
Abstract
BACKGROUND AND PURPOSE: Quantitative MR imaging strategies may have considerable potential for in vivo assessment of neuropathologic changes associated with HIV. This investigation evaluated the prognostic significance of whole brain histogram-derived diffusion tensor imaging indices with respect to severity of cognitive impairment and measures of clinical status in cases of HIV.
METHODS: Quantitative indices derived with diffusion tensor imaging, including whole brain fractional anisotropy and the apparent diffusion coefficient, were compared for six patients with HIV and eight control volunteers. Relationships between whole brain indices and specific measures of dementia severity and clinical status were examined.
RESULTS: Whole brain fractional anisotropy was reduced in patients with HIV and was significantly associated with severity of dementia, as indicated by several widely used clinical and functional status measures. Summary fractional anisotropy measures were more prognostic of dementia status than were apparent diffusion coefficient measures.
CONCLUSION: Findings from this investigation support the use of diffusion tensor imaging for noninvasive MR imaging measurement of neuropathologic changes in studies of HIV-associated cognitive impairment.
Both direct and indirect mechanisms have been implicated in neuronal injury in cases of HIV (1). These pathologic processes cannot be directly observed. The sensitivity of T1- and T2-weighted MR imaging is limited by the diffuse nature of the neuropathologic substrate in cases of HIV, and conventional MR imaging cannot be used to determine the cumulative extent of injury (2, 3). Diffusion tensor imaging provides a noninvasive means of measuring otherwise unobservable alterations in tissue status (4). The sensitivity of diffusion tensor imaging to displacements of water molecules can be used to derive parameters that reflect intrinsic structural and physiological characteristics of tissue, including pathologic changes in size, spacing, or integrity of CNS structures (5).
Measures commonly determined from the diffusion tensor include fractional anisotropy (FA), a measure of the direction-dependent mobility of water molecules, and apparent diffusion coefficient (ADC), a measure of the average diffusivity in all directions (4). Diffusion tensor imaging indices may have considerable promise for measuring changes corresponding to pathologic processes in cases of HIV, including sublethal injury to tissue. Aggregate measurements, determined across the entire brain, may have potential usefulness for summarizing overall disease burden in cases of HIV, including changes in the integrity of neuronal structures (eg, axonal processes in white matter) and changes caused by inflammatory processes (6). The purpose of this investigation was to evaluate the usefulness of whole brain diffusion tensor imaging indices for noninvasive measurement of neuropathologic changes in cases of HIV-associated cognitive impairment, including the prognostic significance with respect to concurrent measures of dementia severity.
Methods
Participants
Seropositive participants (four male and two female patients; mean age, 47 ± 7.8 years) included well-characterized, medically stable patients participating in a longitudinal investigation of the natural history of neurologic impairment in cases of advanced HIV infection (7). Control participants (six male and two female volunteers; mean age, 39 ± 10 years) were comprised of volunteers without history of neurologic illness. Self-reported seropositivity was confirmed by enzyme-linked immunosorbent assay and Western blot analysis. All control participants reported HIV seronegativity. Study exclusion criteria were chronic neurologic disorders, current or past opportunistic CNS infection, and major psychiatric disorder at study entry. There were no significant demographic differences between the groups. All patients with HIV were receiving anti-retroviral therapy. Dementia severity was determined for all participants on the basis of standardized criteria defined by the American Academy of Neurology (AAN) (8) and ratings based on the Memorial Sloan Kettering (MSK) rating scale (9). Various cognitive domains were assessed, including verbal and visual memory, working memory, constructions, psychomotor skills, frontal systems, reaction time, and literacy. Functional status was measured by using the Karnofsky Performance Scale (10). Clinical assessments of the patients with HIV included the ACTG macro-neurologic examination, the Unified Parkinson’s Disease Rating Scale, and neuropathy evaluation. CD4 counts for the patients with HIV ranged from 10 to 187; plasma viral load ranged from 1.9 to 2.6 (measures in log10). The cohort sample and the derivation of dementia severity scores have been extensively described elsewhere (7).
MR Imaging and Image Processing
Studies were performed on a 1.5-T twin speed MR imaging unit using the zoom gradient. A quadrature birdcage head coil was used for RF transmission and signal intensity reception. Diffusion tensor imaging was performed with an echo-planar sequence and a bandwidth of ±125 kHz and bipolar diffusion gradients (dual spin-echo option) to minimize distortion. Six diffusion-weighted images were acquired of each section, with a b value of 1000 s/mm2. A b = 0 reference image was also acquired. Diffusion was applied along six directions: (1,0,1)/2, (−1,0,1)/2, (0,1,1)/2, (0,1,−1)/2, (1,1,0)/2, (−1,1,0)/2. The entire brain was imaged, from the base of the cerebellum to the top of the skull, by using 22 contiguous 7-mm axial sections with the following parameters: field of view, 24 cm; matrix, 128 × 128; 7000/4 (TR/number of excitations). All imaging parameters were held constant across all participants.
Quantitative image analysis was performed off-line on a Linux workstation by using customized image processing routines written in MatLab (Mathworks, Natick, MA). The eigenvectors and eigenvalues of the diffusion tensor were calculated for each voxel and used to produce maps of the ADC and FA, defined as follows:  where
where  where D1, D2, and D3 are the eigenvalues of the diffusion tensor.
where D1, D2, and D3 are the eigenvalues of the diffusion tensor.
To obtain whole brain statistics for the FA and ADC, the background noise was first segmented out from tissue by applying an automated thresholding technique to the diffusion-weighted images. This also removed voxels containing predominantly CSF, because these have low intensity on diffusion-weighted images. Extracranial structures were excluded from the remaining mask by manual segmentation. FA measures (dimensionless) were expressed as root mean squares to give weighting to tissue with high FA (white matter); whole brain peak ADCs were in units of 10(−3) mm2/s, hereafter referred to as whole brain FA and whole brain ADC.
Statistical Analyses
Primary dependent measures for analyses included the quantitative diffusion tensor imaging measures calculated for whole brain: FA and ADC. Cognitive (AAN, MSK, and Karnofsky) and clinical (CD4 counts, plasma viral load) status measures were also examined. These analyses were executed with SPSS (release 11.5; Chicago, IL) using two-tailed (P = 0.05 significance level) statistical tests.
Results
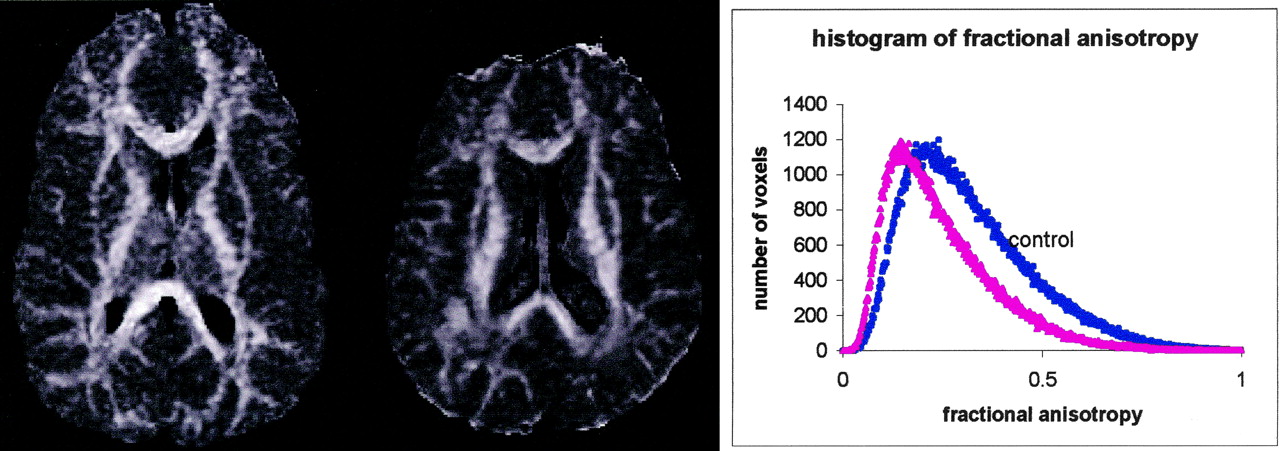
Aggregate whole brain diffusion tensor imaging measures, including FA and ADC, were compared between patients with HIV and control volunteers. Whole brain FA measures were significantly reduced in the patients with HIV (t(12) = −2.1, P = .05; mean (SD) FA: HIV = 0.30 (0.01) versus Control = 0.32 (0.02)). Figure 1 presents whole brain histograms of the FA in an HIV-infected patient and a control volunteer. The peak for the patient is shifted to the left, and the histogram shows a higher percentage of voxels with lower FA values. Means and SDs for the whole brain diffusion tensor imaging indices are presented in Table 1. Further analyses examined relationships between the whole brain diffusion tensor imaging measures and various measures of the severity of dementia based on concurrent neuropsychologic evaluations (n = 14) (Table 2). Whole brain FA was significantly associated with severity of dementia, as indicated by all cognitive status measures considered (AAN: rho = −.63, P = .02; MSK: rho = −.59, P = .03; and Karnofsky: rho = 0.64, P = .01). There were no significant differences between groups regarding whole brain ADC or relationships between whole brain measures of ADC and measures of dementia severity (MSK, AAN, and Karnofsky). Table 3 presents more detailed data regarding the patients with HIV, including diffusion tensor imaging means for specific levels of MSK and AAN dementia severity. Examination of the pattern of findings presented in Table 3 indicates that whereas reduced FA was associated with cognitive decline, ADC measures generally tended to increase with the severity of dementia. Other measures of disease severity in cases of HIV, including CD4 counts, plasma viral load, and duration of illness, were not significantly predictive of cognitive status (P > .05) (Table 4). Routine findings based on visual inspection of the images were consistent with those described in previous MR imaging studies of HIV (3). No localized lesions were found in the patients with HIV. Atrophic changes, however, were evident for some patients.

Map of FA at central section in healthy control volunteer (left) and in HIV-infected patient (right) and whole brain histograms of the FA for the control volunteer (blue) and an HIV-infected patient (red).
Means and SDs for whole brain diffusion tensor imaging measures
Relationships between whole brain diffusion tensor imaging and dementia severity measures
Whole brain fractional anisotropy and apparent diffusion coefficient means by levels of dementia severity in participants with HIV
Relationships between dementia severity and clinical status measures in participants with HIV
Discussion
This investigation indicates reduced whole brain FA among cognitively impaired patients with HIV. Whole brain FA was significantly associated with severity of dementia and functional impairment. Other measures of HIV disease severity examined in this investigation, including CD4 counts and plasma viral load, were not significantly predictive of cognitive status. The findings are consistent with evidence that peripheral markers have limited or inconsistent prognostic usefulness for HIV dementia (11). Although injury may result directly from neurotoxic viral proteins (eg, gp120 and Tat), pathways to neuronal injury in cases of HIV are predominantly indirect (1). Virus likely enters the brain through HIV-infected macrophages or microglia, releasing neurotoxic proteins, cytokines, and chemokines, which further activate uninfected resident macrophages and microglia. Macrophages and microglia induce proinflammatory cytokines (eg, tumor necrosis factor-α) and other mediators of inflammation that lead to neuronal and astrocytic dysfunction. Peripheral measures of disease progression may not reflect the combined or cumulative effects of direct HIV infection and immune activation of uninfected cells in the brain (12). Measures such as CSF viral load may represent approximate or more causally distant indicators of neuronal injury (13–15). Whole brain FA histograms may better represent cumulative extent of injury from heterogeneous neuropathologic processes, including inflammatory (eg, microglia, macrophages, and sparse lymphocytes) to degenerative (eg, myelin loss and axonal damage) changes.
Whole brain FA may reflect aggregate anisotropic changes associated with histopathological findings in cases of HIV, including astrogliosis, myelin pallor, diffuse astrocytosis, perivascular mononuclear inflammation, neuronal loss, and the pathologic hallmark, multinucleated giant cells (16). Diffusion tensor imaging studies of other CNS disorders indicate that anisotropy changes correspond to factors that have also been implicated in HIV dementia, including edema, inflammatory infiltrates, demyelination, and axonal degeneration (17, 18). A diffusion tensor imaging study of advanced HIV indicates region-specific reductions in anisotropy and increased diffusivity (19).
Some findings suggest that diffusion tensor imaging may identify changes in brain tissue status during asymptomatic periods; region-specific anisotropy distinguished patients from control participants in a study of white matter pallor, a prominent neuropathologic feature of HIV (20). Diffusion tensor imaging may have potential for localizing patterns of change within the brain early in the course of infection. Subcortical areas, such as the basal ganglia, are particularly vulnerable to the effects of HIV infection (21, 22) and to excitotoxicity (23). Some evidence suggests a relationship between subcortical vulnerability and cognitive decline (24, 25). Investigations of the cognitive correlates of diffusion tensor imaging parameters could shed light on the selective pattern of deficits observed in HIV-associated cognitive decline, including impairment of psychomotor speed, memory, new learning and motor skills with relative sparing of language, judgment, specific perceptual processes, and capacity for abstraction (26). Further studies are necessary to determine whether diffusion tensor imaging measures can be used to identify subclinical changes in asymptomatic patients with HIV and to determine whether these measures have potential use as markers of progression from asymptomatic HIV to early stages of minor cognitive motor deficits and to HIV dementia.
Mechanisms underlying HIV dementia are not clearly understood. Available evidence suggests a complex model involving CNS viral entry, immune dysregulation, and blood-brain barrier dysfunction (1). The relative prognostic significance and/or synergistic effects of macrophage activation and cytokine release, astrocytic infection, neuronal loss, and axonal damage to sequelae of advanced HIV infection have not yet been determined (27). Conventional imaging provides limited information concerning tissue damage, cellular components, and inflammation (28). Factors such as gliosis, leakage of serum proteins, circulating cytokines, reactive astrocytes, and fluctuations of tissue water may mask or bias measurement of sublethal tissue change and cumulative extent of injury in conventional imaging studies (3, 27–30). The findings from this study are consistent with other lines of evidence supporting the use of quantitative MR imaging strategies for measuring diffuse neuropathophysiological processes in cases of HIV (31–33). Imaging modalities such as MR spectroscopy have also been used to derive putative measures of neuronal loss (eg, N-acetylaspartate), astrocytosis, or microglial activation (increased choline in white matter regions) and glial markers of inflammation (eg, increased myoinisotol) in cases of HIV (34, 35). MR spectroscopy studies indicate abnormalities in frontal white matter and in basal ganglia that may respond to highly active anti-retroviral therapy (36–39).
Measurement of diffusion provides another noninvasive imaging strategy for exploring cellular integrity and pathology (5). Diffusion tensor imaging indices may have considerable promise for measuring changes corresponding to pathologic processes that have been implicated in association with HIV but cannot be observed directly, including sublethal injury to tissue. Anisotropy and average diffusivity are influenced by factors such as fiber diameter and degree of myelination within voxels, and macrostructural factors such as intravoxel fiber-tract coherence and organization (4). Diffusion tensor imaging parameters can be used to quantify changes such as loss of integrity in directionally ordered tissues (eg, white matter fiber tracts) and expansion of extracellular space (17, 40). Inflammatory responses may create local hypercellular environments with more restriction to diffusion. Expansion of the extracellular space caused by various pathologic processes may also be reflected in diffusivity changes (19). Diffusion parameters may measure changes in degenerating tissue and alterations due to blood-brain barrier disruption or CNS immune activation (4, 40). Accumulating evidence supports the validity of quantitative MR imaging strategies for studying CNS disorders involving inflammation, blood-brain barrier impairment, and neurodegeneration (17, 41).
This study indicates reduced whole brain FA in cases of HIV-associated cognitive impairment. FA may be more sensitive than ADC for whole brain imaging of patients with HIV. HIV neuropathology involves extensive white matter abnormalities that may be reflected in net loss of directional water molecular motion. Whole brain ADC was not significantly associated with measures of clinical and cognitive status. However, examination of relationships between ADC and dementia status measures indicated a consistent reversal of the pattern observed for FA; increased ADC tended to be associated with severity of cognitive impairment. The respective diffusion tensor imaging measures may be differentially sensitive to specific pathophysiological processes or to changes in white versus gray matter. Increased ADC may suggest net loss of structural barriers to diffusion (42). Increased diffusivity may reflect factors associated with increased extracellular space, such as degenerative processes. Aggregate ADC measures may be more influenced by pathology or time-dependent nonlinearities than aggregate FA measures. Although whole brain ADC measures were not associated with clinical status, ADC measures may be useful for longitudinal HIV studies of specific brain regions. Studies of multiple sclerosis indicate increased ADC in lesions and in pre-lesional or normal appearing white matter, possibly reflecting demyelinating processes (43, 44). MR imaging studies of cases of stroke, however, indicate initial decreases in ADC in localized damage, possibly because of cytotoxic edema, energy failure, or swelling of cells consequent to water influx from the extracellular compartment (45–47). When examined across time, ADC measures in stroke may reverse, normalize, or change further in response to late secondary injury (48). Physiological mechanisms underlying these findings are not well understood but, taken together, suggest the potential of ADC measures for differentiating and quantifying the temporal course of neuropathologic processes in longitudinal region-specific investigations of HIV-associated cognitive impairment. Some HIV sequelae may correspond to decreases in ADC (eg, edema), whereas other sequelae may correspond to increased diffusivity (eg, neurodegeneration).
HIV dementia is a major cause of morbidity and a significant risk factor for death in persons with AIDS (13, 49). The brain may be subject to ongoing changes during the course of HIV infection (50–53). The difficulty in quantifying advancing infection in brain has compromised efforts to delineate mechanisms of HIV neuropathogenesis and to identify neuroprotective agents (54). Findings from this investigation support the use of diffusion tensor imaging for measuring diffuse brain changes in cases of HIV-associated cognitive impairment. Further studies are necessary to determine whether diffusion tensor imaging measures are sensitive to subclinical changes in asymptomatic patients with HIV. Diffusion tensor imaging measures may have potential clinical use for identifying individuals at risk for progression and for monitoring clinical status. Longitudinal studies of region-specific diffusion tensor imaging parameters (eg, in caudate nucleus, putamen, and deep white matter) may provide insights concerning early viral entry into brain, the relative resistance or sensitivity of specific brain regions to HIV-associated injury, and factors associated with sudden change in status. Sequelae such as early cognitive decline in persons with HIV may persist, improve with anti-retroviral therapy, or progress to frank dementia. Noninvasive markers of status may be useful for evaluation of treatment failure, for informing efforts to modify therapy, and for determining whether specific cognitive deficits are associated with changes in tissue or are more influenced by other factors (eg, depression). Diffusion tensor imaging indices may have potential clinical use for assessing therapeutic response to anti-retroviral therapy within CNS and for distinguishing reversible and irreversible HIV-induced injury. Region-specific increases in FA or changes in ADC may reflect treatment response; more pronounced or persistent diffusion tensor imaging abnormalities may be consistent with worsening or irreversible changes to tissue.
Conclusion
This investigation evaluated the prognostic significance of whole brain histogram-derived diffusion tensor imaging indices with respect to severity of cognitive impairment and other measures of clinical status in cases of HIV. Whole brain FA was reduced in patients with HIV and correlated with severity of dementia, as indicated by a series of widely used clinical and functional status measures. Further studies are necessary to determine whether diffusion tensor imaging measures represent potential prognostic or vulnerability markers for measuring early HIV-induced neuropathologic changes.
Acknowledgments
We are grateful for the assistance of Linda Pierchala, Linda Reisberg, Prasad Pottumarthi, and Qun Chen.
Footnotes
This work was supported by National Institutes of Health grant K23 MH66705 (to A.R.) and National Institutes of Health/National Institute of Neurological Disorders and Stroke grant NS36519 (to L.E.).
Some findings from this investigation were presented at the 2003 meeting of the International Society of Magnetic Resonance in Medicine, Toronto, and the 2003 meeting of the Organization for Human Brain Mapping, New York.
References
- Received April 3, 2002.
- Accepted after revision June 18, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Longitudinal white matter alterations in SIVmac239 infected rhesus monkeys with and without regular cART treatment
- Neuroimaging of Rapidly Progressive Dementias, Part 2: Prion, Inflammatory, Neoplastic, and Other Etiologies
- Biomarkers of HIV-1 CNS infection and injury
- Disease burden in HIV-associated cognitive impairment: A study of whole-brain imaging measures