
Abstract
Summary: The unusual case of a mandibular arteriovenous malformation in a patient with severe hemophilia A and hepatitis C is reported. Supplementary substitution of various coagulation factors allowed direct puncture and intralesional injection of a liquid adhesive, resulting in complete anatomic and clinical cure without peri- or postoperative bleeding. Replacement therapy providing normal levels of relevant coagulation factors enables endovascular treatment in a safe and effective manner in hemophiliac patients.
Because patients with arteriovenous malformations (AVMs) of the mandible may present with a major hemorrhage (1–3), endovascular treatment often has to be performed as an emergency measure. Hemophilia A, transmitted as an X-linked recessive trait, is the most common heritable bleeding disorder and is caused by various mutations in the gene that codes for factor VIII (FVIII) (4). A patient with a coagulopathy and a high-flow arteriovenous (AV) shunt in this area carries a significantly elevated risk of life-threatening bleeding.
Case Report
A 39-year-old man presented with a round, pulsating, and exophytic distension in the left mandible (20 × 20 × 15 mm), radiating into the external soft tissues of the lower left chin.
He was referred to our hospital for dental surgery and was known to have severe hemophilia A and chronic hepatitis C, corroborated by the laboratory data showing low intrinsic and extrinsic coagulation factor level (FVIII, 0.89; Quick, 58%; apt, 62.0 s).
The patient’s history showed that the distension had become noticeable in 1991 as a “pimple-like” bump. Steady growth and increasing pulsation were observed over the following years and since 1994 seemed to have stopped. Panoramic examination and a CT scan performed at that time revealed an osteolytic lesion in left lower jaw with multiple radiolucencies, following the inferior alveolar canal and resembling a tortuous dilated vessel. MR angiography in 1995 revealed a high-flow vascular lesion—presumably an AVM—of the mandible. Because of feared major hemorrhagic complications, no further invasive diagnostic or therapeutic intervention had been undertaken.
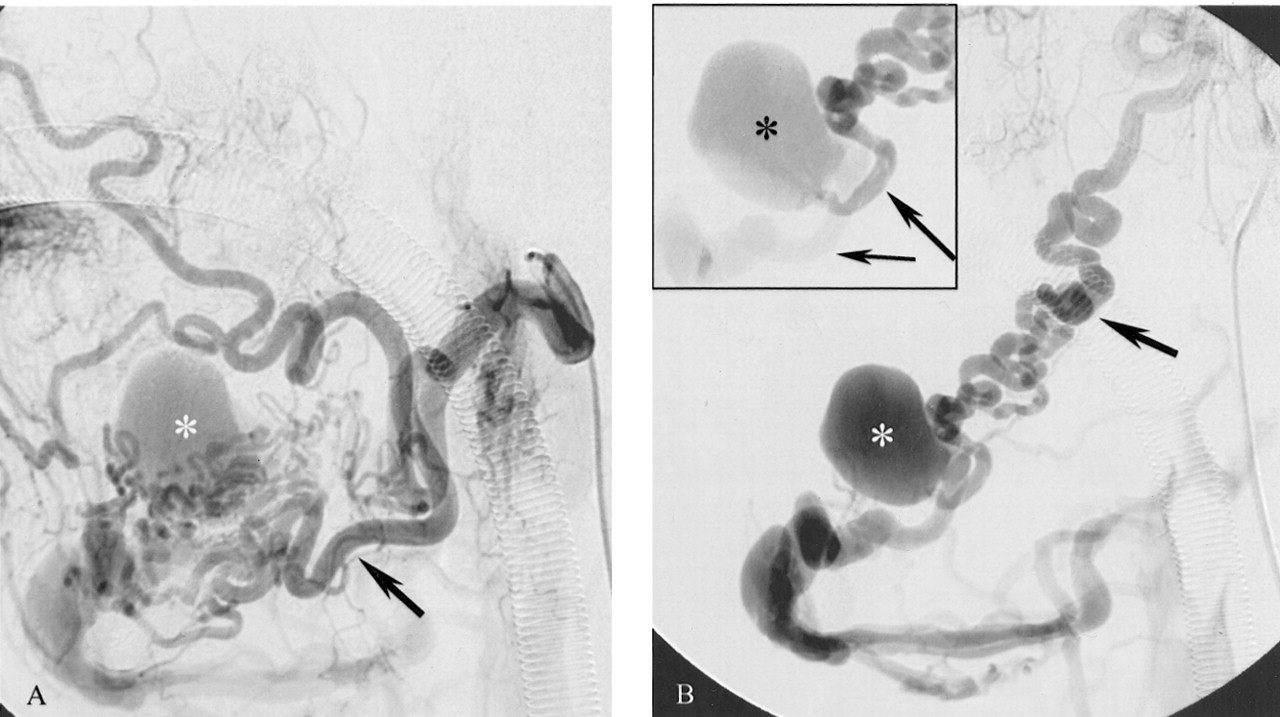
On admission in September 2002, the patient’s dental situation had seriously deteriorated as a result of untreated caries, presenting as residual roots and apical osteitis. For the past 2 years, the patient had stopped using the left side of his mouth for chewing. A control CT scan demonstrated a round, attenuated, soft tissue structure that had broken through the medial and lateral cortex layers in the premolar/molar areas. A selective intra-arterial angiogram confirmed the high-flow AVM of the left mandible with a large venous pouch (Fig 1A and B).

Initial arteriogram.
A, Left facial arteriogram. Lateral view shows opacification of an AV-shunt lesion with early filling of a giant venous varix (asterisk), supplied by numerous small pedicles from the facial artery (large arrow).
B, Left internal maxillary arteriogram. Lateral view reveals the fistulous AV shunt between a tortuous inferior dental artery (large arrow), revealing the intraosseous location, and the aneurysmal pouch (asterisk) of the mandibular vein (small arrow).
Description of the Technique
To ensure effective hemostasis for intra-arterial catheterization, embolization, and surgery, FVIII concentrate (Octanate, Octapharma GmbH, Langenfeld, Germany) was administered as bolus injections. Fresh-frozen plasma (FFP; 1 unit; DRK-Blutspendedienst Sachsen GmbH, Dresden, Germany) and prothrombin complex concentrate (PPSB; DRK-Blutspendedienst Sachsen GmbH) were also administered to raise the patient’s intrinsic and extrinsic coagulation factors to normal levels.
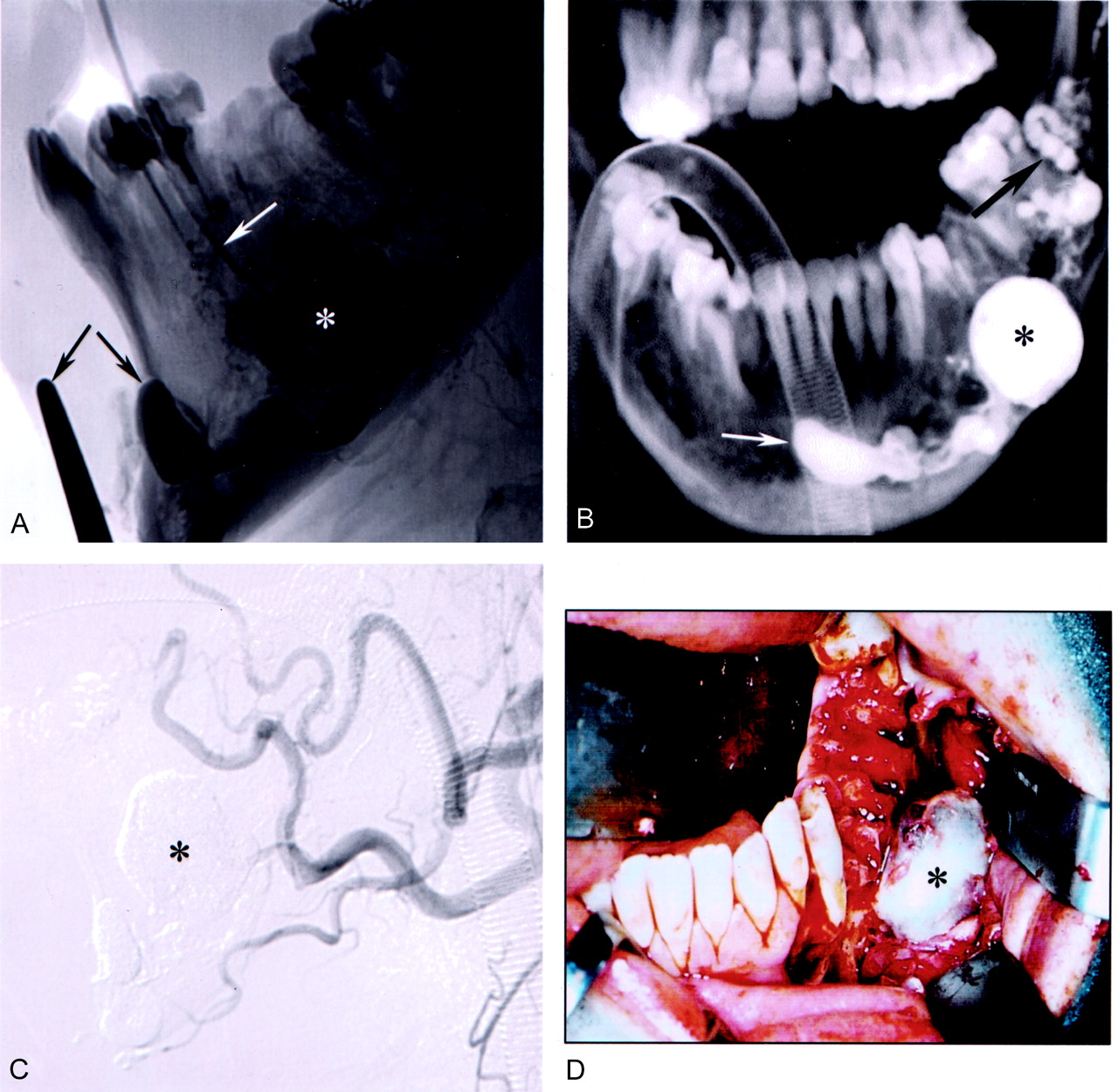
First, the arterial supply from the facial artery was excluded by using polyvinyl alcohol particles (350–500 μ and 500–700 μ). Five days later, a 6F/2F coaxial catheter system was used to superselectively catheterize the left inferior dental artery and embolize with n-butyl-cyanoacrylate (NBCA, 30%) mixed with lipiodol (70%). The tortuous anatomy of this artery precluded distal positioning of the microcatheter for complete filling of the AV-shunt surgery zone. Therefore, direct puncture by using an 18-gauge needle was additionally undertaken and revealed residual AV-shunt (Fig 2A). Manual compression of the draining vein allowed us to deposit 4 mL of NBCA/lipiodol mixture (50%) directly into the lesion, resulting in complete occlusion of the AV-shunt (Fig 2B and C). The needle was removed; no bleeding occurred at the puncture site. Antibiotics (clindamycin) were given to prevent infection or local inflammatory reaction.

Embolization and dental surgery.
A, Left mandibular phlebogram (nonsubtracted view) after direct puncture of the venous varix with an 18-gauge needle (white arrow). The AV shunt is significantly reduced after transarterial embolization and additionally diminished by external compression of the draining vein (arrows) with a metal clamp.
B, Three-dimensional reconstruction obtained by rotational radiography after intralesional injection of NBCA shows the glue cast in the feeding artery (black arrow), the giant venous pouch (asterisk), and the draining vein (mental vein; white arrow).
C, Left external carotid control arteriogram reveals the complete occlusion of the AV shunt.
D, After detaching the mucoperiost flap in the premolar/molar areas, left lower jaw. The glue-filled venous pouch of the AVM (asterisk) is surrounded by the partly loosened osseous lamella and can be removed without significant blood loss.
After another 5 days, we performed an appropriate dental treatment (extraction of teeth 38, 35, 36, and 34 because of intraoperative mobility; radiectomy and endodontal treatment of tooth 33) and a surgical excision of the glued pouch (Fig 2D).
To increase local pressure on the wound, a custom-made polymethylmethacrylate plate was inserted onto the mandible for a total of 3 days. No unusual bleeding was encountered.
After each intervention, the patient received FVIII concentrate and prothrombin complex concentrate to maintain normal levels until the healing process was well underway. The PPSB substitution was continued for 2 days after each intervention. We maintained FVIII levels >70% for another 10 days, modifying the dosage according to the healing process. No postoperative bleeding occurred.
For the administration of the factor concentrate replacement, local hemostatic control of wound healing and laboratory tests (aPTT [activated partial thromboplastin time], PT [prothrombin time, Quick test], FVIII level, platelet count) were performed on a daily basis. The patient was discharged after 21 days.
Discussion
Mandibular AVM
AVMs of the mandible are usually seen, if at all, in children. They are caused by a disturbance in the late stages of angiogenesis (truncal stage) and result in the persistence of arteriovenous anastomoses present in the embryonic stage. Symptoms of mandibular AVMs include bruit, dental loosening, swelling of soft tissue, change in skin and mucosal color, disfigurement, and dysesthesia of the lower lip or chin due to 5th nerve irritation (3). As reported by several authors, they may also cause massive, life-threatening; and sometimes even fatal hemorrhages (1–3).
Radiographically, AVMs most commonly appear as multilocular radiolucencies in panoramic examinations that are usually due to an enlarged, pulsating inferior dental vein. It is interesting that, as seen in our patient, they may also be caused by the dilated tortuous inferior dental artery. Although MR angiography, CT angiography, or Doppler sonography may indicate the AV-shunt lesion, superselective arteriography remains the essential tool for the definite diagnosis and planning of treatment.
Therapeutic management consists of either surgical or endovascular treatment (which today is more common), or a combination of both. Endovascular treatment can be challenging in extended lesions with complex vascular architecture requiring multiple sessions. Because it can be associated with significant blood loss or disfigurement, surgery is not recommended as the treatment of choice before adolescence (3, 5). By contrast, endovascular management will result in effective occlusion only if a permanent embolic agent can be deposited within the AV-shunt zone including the proximal draining vein (3, 6, 7). This is currently best achieved by using a transvenous approach to the lesion with either direct percutaneous puncture or transfemoral venous catheterization and should be preceded by transarterial embolization of the AV-shunt supply. As seen in our case, a seemingly complete transarterial embolization does not guarantee complete occlusion of the AV-shunt surgery zone, and recruitment of new feeding vessels resulting in recurrence and rehemorrhage (3) can be expected. Because of the potential for disastrous bleeding in these patients, treatment should be offered as early as possible.
Hemophilia
Hemophilacs are characterized by a deficiency or dysfunction of FVIII, which has a profound effect on coagulation, resulting in prolonged coagulation times and a tendency to hemorrhage, either spontaneously or as a result of trauma (4, 8). A fairly common clinical classification distinguishes patients with severe hemophilia A, whose plasma has no detectable FVIII (<1%), from patients who have moderate (1%–4%) or mild (5%–25%) hemophilia. This distinction is crucial, because mild or moderate hemophilia A is rarely complicated by episodes of apparently unprovoked bleeding, and some of these patients are detected only because of prolonged postoperative bleeding (8). The association of a coagulation disorder such as hemophilia with a mandibular AVM is extremely uncommon and has, to the best of our knowledge, not yet been described in literature.
Replacement Therapy in Severe Hemophilia A
Severe hemophilia A is currently treated by replacement therapy using plasma-derived FVIII orrecombinant FVIII concentrates. Each FVIII unit per kilogram of body weight infused intravenously is estimated to raise the plasma FVIII level by approximately 1–2%. Because of the increased risk of hemorrhage, extrinsic coagulation factors were raised to normal levels as well by using prothrombin complex concentrate (containing mainly factor 2, 7, 9, 10) and FFP. Today, therapy incorporating differentiated coagulation factor replacement makes it possible to perform even major surgery on hemophilic patients with virtually no complications (9–11). Most authors agree that hemophiliacs can undergo the same kinds of operations as nonhemophiliacs if preoperative and 2-week postoperative coagulation factor activity is maintained at 50% or more of normal levels (9, 12). Both Nakau et al (9) and Andrews et al (10) reported the successful surgical removal of intracranial AVMs in patients with hemophilia A without complications. MacKinlay et al (11) reported on 12 patients undergoing cardiac surgical procedures, including cardiac catheterization, bypass surgery, and angioplasty. In his group of patients, hemostasis was achieved by either intermittent bolus factor therapy or continuous intravenous infusion leading to excellent intra- and postoperative hemostasis.
The unusual combination of two pathologies, each carrying a serious risk of hemorrhagic complications, caused a 10-year delay in the appropriate diagnosis and therapeutic management of the patient, despite the fact that the pulsating mass had increased in size. Today, the presence of hemophilia A should not compromise the appropriate diagnostic investigation and therapeutic management of an AV-shunt malformation, particularly when there is such high potential for bleeding. Even a minimal trauma may have easily fractured the thinned and partially disrupted mandibular bone, causing rupture of the AVM.
In conclusion, hemophilic patients can undergo the same surgical or endovascular therapy, including direct percutaneous puncture of an arteriovenous shunt lesion, as patients without coagulation disorders. These patients can anticipate high success rates, given optimal use of available resources, capacities, and appropriate perioperative management by a multidisciplinary team in cooperation with a hemophilia treatment center. To prevent fatal bleeding, as well as secondary concomitant diseases liable to cause further complications, we recommend endovascular treatment in mandibular AVMs at the earliest possible stage.
References
- Received June 4, 2003.
- Accepted after revision July 8, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}