
Abstract
BACKGROUND AND PURPOSE: Previous studies have shown that axial loading can narrow the spinal canal. However, the clinical significance is unclear. The purpose of this study was to determine whether the narrowing of the spinal canal with axial loading during MR imaging could influence treatment decision for spinal stenosis.
METHODS: Two hundred patients with clinical symptoms of spinal stenosis underwent routine MR imaging and then immediately underwent axially loaded MR imaging. We selected 20 of these patients because they had narrowing of the spinal canal shown on the axially loaded images. Three experienced neurosurgeons evaluated these 20 patients based on clinical information and routine MR images. The same neurosurgeons were then asked for second treatment decisions based on the same clinical information but with axially loaded MR images.
RESULTS: Axial loading during MR imaging of the lumbar spine can influence neurosurgeons in their treatment decisions for symptomatic spinal stenosis. For this selected group of patients, all three neurosurgeons changed their treatment decision from conservative management to decompressive surgery for five patients when shown the axially loaded MR images. For two other patients, two neurosurgeons changed their treatment decisions, and for three additional patients, one neurosurgeon changed his treatment decision, all based on the axially loaded MR images. Treatment was not changed from surgical to medical management for any of the patients when shown the axially loaded images.
CONCLUSION: In selected patients with spinal stenosis and apparent narrowing of the spinal canal shown by axially loaded MR imaging, the additional information gained from this technique can influence experienced neurosurgeons in their treatment decisions.
Stenosis of the lumbar spinal canal may cause low back pain, sciatica, and neurogenic claudication. The symptoms are often induced by walking, standing, or hip extension. Typically, these patients experience fewer symptoms when bending forward, squatting, or lying supine with hip flexion. Alteration of symptoms related to position have led authors to think that imaging in the most symptomatic position might yield more diagnostic information than imaging in a psoas relaxed neutral position. MR imaging and CT are, with few exceptions, performed with the patient in a supine position, often with slight hip and knee flexion to improve the patient’s comfort during imaging.
It is well known from clinical work that a number of patients with significant symptoms do not have corresponding imaging abnormalities, even with the most sophisticated techniques. To simulate upright position, clinicians and researchers have developed a device (DynaWell L-spine; DynaWell Int. AB, Billdal, Sweden) (Fig 1) that loads axially to the spine in the supine position (1–5). This device consists of a harness/jacket with straps connected to a footplate. By tightening the straps, an axial load can be applied to the patient’s spine during imaging.

Patient in position during axial compression.
A and B, Device consists of nonmagnetic harness/jacket with straps connected to a footplate. By tightening or loosening the adjustment knobs on the compression part, the load can be regulated and equally distributed to both legs. The applied load can be measured by using scales on the footplate.
Several previous studies have shown that the use of this device can cause narrowing of the spinal canal and apparent accentuation of spinal stenosis when compared with routine MR imaging techniques (1–4). However, the clinical significance of this narrowing is not fully understood. To gain a better understanding of the importance of increased spinal stenosis that occurs with axial loading, we applied this technique to >200 patients with signs and symptoms of spinal stenosis. We selected 20 patients with apparent narrowing of the spinal canal on the axially loaded images. Three experienced neurosurgeons evaluated these patients based on clinical information and initial routine MR images and provided treatment recommendations. Thereafter, we asked the same neurosurgeons for second treatment recommendations based on the same clinical information but with the axially loaded MR images included. The purpose of this study was to determine whether axial loading during MR imaging of the lumbar spine could influence treatment decisions for spinal stenosis.
Methods
Patients
In our clinical work, we applied axial loading during MR imaging studies of >200 patients with signs and symptoms of spinal stenosis. The criteria for obtaining axially loaded MR images of these patients were low back pain, sciatica or neurogenic claudication, and spinal stenosis shown by routine MR imaging. The axially loaded images were considered to be part of the clinical imaging protocol at this institution (Sahlgrenska University Hospital, Göteborg, Sweden), and institutional review board approval was not obtained. For this study, we selected 20 patients in whom we detected appreciable differences in the caliber of the dural sac on the routine and the axially loaded MR images. The patient group was comprised of 14 men and six women ranging in age from 32 to 75 years, with a mean age of 54 years. Thirteen patients had sciatica, 11 had low back pain, and eight had neurogenic claudication. Two patients had histories of laminectomy at L3–L4 and L4–L5.
Imaging and Axial Loading
MR imaging was performed on a 1.0-T system using a surface coil. Routine MR imaging consisted of axial T2-weighted (4200–8249/119–130/2–3 [TR/TE/number of excitations]) and/or T1-weighted (583–960/12–15/2–3) turbo spin-echo sequences, with an imaging matrix of 210–256 × 256, field of view of 188–285 × 188–285 mm, and section thickness of 4 mm with an intersection gap of 0.4 mm. For the routine MR imaging, the patient was placed supine with slight hip flexion and with a small pillow under the knees.
After the routine MR imaging, axial loading was applied by using a United States Food and Drug Administration approved commercially available device (DynaWell L-spine; DynaWell Int. AB, Billdal, Sweden) (Fig 1) (1–5). This device comprised a nonmagnetic harness/jacket with straps connected to a footplate and a compression mechanism. The harness/jacket was available in four sizes to secure optimal fitting. This harness/jacket was applied to the patient before he or she entered the MR imaging unit, but the loading was not applied during routine MR imaging.
For the axially loaded imaging, the patient was lying in the same supine position. The feet were placed against the footplate and axial load was applied by stretching the side traps by turning the adjustment knobs on the foot plate. We applied approximately 50% of the patient’s body weight distributed equally to both legs according to recommendations in previous studies (1–6). Thus, in a 100-kg patient, we applied 25 kg of axial load to each leg. The load was applied for 5 min, and then axial view T1- and/or T2-weighted MR images were obtained according to the same protocol. The patients were instructed to take their regular pain medication, and we routinely did not use additional pain medication.
Image Interpretation
Three experienced neurosurgeons (R.S.B., T.G.R., W.H.P.) evaluated these 20 patients based on clinical history and routine MR images. The neurosurgeons had at least 20 years of attending experience treating patients with back pain. The neurosurgeons were initially asked to provide treatment decisions based on the clinical information and the routine MR images only. Thereafter, the axial loaded images were placed next to the routine MR images and the neurosurgeons were again asked for treatment decisions.
Results
The additional information gained from the axially loaded images included deformation of the dural sac (12 patients), narrowing of the lateral recess (eight patients), increased disk protrusion (three patients), and visualization of a synovial cyst (one patient). Additional information gained from axial loading during MR imaging of the lumbar portion of the spine can influence experienced neurosurgeons in their treatment decisions for patients with symptomatic spinal stenosis. In our study, all three neurosurgeons changed their treatment decision from conservative management to decompressive surgery for five of 20 patients when shown the axially loaded MR images (Figs 2 and 3). For two other cases, two neurosurgeons changed their treatment decision, and for three additional patients, one neurosurgeon changed his treatment decision, all based on the axially loaded MR images. No change of treatment decision was made for the 10 remaining patients (Fig 4). No decision was made to change from surgical to medical management based on the axially loaded images.

Routine and axially loaded MR images of a 56-year-old man with bilateral sciatica and claudication. All three neurosurgeons changed the treatment decision from conservative therapy to decompression surgery for this patient based on the additional information provided by the axially loaded MR images.
A, Routine T2-weighted image obtained at L4–L5 shows mild spinal stenosis.
B, Axially loaded T2-weighted image obtained at L4–L5 shows severe spinal stenosis, deformation of dural sac and bilateral lateral recesses, and prominence of the dorsal fat pad.

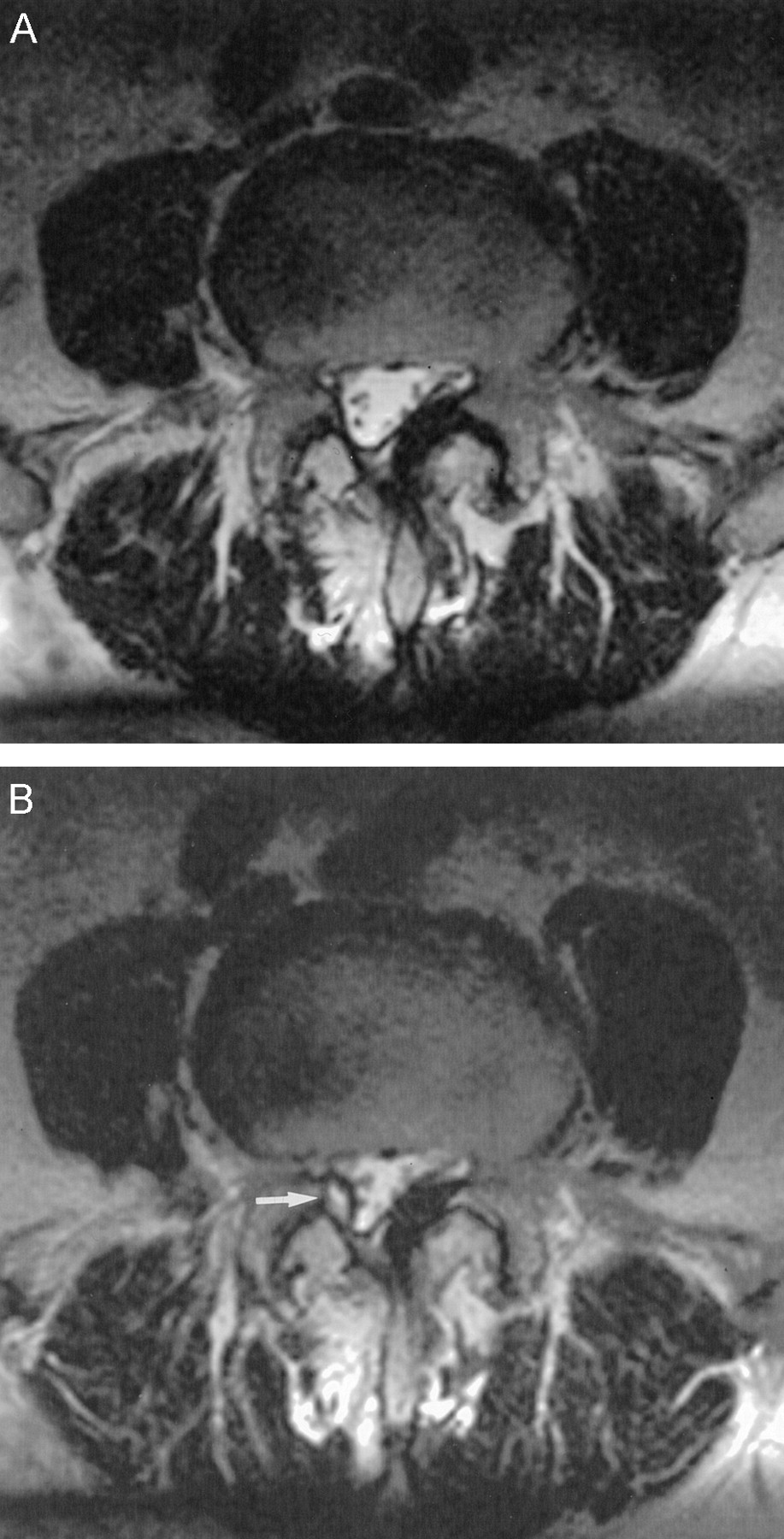
Routine and axially loaded MR images of a 75-year-old man with right sciatica. Decompression surgery had been performed 2 years before this study. All three surgeons changed the treatment decision from conservative therapy to decompression surgery based on the additional information provided by the axially loaded images.
A, Routine T2-weighted image obtained at L4–L5 shows deformation of dural sac and thickening of ligamentum flavum, especially on the left side.
B, Axially loaded T2-weighted image obtained at L4–L5 shows a right synovial cyst (arrow) that was not shown by the routine MR image. Prominent deformation of the dural sac and thickening of the ligamentum flavum can be seen.

Routine and axially loaded MR images of a 54-year-old man with right sciatica and claudication. None of the three neurosurgeons changed the treatment decision based on the information provided by the axially loaded images.
A, Routine T2-weighted image obtained at L4–L5 shows mild spinal stenosis and bilateral foraminal stenosis.
B, Axially loaded T2-weighted image obtained at L4–L5 shows minimal accentuation of spinal stenosis.
Discussion
The pathophysiological reason for the worsening of symptoms of spinal stenosis while walking or standing has been thought to be narrowing of the spinal canal and crowding of the nerve roots. On the other hand, the cause of improvement while bending forward has been postulated to be enlargement of the spinal canal and reduction of the pressure on the nerve roots (7–11). When myelography was the standard imaging procedure for evaluation of spinal stenosis, it was common to use an upright position during imaging. When MR imaging and CT replaced myelography in most cases, we lost the opportunity to image in the most symptomatic position. The results of our study suggest that some of the disadvantages of the supine position can be overcome by applying axial loading during MR imaging.
Several previous studies have shown that axial loading actually decreases the cross-sectional area of the spinal canal in a large proportion of patients with spinal stenosis (1–4, 10, 11). The common reason for this accentuation of spinal stenosis is thickening of the ligamentum flavum, accentuation of a bulging disk, and thickening of the dorsal fat pad, which result in deformation of the dural sac. In our clinical work, we saw examples of all these reasons for narrowing of the spinal canal. Therefore, axial loading during imaging in a supine position seems to be logical and reasonable for patients with signs and symptoms of spinal stenosis.
Willén and Danielson (4) reported “additional valuable imaging information” for 29% of the symptomatic patients, which is in agreement with our observations. However, no previous study has attempted to determine the influence of these imaging findings on treatment decisions. Our study has shown that additional information obtained from axial loading during MR imaging of the lumbar spine can influence experienced neurosurgeons in treatment decisions for symptomatic spinal stenosis. The 20 patients in our study were selected because apparent narrowing of the spinal canal was shown with axial loading. The results can therefore not be used to gauge the incidence of change in treatment decision that would happen if this technique were applied to a larger group of patients. This will be very dependent on the patient selection for axial loading. If we had analyzed the entire group of >200 patients, the proportion of patients with changes in treatment approach would have been lower. The purpose of our study was, however, to determine whether axial loading could influence treatment decision. In our current clinical practice, we use axial loading as an additional MR imaging study when routine MR imaging does not explain the patient’s signs and symptoms that are more prominent in an erect than in a supine position. This is often true for patients with neurogenic claudication with spinal stenosis. The frequency of such influence and the optimal indication for axial loading must await further studies.
It is also unknown whether the alterations in treatment would have resulted in better outcomes. We have no systematic follow-up of the surgical results of these patients. Outcome studies with axial loading are necessary before we can determine the full clinical value of this technique.
One clinical MR imaging system has been designed for use with the patient in an upright position (12). The usefulness of this system has been documented but is not fully understood. The upright position is certainly more physiological for evaluation of back pain, but the advantage of this position might be outweighed by a lower magnetic field strength and increased risk for patient motion. The comparative studies between our device and this new imaging unit should be awaited.
Disadvantages of axial loading could be increased pain and other symptoms during imaging. We observed these in a few patients, but there was no degradation of images related to motion. We did not routinely use additional pain medication for the axially loaded images. Another disadvantage of using axial loading is prolongation of the examination by 5 to 10 min. To save time, another option would be to obtain only axially loaded images, but this must await the outcome studies discussed above.
Conclusion
Additional information gained by axial loading during MR imaging can influence treatment decisions. The frequency of changes in treatment decision, the optimal indication for axial loading, and the surgical outcomes must await further studies.
References
- Received January 20, 2003.
- Accepted after revision May 16, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Increased Facet Fluid Predicts Dynamic Changes in the Dural Sac Size on Axial-Loaded MRI in Patients with Lumbar Spinal Canal Stenosis
- Radiculopathy
- Dynamic Changes in the Dural Sac Cross-Sectional Area on Axial Loaded MR Imaging: Is There a Difference between Degenerative Spondylolisthesis and Spinal Stenosis?
- Radiculopathy