant on MR images.
Discussion
A spinal meningocele is a herniation of meninges through bone defects or foramina to form a CSF-filled sac. An acquired meningocele is a comparatively common laminectomy complication, whereas congenital meningocele is a relatively rare developmental anomaly (1). Although there are several theories, their embryologic origin is still unclear. More than 80% of spinal meningoceles are located posteriorly in the lumbosacral area. Anterior meningoceles are rarer and are described generally in the thoracic and sacral region. Most of the reported thoracic meningoceles are not strictly anterior in location, but lateral in origin, with a secondary forward projection of a dural herniation usually passing through a previously enlarged intervertebral foramen (2). The thoracic meningocele described in our report does not pass through an enlarged foramen, but rather through a wide midline bony defect of the vertebral bodies and is therefore a true anterior thoracic meningocele.
In their review of the literature, Andrade et al (3) found 134 cases of intrathoracic meningoceles reported before 1992. They stated that 69% of these thoracic meningoceles were in association with NF-1, whereas only 22% were isolated cases. In the same article, a total of 16 patients with thoracic meningocele between 1992 and 2003 were reported. Twelve of these 16 patients were together with NF-1 and the remaining four being isolated cases. The patient presented in this case report had no association with NF-1 or other generalized mesenchymal dysplasia and therefore is classified as being an isolated case of true anterior thoracic meningocele.
The clinical manifestations of a thoracic meningocele are closely related with its size and its relationship with surrounding structures. It may include back pain, paraparesis from insult to the spinal cord, or shortness of breath, coughing, and palpitation by compression of the lung and mediastinal structures, as was the case for the patient presented here. Even progressive hydrothorax caused by rupture of meningoceles has been reported in the literature (4). On the other hand, in the setting of a small meningocele, no symptoms can be recorded, and the lesion may be incidentally diagnosed on a routine chest radiograph.
Although there are still conflicts concerning their treatment, it is widely accepted that excision of the lesion is indicated in the presence of progressive neurologic deficit, respiratory distress or rapid progress in the size of the meningocele (4, 5). The decision for the surgical approach is closely related with the lesion size. For small and medium-sized meningoceles, the most common approach is through a laminectomy and an intradural repair of the cyst, with the advantage of avoiding a thoracotomy. The posterior approach is inadequate for larger lesions, as in the case presented here, and a transthoracic access is indicated because it offers a larger operating field with a small chance to damage the spinal cord (3, 6, 7). Regardless of the treatment decision, cross-sectional imaging techniques, such as CT and MR imaging are essential, not only for the diagnosis, but also for the depiction of its relationships to surrounding structures and the exclusion of other possible accompanying lesion such as neuroma in the setting of NF-1. In the case presented here, segmentation anomalies and widening of the spinal canal caused by the thoracic meningocele was first noticed on a chest radiograph, but the final diagnosis, with its anatomic relationships, was made possible by CT and MR imaging.
- Received February 11, 2004.
- Accepted after revision March 12, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.