
Abstract
BACKGROUND AND PURPOSE: Intracranial hemorrhage in term neonates often results from asphyxia, obvious birth trauma, blood dyscrasia, or vascular malformation but may occur without an obvious inciting event. In this study, we review the clinical and neuroimaging features of healthy term neonates presenting with spontaneous superficial parenchymal and leptomeningeal (ie, subpial or subarachnoid) hemorrhage.
METHODS: The clinical records and neuroimaging studies of seven term neonates with spontaneous superficial parenchymal and leptomeningeal hemorrhage were retrospectively reviewed. All underwent diffusion-weighted MR imaging and 6 underwent CT within 72 hours of birth. Magnetic susceptibility-weighted imaging was performed in five, MR angiography in two, and MR venography in two. Follow-up MR imaging was performed in one infant. Clinical follow-up was done in four patients.
RESULTS: All neonates had normal birth weights and high 5-minute APGAR scores. All were delivered vaginally (one with forceps assistance, and one with vacuum assistance). No blood dyscrasias were noted. Within 36 hours after delivery, all neonates presented with apnea or seizures or both. Neuroimaging subsequently revealed superficial parenchymal and leptomeningeal hemorrhage. Four occurred in the anterior-inferior-lateral temporal lobe adjacent to the pterion. The remaining three were located in the parietal lobe, frontal lobe, and lateral temporal lobe under the squamosal suture. Decreased diffusion in parenchyma adjacent to the hemorrhage and overlying subcutaneous soft-tissue swelling were apparent in five patients. Susceptibility-weighted imaging showed no additional lesions. MR angiography and MR venography findings were normal. Follow-up MR imaging in one patient demonstrated encephalomalacia. Four patients with short-term clinical follow-up were neurologically normal.
CONCLUSION: Spontaneous superficial parenchymal and leptomeningeal hemorrhage occurs in otherwise healthy term neonates. The hemorrhage is most often in the temporal lobe and in proximity to sutures, accompanied by overlying soft-tissue swelling and adjacent decreased diffusion. This pattern leads us to implicate local trauma with contusion or venous compression or occlusion in the development of these hemorrhages.
Intracranial hemorrhage in term neonates is most often subdural or subarachnoid in location. Intraparenchymal hemorrhage occurs infrequently in full-term neonates. Most parenchymal bleeding in the term infant involves the thalamus, is associated with intraventricular hemorrhage, and develops in infants at risk for venous thrombosis (1). Hemorrhage elsewhere in the brain is usually due to obvious birth trauma, asphyxia, underlying blood dyscrasia, or congenital vascular malformation (2). However, the literature contains scattered descriptions of intracranial hemorrhage occurring spontaneously in previously healthy neonates (3–6). In this study, we review the clinical presentation, neuroimaging features, and short-term outcome of a group of term infants presenting with apparently spontaneous superficial parenchymal and leptomeningeal (ie, subpial or subarachnoid) hemorrhage. We also describe unique diffusion imaging abnormalities that accompany these hemorrhages and postulate a mechanism for their occurrence.
Methods
After obtaining approval from our institutional review board, we reviewed the clinical records and neuroimaging studies of seven term neonates (38 to 41 weeks postconceptional age) (Table 1) presenting with superficial parenchymal and leptomeningeal hemorrhage. Prenatal, postnatal, and obstetric histories, age, sex, and relevant laboratory results were recorded. Neurologic follow-up ranging from 1 to 13 months (average, 4 months) was available for four patients.
Clinical history of term neonates with lobar hemorrhage
CT Protocol
Six patients underwent cranial CT within the first 48 hr of life. Using a GE CTi Highspeed (GE Medical Systems, Milwaukee, WI) scanner, contiguous sequential axial CT sections were obtained from the skull base to the vertex with 5-mm collimation (KV = 120, mAs = 340) and gantry parallel to the glabella-meatal line.
MR Imaging Protocol
All seven patients underwent cranial MR imaging, with diffusion imaging being performed within the first 72 hr of life. One patient underwent follow-up MR imaging of the brain at 16 months of age. Using a quadrature head coil and a 1.5-T MR imaging unit (Signa LX or 5X, General Electric Medical Systems, Milwaukee, WI), sagittal and axial view T1-weighted conventional spin-echo sequences (600/20/2 [TR/TR/number of excitations]; field of view, 20 cm; section thickness, 4 mm; section gap, 1 mm; acquisition matrix, 256 × 192) and fast spin-echo axial view T2-weighted images (3200/85/1; field of view, 20 cm; section thickness, 4 mm; section gap, 1 mm; acquisition matrix, 256 × 192; echo train length, 8) were obtained. Magnetic susceptibility-weighted gradient-echo images (5000/40/1; field of view, 20 cm; section thickness, 4 mm; section gap, 1 mm; acquisition matrix, 256 × 256; flip angle, 20 degrees) were obtained of five patients. Three-dimensional time-of-flight MR angiography (47/2.6/1; field of view, 20 cm; partition thickness, 1 mm; volume thickness, 60 mm) was performed for two patients. 2D phase contrast MR venography (38/12.6/1; field of view, 20 cm; section thickness, 3 mm; velocity encoding, 10 cm/s) was performed for two patients.
Diffusion imaging was performed by using line scan diffusion imaging acquisition in the axial plane with 2014/103/1 (effective TR/TE/number of excitations); field of view, 20 × 10 cm; section thickness, 4 mm; intersection gap, 3 mm; columns, 128 × 96; and b = 5 and 750 s/mm2 (with the maximum b value applied in six directions). Isotropic diffusion-weighted images and apparent diffusion coefficient (ADC) maps extrapolated to a b value of 1000 s/mm2 were generated on a pixel-by-pixel basis according to the Stejskal and Tanner equation, S = S0e−bADC (where b = maximum and S0 is the signal intensity for b = 5 s/mm2) (7).
Results
Clinical History
The prenatal history was unremarkable for five patients (Table 1). Maternal hypertension was present in one case, and maternal thalassemia minor in another.
Five neonates were born via spontaneous vaginal delivery (Table 1). Delivery was assisted with low forceps and vacuum extraction in one patient each. Apgar scores at 1 min ranged from 2 to 9 (average Apgar score, 6), and Apgar scores at 5 min were ≥7 for all infants.
Six infants had no neurologic symptoms for at least several hours after birth. However, all patients eventually presented with apnea (five patients) and/or seizures (four patients) within 36 hr.
Platelet counts were normal in all patients. Prothrombin and partial thromboplastin times, available for five patients, were normal. Hematocrit ranged from 48% to 56%.
Imaging Findings
Variable amounts of superficial parenchymal and leptomeningeal hemorrhage occurred in the anterior inferior temporal lobe under the pterion in four patients (Figs 1 and 2), in the lateral temporal lobe under the squamosal suture in one patient (Fig 3), in the left frontal lobe under the coronal suture in one patient (Fig 4), and in the right parietal lobe in one patient (Fig 5) (Table 2). The parenchymal hemorrhage was contiguous with extraparenchymal leptomeningeal bleeding, either subpial or subarachnoid, in all patients. Extracranial soft-tissue swelling was noted overlying the site of hemorrhage in five neonates. In four patients, the soft-tissue swelling consisted of mild edema in the subcutaneous fat (Figs 1 and 2), whereas in one patient, there was a cephalohematoma (Fig 5) (patient 6, Table 2).

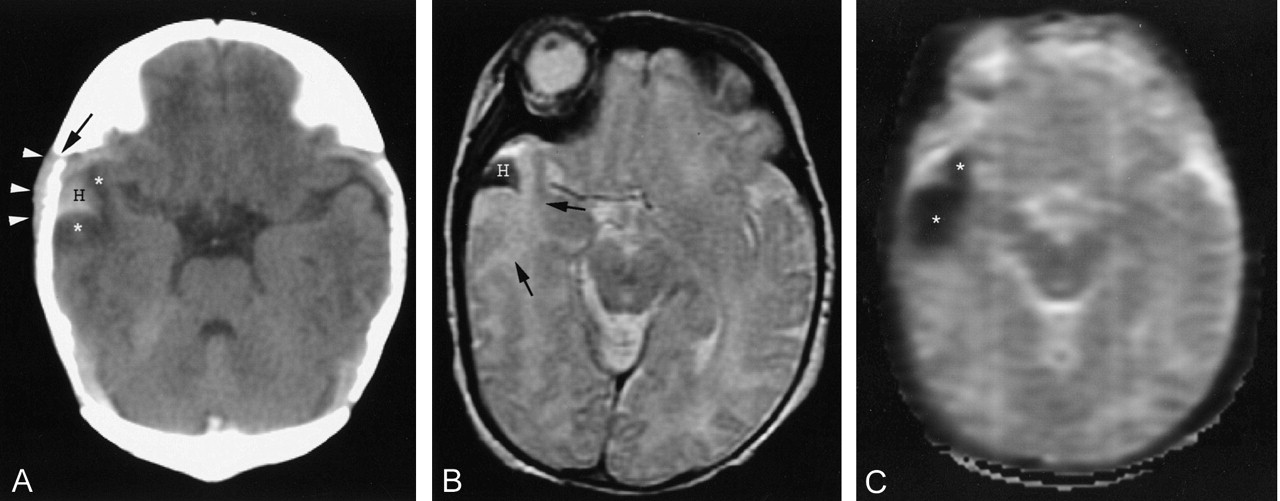
Images of a neonate (patient 4) with perinatal depression and episodes of apnea beginning immediately after birth.
A, Axial view unenhanced CT scan of the head shows parenchymal hemorrhage (H) extending to the brain surface and asymmetric soft-tissue swelling (arrowheads). A minor amount of edema is present next to the hemorrhage (*). Note proximity to the pterion (arrow).
B, Axial view T2-weighted MR image (3200/85/1; echo train length, 8) shows a low intensity hemorrhage (H) with adjacent edema (arrows).
C, ADC map (2014/103/1; b max, 750 s/mm2) shows decreased diffusion in area of edema next to the hemorrhage (*).

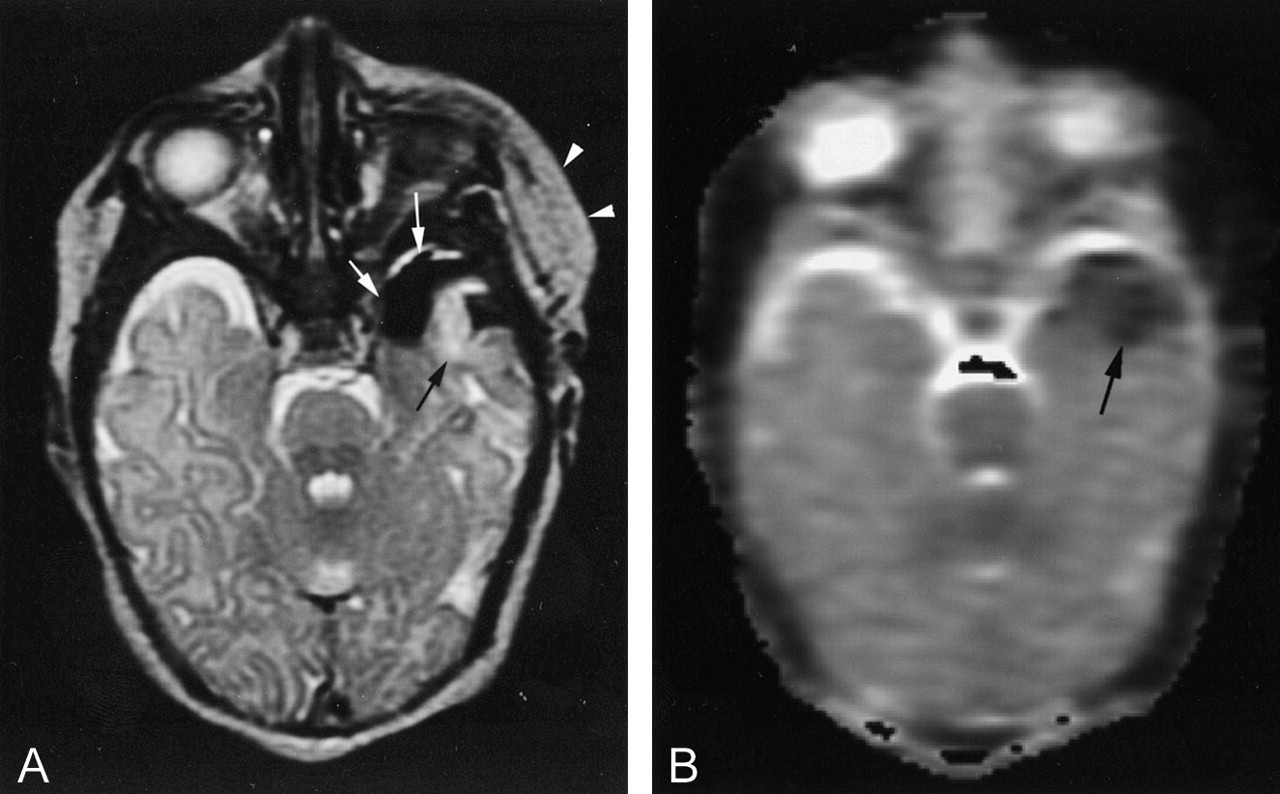
Images of a neonate (patient 3) with apnea and seizures at 24 hr of life.
A, Axial view T2-weighted MR image (3200/85/1; echo train length, 8), obtained above the level of parenchymal hemorrhage, shows soft-tissue swelling (arrowheads), subpial extension of hemorrhage (white arrows), and parenchymal edema (black arrow).
B, ADC map indicates decreased diffusion in the edematous area (arrow).

Images of a neonate (patient 5) with apnea at 8 hr of life.
A, Axial view unenhanced CT scan of the head shows leptomeningeal hemorrhage (H) under an expanded squamosal suture (arrowheads). Adjacent low attenuation edema is present (arrows).
B, Axial view T2-weighted MR image (3200/85/1; echo train length, 8) shows low intensity hemorrhage (H) and high intensity adjacent edema (arrows).
C, Decreased diffusion (arrows) is indicated on the ADC map (2014/103/1; b max, 750 s/mm2).
D, Axial view T2-weighted MR image (3200/85/1; echo train length, 8), obtained at 16 months of age, shows encephalomalacia (arrows). No underlying vascular abnormality is apparent.

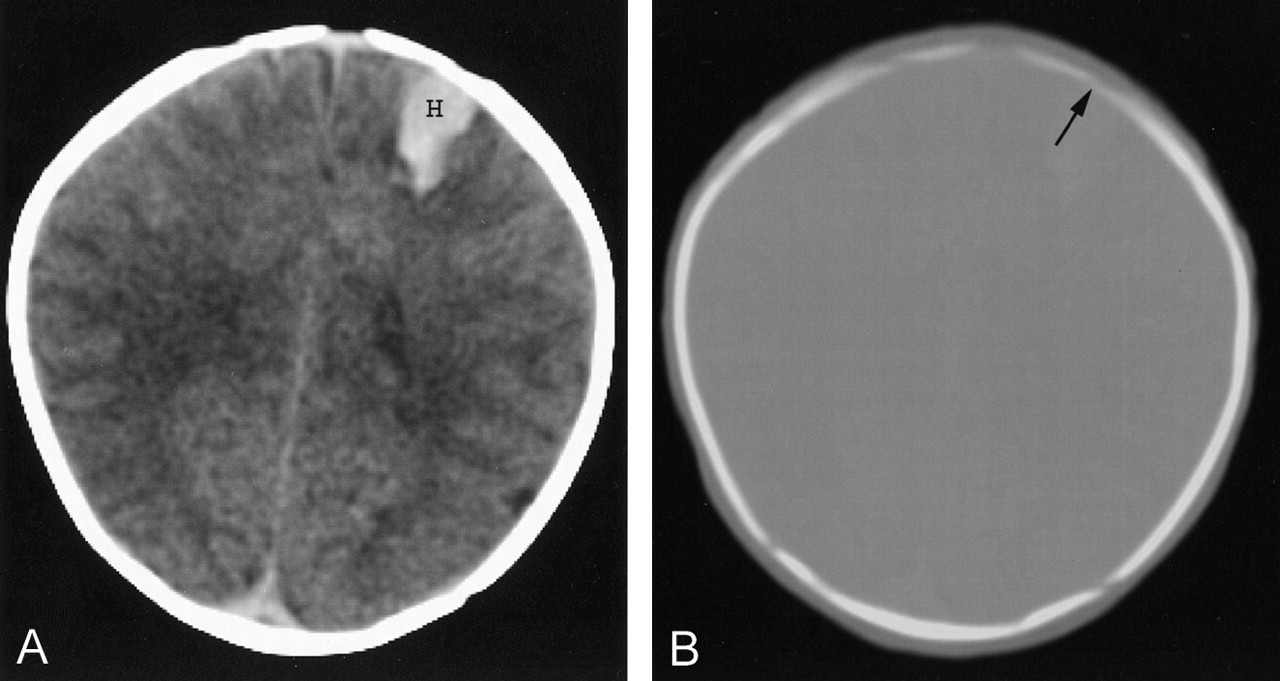
Unenhanced CT scan of a neonate (patient 7) with seizures at 36 hr of life.
A, Brain window shows a parenchymal hemorrhage (H) extending to the brain surface in close proximity to the coronal suture (arrow). Leptomeningeal hemorrhage was evident at other levels (not shown).
B, Bone window also shows a parenchymal hemorrhage (H) extending to the brain surface in close proximity to the coronal suture (arrow).

Unenhanced CT scans of a neonate (patient 6) with focal seizures at 18 hr of life.
A, CT scan shows a right parietal parenchymal hematoma (H).
B, CT scan obtained at a slightly higher anatomic section reveals additional hemorrhage (H) with extension into the sulci, indicating leptomeningeal bleeding (arrows). A large overlying cephalohematoma (arrowheads) is also present.
Imaging features of lobar hemorrhage in term neonates
CT revealed hyperattenuated superficial parenchymal and leptomeningeal hemorrhage with variable adjacent edema in all patients. No calvarial fractures were evident. On MR images, the hemorrhage exhibited T1 and T2 shortening in six patients and T1 prolongation/T2 shortening in one patient. Regions of T2 prolongation in parenchyma adjacent to the hemorrhage had abnormally decreased ADC values in five patients (Figs 1–3). A small subdural hematoma was present in one patient. MR angiography of two patients revealed no middle cerebral artery occlusion. Additionally, spin-echo images showed no asymmetry of arterial flow voids to suggest arterial occlusion in any patient. The results of MR venography of two patients were normal. No thrombosed cortical veins were seen on spin-echo images. No underlying vascular abnormality or mass lesion was evident on any images. Magnetic susceptibility-weighted imaging of the five patients for whom it was performed did not show any additional sites of hemorrhage. Sixteen-month follow-up MR imaging of one patient showed only encephalomalacia in the anterior temporal lobe (Fig 3D).
Clinical Follow-up
Data from clinical follow-up that ranged from 4 weeks to 13 months (mean, 4.3 months) were available for four patients. These four infants were neurologically normal, with no further seizures or apnea occurring beyond the perinatal period.
Discussion
Neonatal intracranial hemorrhage is usually subarachnoid, subdural, or intraventricular in location (3). Intraparenchymal hemorrhage in the term infant is relatively uncommon (1, 3–5, 8). Our study focuses on a particularly rare subset of full-term intracranial hemorrhage: spontaneous superficial parenchymal and leptomeningeal (ie, subpial or subarachnoid) hemorrhage.
Both intraventricular and intraparenchymal hemorrhage in term neonates have been described previously (1, 3–5, 8). The cause of intraventricular hemorrhage in term neonates is often unknown but is more frequently seen in neonates with a predisposition to cerebral venous infarction, such as sepsis, cyanotic congenital heart disease, and coagulopathy (1, 4). Internal cerebral vein thrombosis has been postulated as an explanation for the observation of a high incidence of thalamic hemorrhage as a cause of intraventricular hemorrhage (1).
Scattered case reports have attributed intraparenchymal hemorrhage in full-term neonates to birth trauma, asphyxia, underlying blood dyscrasia, or congenital malformation (2). More baffling are multiple descriptions in the literature of intraparenchymal hemorrhage occurring spontaneously in previously healthy neonates (3–6, 8). Those patients, like the patients with superficial parenchymal and leptomeningeal bleeding comprising our study, are of normal birth weight, have no prenatal complications, possess high Apgar scores, and undergo deliveries that are characterized by hospital records as atraumatic and uncomplicated (4). Most neonates presenting with isolated intraparenchymal hemorrhages are healthy, and no specific cause for the bleeding is ever identified (3–5, 8).
Potential explanations for the spontaneous parenchymal hemorrhages presented in the literature and for the spontaneous superficial parenchymal and leptomeningeal hemorrhages we observed include arterial occlusion with hemorrhagic infarction and hemorrhagic venous infarction or unsuspected cortical contusion related to parturitional trauma (3–5, 8). We think local trauma with resultant venous or capillary-venous injury is the most likely cause of the bleeding that occurred in our patients.
In 1985, Bergman et al (4) described three cases of intraparenchymal hemorrhage occurring in previously healthy term neonates (0–3 days old) and hypothesized hemorrhagic conversion of embolic arterial infarction as the cause. In their view, emboli in the neonate could arise spontaneously from thrombosis of the umbilical arteries, from thrombosis of the ductus arteriosus, or as emboli of infarcted placental fragments. This hypothesis of hemorrhagic arterial infarction was based on the observation that the location of the lesions as shown on CT scans was consistent with branch occlusions of the middle cerebral or posterior cerebral arteries. Confirmatory vascular imaging was not performed for their patients.
Difficulties exist in ascribing the superficial parenchymal and leptomeningeal hemorrhages and associated imaging features we observed to embolic arterial occlusion. Hemorrhagic conversion of ischemic infarctions is most likely to occur with large arterial infarctions in older adults (9, 10). Although signal intensity changes suggesting small petechial hemorrhages or mineralization may occasionally occur with arterial infarctions in the neonate, hemorrhage is not usually the dominant feature of the lesion, as was seen in our patients (11, 12). By contrast, the lesions we identified consisted most often of small regions of cortical swelling adjacent to larger areas of hemorrhage. Additionally, MR imaging did not show any secondary signs of arterial occlusion (eg, vascular flow void asymmetry) in our patients, and MR angiography of the two patients for whom it was performed showed patency of the major branch vessels of the circle of Willis. Last, the frequent association of overlying soft-tissue swelling we observed cannot be accounted for by intracranial arterial infarction. Although these features do not entirely preclude hemorrhage into a small arterial branch territory infarction, the possibility of such a cause seems remote.
Cortical contusion and hemorrhagic infarction due to venous thrombosis, compression, or laceration are common causes of parenchymal brain hemorrhage in both children and adults and are potential causes of the hemorrhages we observed. Although certain factors predisposing to the development of venous thrombosis, such as significant dehydration, polycythemia, sepsis, congenital heart disease, and hemoglobinopathy, were lacking in our patients, minor parturitional trauma alone may have been sufficient for the development of hemorrhagic venous or capillary-venous related injury.
Considering the relative compliance of the neonatal calvaria and widely open sutures in the neonate, it is easy to imagine that one cranial bone could slip under an adjacent cranial bone during head molding in delivery and thereby press on the brain parenchyma. Contusion or venous hemorrhage could then result, either secondary to shearing forces created by bone edges tearing the dura mater and damaging bridging veins or from impact on delicate intraparenchymal capillaries or veins (8). The finding of scalp swelling overlying the cortical injury in five of seven patients further supports a theory of local mechanical trauma. Moreover, a crescent of decreased diffusion around a hematoma, similar to what we observed in our neonates, has been reported to be observed during the subacute phase of contusion in adults (13). Although none of the neonates in our study exhibited imaging signs of dural venous thrombosis, isolated cortical venous thrombosis or parenchymal capillary-venous injury are possible explanations for the hemorrhages. Direct evidence of small vessel injury is difficult to detect, but the finding of decreased diffusion, consistent with cytotoxic edema, in the tissue adjacent to the hemorrhage is supportive of ischemic necrosis (13–18).
Four of the hemorrhages we documented were located in the anterior-inferior-lateral temporal lobe adjacent to the pterion, which is a large, relatively unprotected sutural confluence in the neonate and, therefore, an ideal location for vascular injury due to changing positions of cranial bones during delivery. The immature configuration of the venous system in the infant may also render the anterior temporal lobe especially vulnerable to hemorrhage. Even in the term infant, the dural venous and pial venous systems have not yet reached an adult configuration (19). Importantly, the precursor to the sphenoparietal sinus, which collects the superficial middle cerebral veins, has not yet developed a connection medially with the cavernous sinus but instead drains into the tentorial sinus, which courses along the floor of the middle cranial fossa to the transverse sinus (19). The position of the tentorial sinus is variable. It is possible that a lateral position, near the pterion would render this sinus vulnerable to local compression or thrombosis, resulting in increased parenchymal venous pressure and hemorrhage. Also of potential significance is the diploic segment (temporal diploic vein) of the anteroparietal meningeal sinus, the embryologic precursor to the sinus of Breschet, which accompanies the anterior division of the middle meningeal artery and ultimately drains into the sphenoparietal sinus (19). The temporal diploic vein is likely to be especially prone to compression or injury during parturition because of its proximity to open sutures and the plasticity of the calvaria at birth.
Of the remaining three hemorrhages we observed, two were located adjacent to open sutures and, therefore, like the hemorrhages in the anterior temporal lobe, in relatively unprotected locations potentially susceptible to direct mechanical injury. The third hemorrhage, located in the parietal lobe, was immediately beneath a large cephalohematoma, also suggesting the possibility of local trauma.
The concept of mechanical injury to the brain parenchyma as a cause for neonatal superficial parenchymal hemorrhage has been previously noted by Hayashi et al (8). That particular report, however, was limited to only two cases in which the hemorrhage occurred in the left frontal lobe under the coronal suture. Additionally, the observation of subtle, localized subcutaneous soft-tissue swelling, which corroborates the theory of local trauma, was not made. Also, although Hayashi et al documented superficial parenchymal hemorrhage in their patients, associated leptomeningeal hemorrhage was not reported and, in contrast, our series suggested that the temporal lobe may be the most common location for such a hemorrhage. The report presented by Hayashi et al antedated the use of diffusion imaging, which also supports a diagnosis of contusion or traumatic venous infarction in our patients.
The superficial cortical swelling and location of parenchymal bleeding that we observed not only supports a traumatic theory of origin for these lesions but also suggests that the leptomeningeal bleeding may be subpial in location. Intracranial hemorrhage is usually classified as parenchymal, subarachnoid, subdural, intradural, or epidural in location. Leptomeningeal hemorrhage most often results in bleeding into the subarachnoid space but, in theory, may also occur deep to the pia in the subpial space. However, the occurrence of subpial hemorrhage is controversial because electron micrographs have indicated that no true subpial space exists in normal brain (20). The subpial space normally consists of only small intercellular clefts located between astrocytic processes and equally narrow clefts between the glial footplates and the basement membrane coating the brain (20). However, pathologically proved subpial hemorrhage has been documented in neonates (20). In 1972, Friede (20) reported histopathologic findings in nine cases of subpial hemorrhage in neonates and young infants. In that report, subpial bleeding occurred predominantly in preterm infants; however, one infant, similar to the infants in our study, was a term neonate who was clinically well immediately after birth but developed cyanosis at 7 hr of age. Friede found that the subpial hemorrhage originated in the parenchyma and extended into the superficial glial layer, disrupting the astrocytic footplates that bind the pia to the brain. Friede postulated that the development of cleavage at this level is facilitated if the superficial glial tissue is swollen. Hemorrhage is thought to develop as a result of stretching and consequent rupture of the capillary-venular network in the outer layers of edematous cortex (20). The finding of edema with restricted diffusion in brain tissue adjacent to the superficial parenchymal and leptomeningeal hemorrhage in our patients would be consistent with the histopathologic findings of outer layer glial swelling and vacuolization in subpial hemorrhages reported by Friede. Moreover, according to Friede, the pia is more easily separated from the immature than the mature brain. The fragility of the pia-brain adhesion in the neonate may well make it particularly susceptible to injury and the development of subpial hemorrhage. Although pathologic proof is lacking for our patients, the combination of parenchymal hemorrhage with direct extension beyond the confines of the brain suggests that the extraparenchymal bleeding we observed is more likely subpial than subarachnoid in location.
Although clinical follow-up was not the emphasis of our study, we observed that the four patients with short-term clinical follow-up were all neurologically normal without seizures or apnea after the perinatal period. These findings are corroborated by Hanigan et al (5, 6) and Bergman et al (4), who observed normal outcomes during follow-up periods extending up to 6 years in the neonates who matched our patients’ demographic background (term neonates, presenting with hemorrhage at 0–3 days of age, no prenatal complications, high Apgar scores, and supposedly “atraumatic” and “uncomplicated” deliveries). Further studies are needed to follow even longer term outcomes in larger patient populations to confirm whether expectant medical management should be a standard of care. Because there are many presentations of neonatal intracranial hemorrhage, with reportedly different outcomes, some requiring surgical management (4), proper identification of the subset of patients with superficial capillary-venous related hemorrhage would be important for both prognosis and future treatment.
Conclusion
Spontaneous superficial parenchymal and leptomeningeal hemorrhage occurs in otherwise healthy term neonates. In our study of seven affected neonates, these hemorrhages presented most commonly within the temporal lobe, in frequent proximity to open sutures, with overlying soft-tissue swelling, and with adjacent abnormally decreased parenchymal diffusion. This constellation of findings leads us to implicate unsuspected local trauma with contusion or venous compression/occlusion as explanations for this unusual entity.
References
- Received March 27, 2003.
- Accepted after revision August 26, 2003.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging Patterns of Neonatal Subpial Hemorrhage: Provisional Statements on Neurologic Outcomes
- Intracranial Hemorrhage in Term and Late-Preterm Neonates: An Institutional Perspective
- An In-Depth Analysis of Brain and Spine Neuroimaging in Children with Abusive Head Trauma: Beyond the Classic Imaging Findings
- Apnea Spells in a Term Neonate
- Idiopathic Neonatal Subpial Hemorrhage with Underlying Cerebral Infarct: Imaging Features and Clinical Outcome
- Superficial Echogenic Lesions Detected on Neonatal Cranial Sonography: Possible Indicators of Severe Birth Injury
- Retrospective Analysis of Delayed Intraparenchymal Hemorrhage after Flow-Diverter Treatment: Presentation of a Retrospective Multicenter Trial
- Neonatal Seizures
- Early versus late MRI in asphyxiated newborns treated with hypothermia
- Isolated cerebral cortical tears in children: aetiology, characterisation and differentiation from non-accidental head injury
- Neonatal Intracranial Hemorrhage May Be More Frequent than Previously Suspected