
Abstract
Summary: We report a case of angiotropic large cell lymphoma (ALCL) with central system involvement in which there was initially an isolated spinal cord stroke with paraplegia. MR imaging of the spinal cord demonstrated increased signal intensity in the center of the cord on T2-weighted images and subsequently a cerebral lesion in the right temporal lobe. The diagnosis of ALCL was established by brain biopsy. An enlarged spinal cord with enhancement after administration of contrast material and increased signal intensity on T2-weighted images, while not specific for ALCL, may be the first imaging findings of that disease.
ALCL is a rare systemic disease in which there is partial or complete occlusion of blood vessels by neoplastic cells. The histogenesis of the neoplastic cells in the malignant lymphoma is most commonly B-cell lineage. The diagnostic imaging of ALCL is nonspecific; often the diagnosis of ALCL is established on postmortem histologic studies (1, 2). We describe the clinical course of a patient with ALCL in which the initial central nervous system involvement was limited to the spinal cord. The diagnosis was established by brain biopsy, and we performed serial spinal cord and brain MR imaging throughout the disease evolution. Clinical stabilization was achieved by means of rapid diagnosis and chemotherapy. The patient was still alive 19 months after the onset of the disease and was considered to be in complete remission.
Case Report
A 71-year-old woman with a non-significant medical history presented gradually over 2 weeks with a sensory disturbance of the lower extremities, rapidly followed by motor weakness of the lower limbs, anal incontinence and dysuria. Paraparesis was found on clinical examination; her reflexes were symmetrical and abnormally brisk in the lower limbs, associated with bilateral extensor plantar responses. Initial MR imaging of the lower spinal cord showed a thick conus with increased signal intensity on the T2-weighted images (Fig 1A) and without enhancement after administration of Gd-DTPA (Fig 1B). Spinal cord ischemia was suspected; a spinal angiogram was obtained to search for an arteriovenous shunt or vasculitis but no evidence of vascular abnormality was found. Two CSF samples were normal with no increased protein level. Steroid injections (solumedrol 1 mg/kg) were administered for 5 days during the beginning of the clinical course with no evidence of patient improvement. During 3 weeks, we clinically observed a worsening of the sensory disturbance and a complete paraplegia with T10 sensory level and saddle anesthesia. Repeat spinal cord and cerebral MR imaging was performed showing spinal cord thickening associated with a signal intensity abnormality: increased signal intensity on T2-weighted images (Fig 2A–C), isointense signal on T1-weighted images without enhancement (Fig 2D) involving the cervical, thoracic, and conus areas. The lesions had increased in size and in number compared with those on the first MR image; findings of the initial cerebral MR imaging were normal. Findings of 3D time-of-flight MR angiography of the spino-cranial junction were also normal. Biologic investigations revealed normal serum vitamin-B12 level, and antibodies including rheumatoid factor were negative. Coomb’s antiglobulin test, serum levels of lactate deshydrogenase, thyroid stimulating hormone, cortisol, folate, haptoglobin, and C3 and C4 complement levels were within normal limits. Tests for antinuclear antibodies and antineutrophil cytoplasmic autoantibodies (p-ANCA and c-ANCA) were negative as well. Infectious serologies were also negative (HIV, BHV, CHV, HTLV, CMV, EBV, Borrelia, Mycoplasma, TPHA/VDRL).

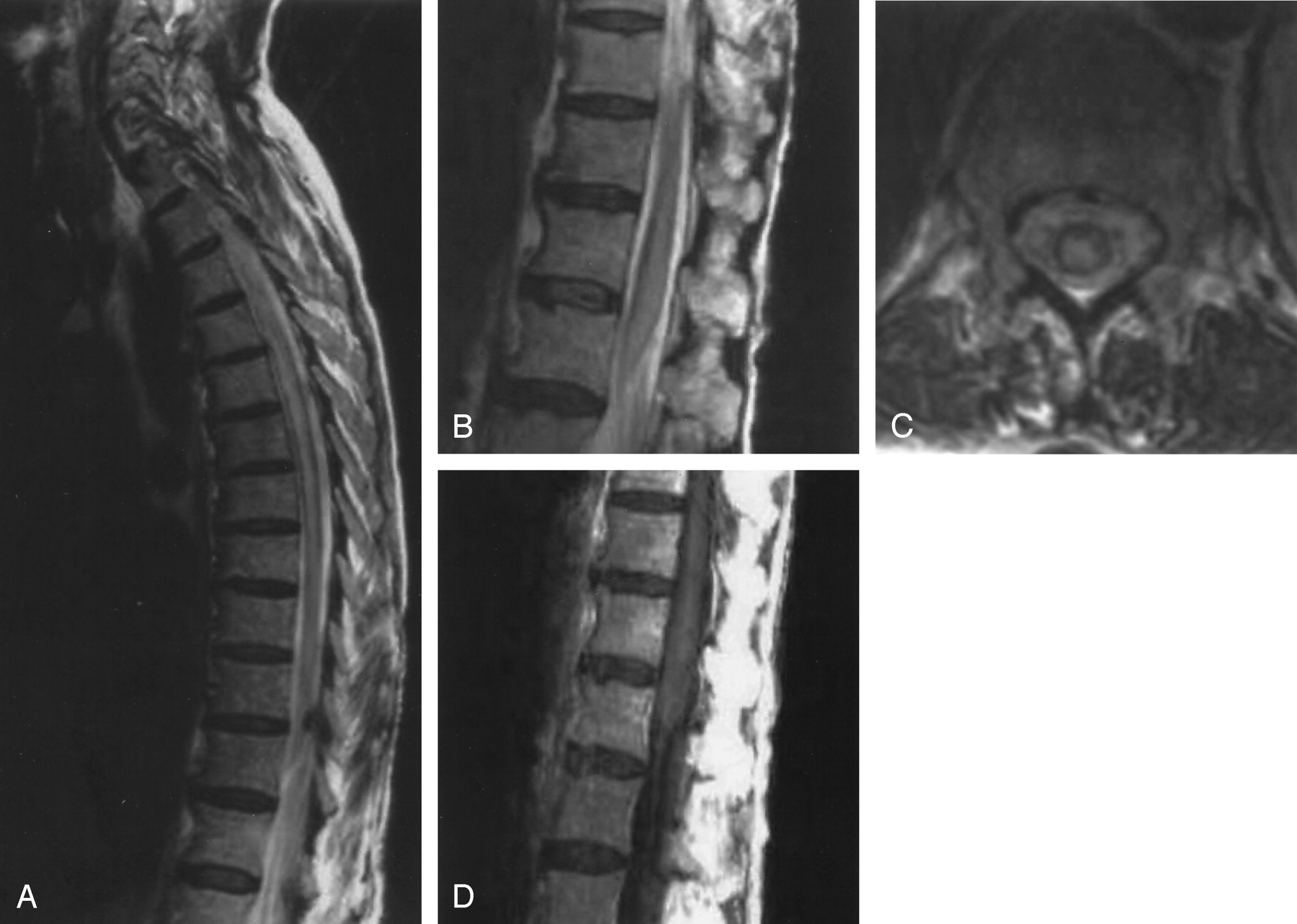
Imaging findings at initial imaging.
A, T2-weighted image shows a thick conus that is increased in signal intensity.
B, Contrast-enhanced T1-weighted image shows a thick conus without enhancement.

Imaging findings at 6-week follow-up.
A, MR image shows an enlargement of the thoracic cord associated with increased signal intensity in T2-weighted images.
B, The conus remains enlarged with signal intensity abnormality.
C, Axial T2-weighted MR image shows a central signal intensity abnormality within the cord at the T12 level.
D, There is still no enhancement of the conus following contrast medium injection.
One month later, the patient presented at the hospital with generalized seizures. A few days before, she had developed transient weakness of the left arm and a left facial paralysis. The clinical examination found paraplegia, a T6 sensory level, urinary retention, and constipation. There was no upper-extremity sensory motor deficit. The patient erythrocyte sedimentation rate (ESR) was elevated at 90 mm/h and the C-reactive protein (CRP) was also elevated at 22 IU. A urinary infection was discovered and considered to be responsible for the ESR and CRP disturbance. CSF cultures, cytological examination, and tests for Lyme disease and human immunodeficiency virus (HIV) were negative.
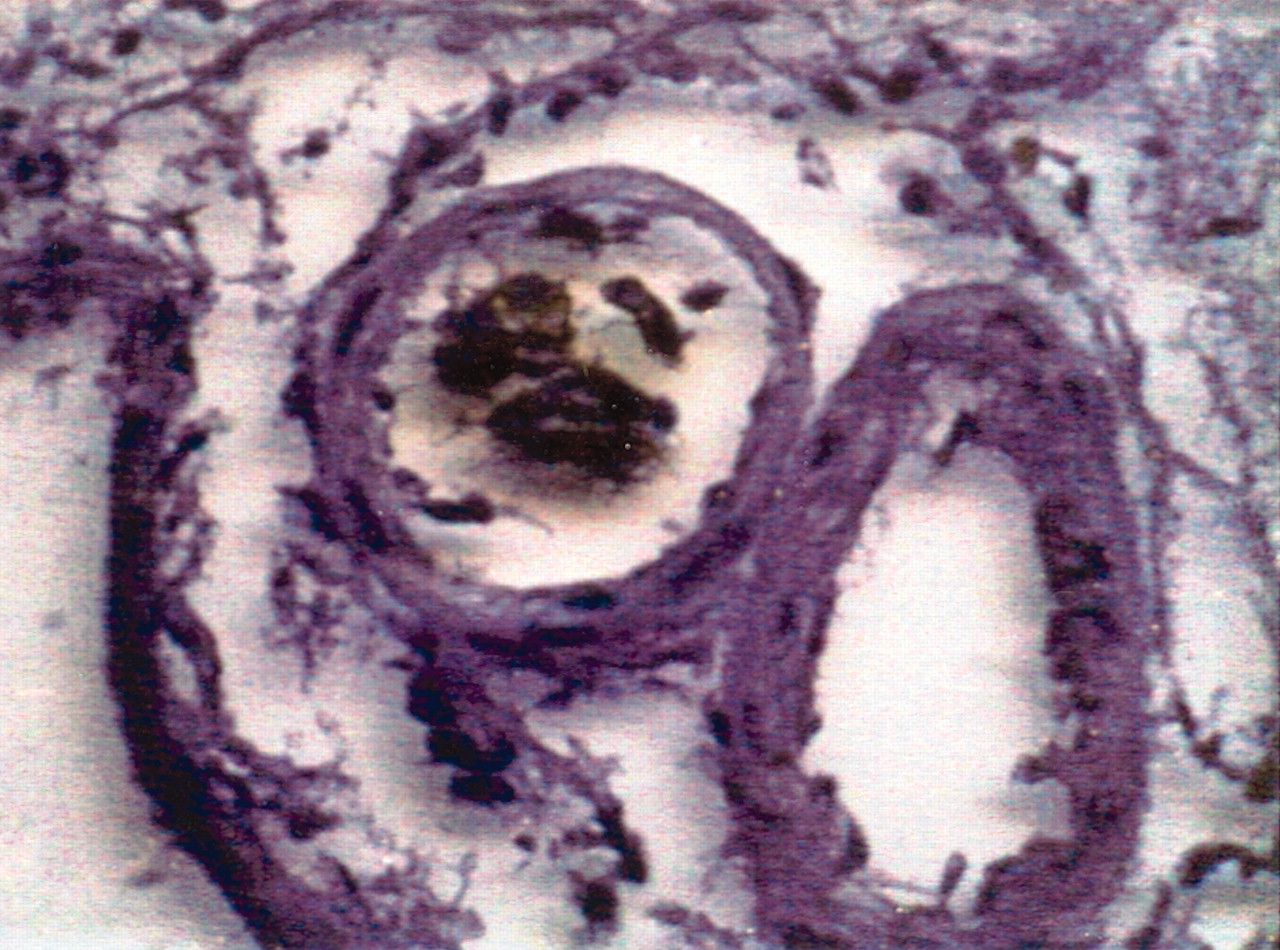
Repeat cerebral and spinal cord MR imaging showed high signal intensity on T2-weighted images (Fig 3A) in the cord and contrast enhancing (Fig 3B). The thoraco-lumbar spinal cord was still thick. In the brain, MR imaging demonstrated a right temporal high signal intensity on T2-weighted FLAIR weighted images (Fig 3C) with contrast enhancement associated with a local pachymeningitis (Fig 3D). The primary diagnosis was lymphoma. The patient underwent a craniotomy with biopsy of the right temporal lobe by neuronavigation. The biopsies contained two cortical fragments and two fragments of dura mater and microscopic examination revealed extensive plugging of arteries and veins of various sizes by a population of malignant lymphoid cells (Fig 4). Immunochemistry confirmed the B-cell phenotype of these malignant cells (CD20 positive) and the appearances were those of an intravascular B-cell lymphoma (Fig 5). After surgery, a sudden worsening of the neurologic state of the patient led us to administer new steroid boluses, which were effective over this period. Three months after the first MR imaging study, treatment with a half-dose of methotrexate etoposide BICNU solumedrol (MBVP) associating anti-emetic and folic acid was well tolerated. After a second similar treatment, a new MR imaging examination was performed (Fig 6A and B).

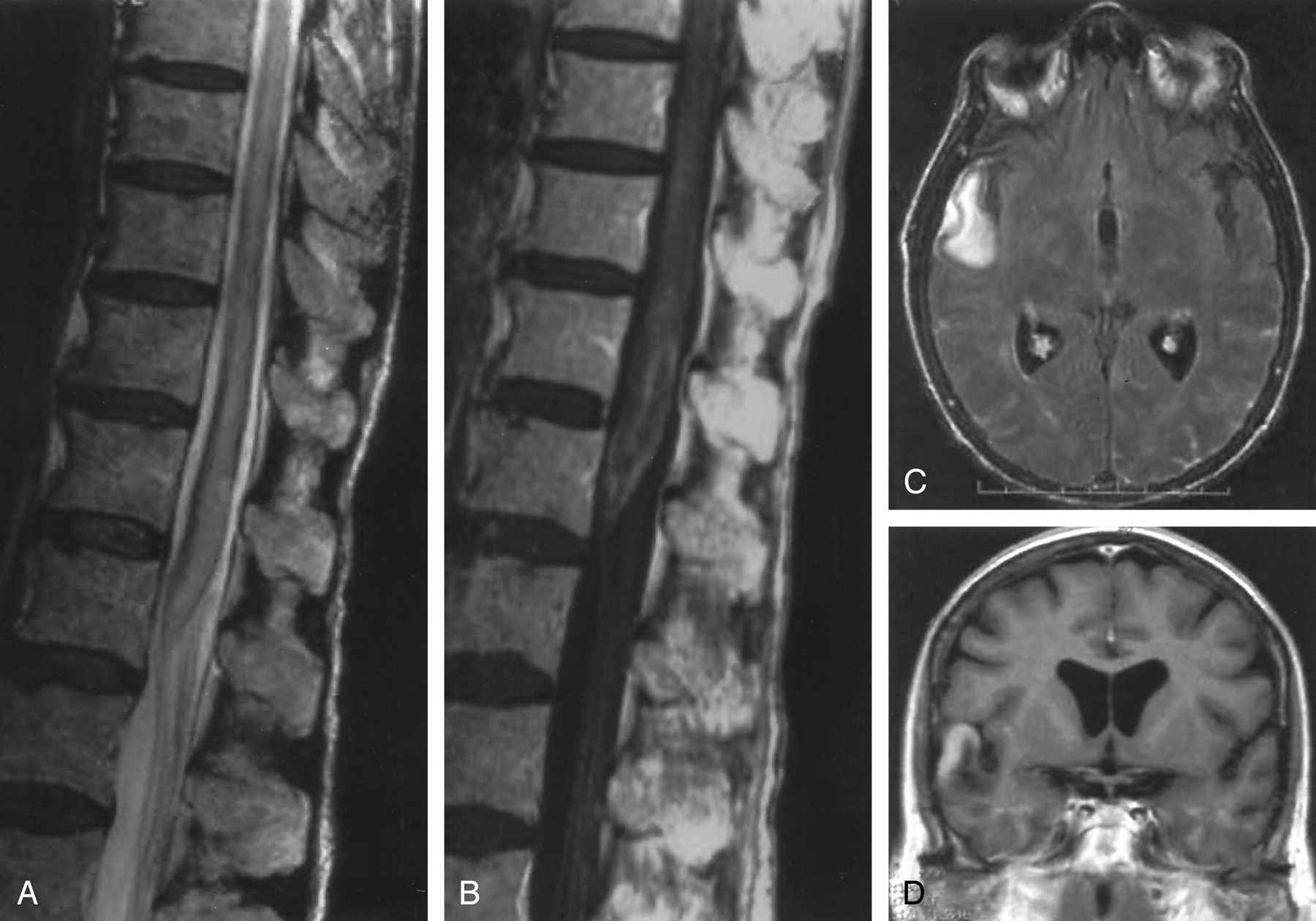
Imaging findings at 10-week follow-up.
A, There is an extension of spinal cord thickening on T2-weighted images.
B, Abnormal enhancement after Gd-DTPA injection on T1- weighted images.
C, T2-weighted FLAIR weighted image shows appearance of a right temporal lesion.
D, Postcontrast T1-weighted image shows lesion enhancement.

Large tumor cells in the lumen of small vessels of the brain (magnification ×400; hematoxylin and eosin). Biopsy fragments were taken from the right temporal lobe.

Large intravascular tumor cells express the cluster of differentiation 20,which is specific for B-cell lineage lymphocyte. (magnification ×400) (method with autoantibodies immunofixation). Biopsy fragments were taken from the right temporal lobe.

Imaging findings at 20-week follow-up.
A, T2-weighted FLAIR image following treatment shows disappearance of the previous signal intensity abnormality in the leptomeninges and in the right temporal lobe.
B, Contrast-enhanced T1-weighted image shows disappearance of prior enhancement.
Compared with the second examination of the spinal cord, the conus decreased in size, and the enhancement disappeared. There was still a signal intensity abnormality on the T2-weighted images, but these were less extensive at the thoracic and conus levels. Likewise, cerebral examination showed a disappearance of previous signal intensity abnormalities in the leptomeninges and in the right temporal lobe. Compared with the previous MR imaging examination (Table), we noticed the appearance of multiple little nodular white matter signal intensity abnormalities inside, suspected to be a demyelinated area of post-therapeutic toxic origin. Nineteen months later, the patient was in complete remission.
The dates of examination, area examined, and the findings at each time interval.
Discussion
ALCL is rare, and MR imaging is important in helping to establish the diagnosis (1–3). Unlike biologic examination, it shows early signal intensity abnormalities in the CNS locations involved, allows the ability to brush aside some differential diagnoses, shows pejorative evolution in lack of treatment, and could lead to biopsies for cellular examination.
Histologic studies reveal intravascular neoplastic cell proliferation typically found within the lumina of capillaries, venules, arterioles, and small arteries. The immune examination of these malignant cells affirms the lymphomatous origin, most commonly of B-lineage, and more rarely from T-lineage (4).
Most patients with ALCL are elderly, the average age of onset is 60 years, without sex predominance (5). This case is an illustration of the varied pattern of vascular involvement that can occur in ALCL. Most cases in the literature describe central nervous system involvement with high prevalence of confusion, rapidly progressive dementia in 75% of the cases (6–8) or epileptic seizures. In his literature review, Williams et al (8) noticed no cases of isolated spinal cord involvement associated with clinical and radiologic signs. Moreover, very few patient cases have been described with an isolated spinal cord stroke in ALCL disease.
Conclusion
Our case shows that ALCL can present as a single spinal cord stroke without involvement of cerebral structures, and should be considered in the differential diagnosis of isolated spinal cord involvement that can mimic primary angiitis of the central nervous system or a diffuse systemic necrotizing vasculitis. In our patient, no immunocompromise was described (autoantibodies and salivary gland biopsies were negative). Vitamin B12 level was normal, and all infectious serologies and blood cultures were also negative. ALCL prevalence is unknown, and it is probable that many cases are not diagnosed because of the rapid evolution of the disease to patient death and because of the difficulty in establishing an antemortem histologic diagnosis (2, 11, 12). In the literature available, most ALCL diagnoses are established post mortem. In our case, the rapid diagnosis permitted the initiation of chemotherapy less than 2 months after beginning the clinical course, and it led to a clinically stable state and radiologic improvement.
Acknowledgments
We would like to thank Catherine Vinnikoff-Sonier, PhD for her MR imaging examination contribution, Christophe Destrieux, PhD for the Neurosurgery Units, Flavie Arbion, PhD for the Anatomopathology Units, and Aparna Swaminathan.
References
- Received January 21, 2004.
- Accepted after revision March 8, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}