
Abstract
BACKGROUND AND PURPOSE: Asymptomatic microbleeds shown by T2*-weighted MR imaging are associated with small-artery diseases, especially with intracerebral hemorrhage. Few studies have focused on the prevalence of microbleeds in patients with recurrent stroke. We investigated frequency of microbleeds in patients with recurrent stroke and association of presence of microbleeds with a combination of stroke subtypes and severity of leukoaraiosis.
METHODS: The study population consisted of 102 patients with primary stroke and 54 patients with recurrent stroke. Microbleeds were counted and classified by using T2*-weighted MR imaging with a 1.0-T system.
RESULTS: Patients with recurrent stroke showed a significantly higher prevalence of microbleeds (68.5%) than did patients with primary stroke (28.4%) (P < .0001). Among patients with recurrent stroke, the highest frequency of microbleeds occurred in those with intracerebral hemorrhage alone (92.3%), with the next highest frequency occurring in those with a combination of intracerebral hemorrhage and ischemic stroke (76.5%) and then those with ischemic stroke alone (50.0%) (P < .05). Leukoaraiosis was more severe in patients with recurrent stroke than in patients with primary stroke, and correlations between grade of microbleeds and severity of leukoaraiosis were found in patients with primary stroke (r = 0.367, P < .001) and in patients with recurrent stroke (r = 0.553, P < .0001). Logistic regression analysis identified recurrent stroke (odds ratio, 4.487; 95% confidence interval, 1.989−10.120) and leukoaraiosis (odds ratio, 5.079; 95% confidence interval, 2.125−12.143) as being significantly and independently associated with microbleeds.
CONCLUSION: Asymptomatic microbleeds are observed to occur frequently in patients with recurrent stroke, either hemorrhagic or ischemic stroke, and are closely associated with the severity of leukoaraiosis.
Gradient-echo T2*-weighted MR imaging is extremely sensitive for detecting silent microbleeds, which are shown as signal intensity loss, representing hemosiderin deposit (1, 2). Recent studies using T2*-weighted MR imaging have shown a high frequency of microbleeds in patients with severe leukoaraiosis, lacunar infarction, and cerebral hemorrhage, indicating that an association exists between microbleeds and small-artery disease (3–10).
Recurrent stroke potentially affects the prognosis and physical and psychologic disability of the patient, and it is extremely important not only to prevent recurrence of stroke by antiplatelet or anticoagulation therapy or by control of risk factors but also to assess which patients are prone to recurrence by using neuroradiologic tools. Previous stroke trials have revealed considerable recurrence of stroke despite treatment with antiplatelet or anticoagulation therapy for the prevention of recurrence (11–16), but characteristic neuroradiologic findings of patients who are prone to recurrent stroke have not been elucidated. T2*-weighted MR imaging is expected to have the potential to identify those patients who are prone to recurrence. However, few studies have focused on the prevalence of microbleeds in patients with recurrent stroke. Recognition of microangiopathy that causes a patient to be prone to bleeding is extremely important, and T2*-weighted MR imaging could be useful if the presence of microbleeds on T2*-weighted MR images enables prediction of the recurrence of specific stroke subtypes. Therefore, the aim of the present study was to evaluate frequency of microbleeds in patients with recurrent stroke and association between presence of microbleeds with combination of stroke subtypes and findings on conventional MR images and MR angiograms.
Methods
We prospectively evaluated inpatient and outpatient subjects with acute primary or recurrent stroke who underwent MR imaging studies at our hospital from September 2002 to March 2003. Histories of neurologic episodes were carefully obtained from the patients and/or their families. Diagnosis of acute stroke was made on the basis of neurologic signs and symptoms and on the basis of results of neuroradiologic examinations. Stroke was classified into ischemic stroke and intracerebral hemorrhage, and ischemic stroke was further classified according to the criteria of the National Institute of Neurologic Disorders and Stroke as atherothrombotic infarction, cardioembolic infarction, and lacunar infarction (17). Cases of undetermined classification were excluded from this study. Acute ischemic stroke was confirmed based on diffusion-weighted images and apparent diffusion coefficient maps, and intracerebral hemorrhage was diagnosed on the basis of CT findings. Cases in which hematoma was not caused by spontaneous intracerebral hemorrhage (eg, caused by vascular malformation, trauma, cavernous hemangioma, or brain tumor) were excluded from this study. The requirement for diagnosis of previous stroke was symptomatic episodes that had been diagnosed as stroke and had been treated; cases with lesions suggestive of stroke on MR images alone without neurologic symptoms were not diagnosed as recurrent stroke. In patients who had suffered recurrent stroke, the subtype of the previous stroke and whether they had undergone antiplatelet or anticoagulation therapy after the previous ischemic stroke were evaluated. Subsequent worsening of the same neurologic dysfunction after continuous disturbance of focal neurologic function after the acute stroke was not recognized as recurrent stroke.
All patients in the study were examined with the use of a 1.0-T clinical MR imaging unit (Siemens, Magneton Harmony), and the whole brain was imaged with a section thickness of 5 mm and intersection gap of 1.5 mm. The imaging protocol consisted of axial view T2-weighted spin-echo sequences (4500/112 [TR/TE]; field of view, 201 × 230; matrix, 225 × 512), axial view T2*-weighted gradient-echo sequences (800/26; flip angle, 20 degrees; field of view, 230 × 230; matrix, 192 × 256), diffusion-weighted imaging with single shot echo-planar spin-echo sequences (5300/135; field of view, 196 × 261; matrix, 80 × 128; b values, 0 and 1000 mm2/s), and intracranial MR angiography (3D time-of-flight sequence; 39/10; field of view, 150 × 200; matrix, 192 × 512). Patients were excluded if their MR images could not be evaluated because of artifacts.
Microbleeds were defined as homogeneous, round hypointense lesions on T2*-weighted MR images, excluding lesions in the globus pallidum and in the subarachnoid space, which are likely to represent calcification and adjacent pial blood vessels, respectively. Intracerebral lesions with a hemorrhagic component were also excluded. Microbleeds were classified as absent (grade 0), mild (grade 1; total number of microbleeds, one to two), moderate (grade 2; total number of microbleeds, three to 10), and severe (grade 3; total number of microbleeds, >10) according to the grading scale presented by Lee et al (18). MR angiography was used to examine intracranial large arteries, including the intracranial internal carotid, anterior cerebral, middle cerebral, posterior cerebral, basilar, and intracranial vertebral arteries, for the presence of intracranial large-artery diseases, defined as >50% luminal narrowing. Arterial occlusion suspected to be due to embolism by thrombus in patients with cardioembolic infarction was not considered to be large-artery disease. Leukoaraiosis shown by T2-weighted imaging was graded by using the scoring system presented by Fazekas et al (19): grade 0, absent; grade 1, punctate; grade 2, early confluent; and grade 3, confluent. MR images were independently evaluated by two of the authors (H.N., E.N.) without knowledge of the patients’ clinical profiles; the number of microbleeds and the grading scores of intracranial large-artery diseases and leukoaraiosis were determined by consensus.
Values were expressed as means ±SD. For the cases of primary and recurrent stroke, the χ2 test for independence was used for comparison of sex ratio, hypertension, atrial fibrillation, diabetes mellitus, hyperlipidemia, and intracranial large-artery diseases, Student’s t test was used for comparison of age, and Mann-Whitney’s U test was used for comparison of grade of leukoaraiosis and microbleeds. Prevalences of microbleeds or intracranial large-artery diseases among the groups were compared by conducting the χ2 test for independence. Prevalences of hypertension and lacunar infarction among the patients with intracranial large-artery diseases with and those without microbleeds were also compared by conducting the χ2 test for independence. Comparisons of grades of microbleeds in three or four groups were performed by the Kruskal-Wallis rank test with post hoc comparisons (Scheffé). Correlation between degrees of microbleeds and leukoaraiosis was examined by using the Spearman rank correlation test. Logistic regression analysis was used to assess the relationships of microbleeds with the following variables: age, sex, hypertension, atrial fibrillation, diabetes mellitus, hyperlipidemia, intracranial large-artery diseases, leukoaraiosis, and primary or recurrent stroke.
Results
The study population consisted of 156 Japanese patients with acute stroke, including 102 (57 men and 45 women; age, 69.0 ± 12.7 years) with primary stroke and 54 (38 men and 16 women; 68.6 ± 11.4 years) with recurrent stroke. Patient data are summarized in Table 1. No statistical differences were observed in age, sex ratio, or prevalences of hypertension, atrial fibrillation, diabetes mellitus, hyperlipidemia, or intracranial large-artery diseases between the primary and recurrent stroke groups. However, the grade of leukoaraiosis was higher in the recurrent stroke group than in the primary stroke group (P < .0001).
Background of the patients
Prevalences and grades of microbleeds in the patients in the primary stroke group are summarized in Table 2. Microbleeds were observed more frequently in patients with intracerebral hemorrhage (47.2% of the patients) than in patients with atherothrombotic infarction (22.7%) or lacunar infarction (22.6%). Microbleeds were not observed in patients with cardioembolic infarction. The grade of microbleeds was highest in patients with intracerebral hemorrhage, with statistical significance for patients with cardioembolic infarction (P < .05). A significant correlation was shown between grade of microbleeds and severity of leukoaraiosis (r = 0.367, P < .001). No significant difference was shown in incidences of intracranial large-artery diseases between patients with primary stroke with microbleeds and patients with primary stroke without microbleeds.
Prevalence and grade of microbleeds in patients with primary stroke
Combinations of stroke subtypes in patients with recurrent stroke are summarized in Table 3. Two patients with intracerebral hemorrhage who had undergone antiplatelet therapy after previous ischemic stroke (cases of lacunar/intracerebral hemorrhage) exhibited severe microbleeds. On the other hand, three patients who had not undergone antiplatelet or anticoagulant therapy after previous ischemic stroke exhibited intracerebral hemorrhage (cases of lacunar/intracerebral hemorrhage), and two of the three exhibited microbleeds. Patients with recurrent stroke had a significantly higher prevalence of microbleeds than did patients with primary stroke (68.5% versus 28.4%, P < .0001). The grade of microbleeds was also significantly higher in patients with recurrent stroke than in patients with primary stroke (P < .0001). Representative T2- and T2*-weighted MR images are shown in Figure 1. The prevalences and grades of microbleeds in patients with ischemic stroke (including atherothrombotic infarction, cardioembolic infarction, and lacunar infarction) alone, in patients with intracerebral hemorrhage alone, and in patients with a combination of ischemic stroke and intracerebral hemorrhage are summarized in Table 4. Frequency of microbleeds was highest in the group of patients with intracerebral hemorrhage alone (92.3%), next highest in the group of patients with intracerebral hemorrhage and ischemic stroke (76.5%), and then in the group of patients with ischemic stroke alone (50.0%) (P < .05). The order of grades of microbleeds was the same: highest in the group of patients with intracerebral hemorrhage alone, next highest in the group of patients with intracerebral hemorrhage and ischemic stroke, and then in the group of patients with ischemic stroke alone (P < .01). Although a significant correlation was found between grade of microbleeds and severity of leukoaraiosis in the patients with recurrent stroke (r = 0.553, P < .0001), no significant difference was observed in incidences of intracranial large-artery diseases between patients with recurrent stroke with microbleeds and patients with recurrent stroke without microbleeds.

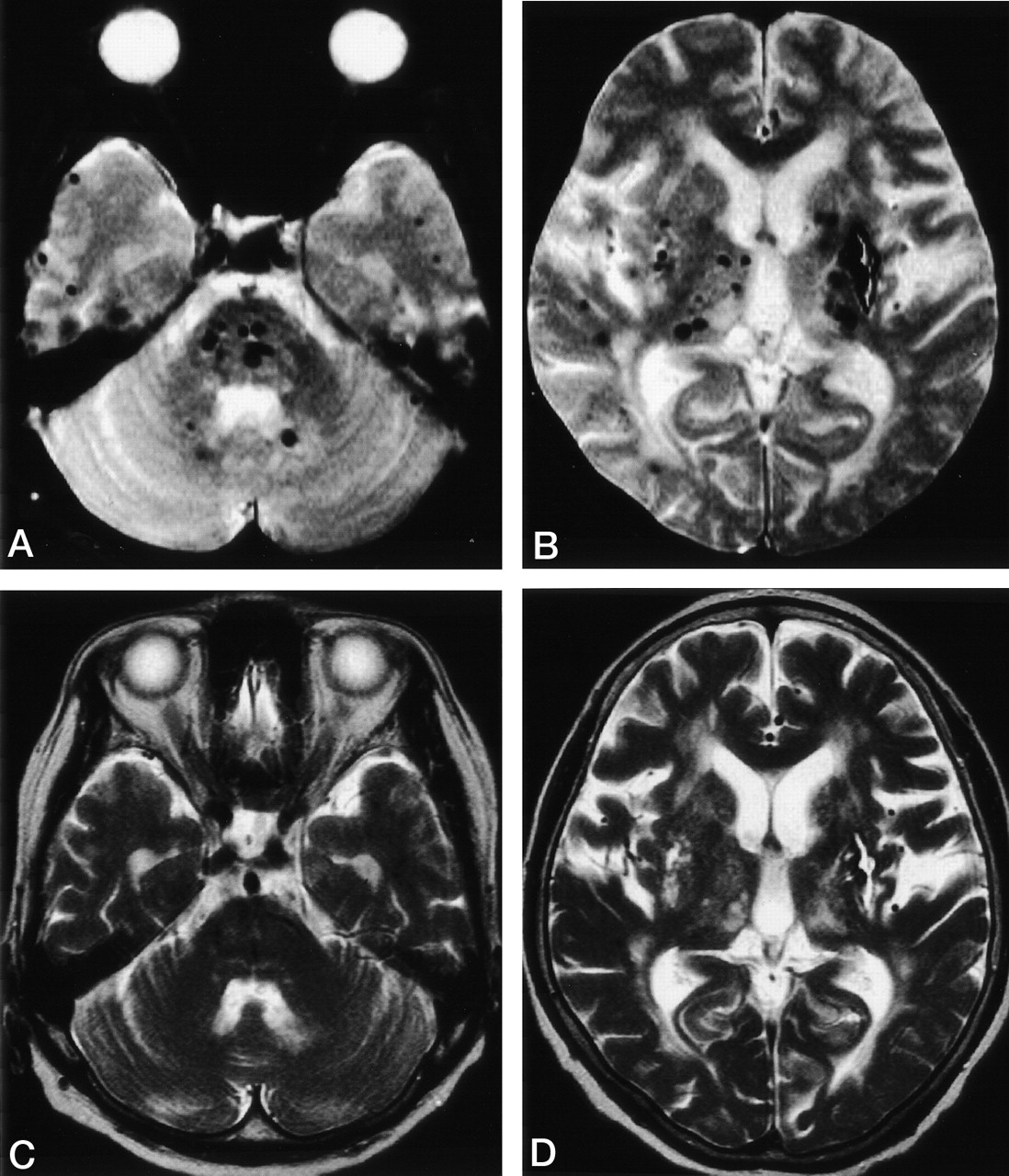
MR images of a 75-year-old patient with intracerebral hemorrhage in the right parietal lobe 8 years after the occurrence of intracerebral hemorrhage in the left putamen.
A and B, T2*-weighted gradient-echo images (800/26; flip angle, 20 degrees) reveal multiple foci of signal intensity loss (microbleeds) in the brain stem, cerebellum, basal ganglia, and cerebral hemispheres. In addition, old intracerebral hemorrhage is evident in the left putamen.
C and D, T2-weighted spin-echo images (4500/112) show the site of old intracerebral hemorrhage in the left putamen, but microbleeds are not evident.
Combination of stroke subtypes in patients with recurrent stroke
Prevalence and grade of microbleeds in patients with each combination of subtypes of recurrent stroke
Among the patients with intracranial large-artery diseases (54 patients), 22 were shown to have microbleeds. Patients with intracranial large-artery diseases and microbleeds showed a significantly higher prevalence of hypertension or lacunar infarction (90.9%) than did those with intracranial large-artery diseases but without microbleeds (59.4%) (P = .0110).
Results of logistic regression analysis showed that recurrent stroke (odds ratio, 4.487; 95% confidence interval, 1.989−10.120) and leukoaraiosis (odds ratio, 5.079; 95% confidence interval, 2.125−12.143) were significantly and independently associated with presence of microbleeds, whereas atrial fibrillation had a significant and independent negative association with presence of microbleeds (Table 5).
Logistic regression analysis
Discussion
In the present study, we evaluated frequency of microbleeds in patients with recurrent stroke and association of microbleeds with combination of stroke subtypes and severity of leukoaraiosis. The following results were obtained: 1) prevalence and grade of microbleeds were significantly higher in patients with recurrent stroke than in patients with primary stroke; 2) microbleeds were observed more frequently and were of higher grade in patients with intracerebral hemorrhage than in patients with either primary or recurrent ischemic stroke but were frequently observed even in patients with recurrent ischemic stroke (prevalence of 50%); and 3) leukoaraiosis was more severe in patients with recurrent stroke than in patients with primary stroke, and a correlation was found between grade of microbleeds and severity of leukoaraiosis in both patients with primary stroke and those with recurrent stroke.
Previous studies using T2*-weighted MR imaging have revealed that there is an association between presence of microbleeds and small-artery disease (3–10), as was also indicated by the results of the present study, which showed a high frequency of microbleeds in patients with intracerebral hemorrhage or severe leukoaraiosis but no association between presence of microbleeds and intracranial large-artery diseases. Association of microbleeds with small-artery diseases but not with intracranial large-artery diseases was further indicated by the results; among patients with intracranial large-artery diseases, those with microbleeds showed a significantly higher prevalence of hypertension or lacunar infarction, which is associated with small-artery disease, than did those without microbleeds. However, to the best of our knowledge, few studies have focused on microbleeds in patients with recurrent stroke. Some studies have included cases of recurrent stroke. Roob et al (5) reported that among patients with primary intracerebral hemorrhage, those with microbleeds more frequently have histories of stroke than do those without. Kato et al (7) revealed a correlation between number of microbleeds and number of intracerebral hemorrhages or lacunar infarctions. However, no detailed evaluation of the combination of stroke subtypes was conducted in those studies.
The present study clearly showed that patients with recurrent stroke had a higher prevalence and higher grade of microbleeds than did those with primary stroke. In addition, the prevalences of microbleeds were similar but not exactly the same in patients with primary and recurrent stroke with each subtype of stroke; although microbleeds were associated more with intracerebral hemorrhage than with ischemic stroke in patients with primary and recurrent stroke, their prevalence was high in patients with recurrent stroke with all combinations of subtypes. Association between microbleeds and symptomatic intracerebral hemorrhage has been shown in many studies (8–10, 20–24). Tsushina et al (9) reported that the presence of microbleeds was most significantly correlated with history of hemorrhagic stroke. Microbleeds have been reported to be a risk factor for acute postischemic cerebral hemorrhage (22, 23) and also to be associated with intracerebral hemorrhage in patients with cerebral amyloid angiopathy (20, 21). In addition, some studies have indicated that the presence of microbleeds increases the risk of hemorrhagic transformation in patients receiving thrombolytic therapy for acute ischemic stroke (23) or the risk of aspirin-associated intracerebral hemorrhages (10). In the present study, two antiplatelet-treated cases of intracerebral hemorrhage exhibited severe microbleeds. The presence of microbleeds may identify the patients with bleeding-prone microangiopathy, by which decision of using antiplatelet or anticoagulation therapy after ischemic stroke would be possible. Cohort studies are needed to clarify whether patients with microbleeds are really prone to bleeding or whether both microbleeds and symptomatic intracerebral hemorrhage occur after the progression of microangiopathy.
The notable findings of this study are the high frequency of microbleeds in patients with recurrent stroke and the different microbleed prevalences in patients with each subtype of recurrent stroke than in patients with each subtype of primary stroke. Not only were extremely high prevalences shown in patients with intracerebral hemorrhage alone and in patients with a combination of intracerebral hemorrhage and ischemic stroke, but also, a relatively high prevalence (50%) was shown in patients with ischemic stroke alone. This may be explained by the more severe leukoaraiosis in patients with recurrent stroke than in patients with primary stroke. Previous studies have revealed that microbleeds are associated with leukoaraiosis (3, 5, 7–9) but not with intracranial large-artery diseases (18), indicating that small-artery disease results in the presence of microbleeds. In addition, leukoaraiosis has been shown to be closely linked with both intracerebral hemorrhage and ischemic injury (25–27). Either rupture or occlusion associated with microangiopathy may result in intracerebral hemorrhage or ischemic stroke, depending on the circumstances. Kim et al (8) revealed that microbleeds are a predictor of intracerebral hemorrhage in patients with no or mild leukoaraiosis but they occur similarly in association with both ischemic stroke and hemorrhagic stroke in patients with advanced leukoaraiosis. Progression of leukoaraiosis in the course of continuous disturbance of a small artery related to long-standing exposure to stroke risk factors after primary stroke might result in the appearance of microbleeds and finally result in recurrence of stroke of any subtype, not restricted to intracerebral hemorrhage.
Conclusion
Asymptomatic microbleeds shown by T2*-weighted MR imaging frequently occur in patients with recurrent stroke, either hemorrhagic or ischemic stroke, and the microbleeds are closely associated with severity of leukoaraiosis. The presence of microbleeds may be an increased risk factor for recurrent stroke, and we might be able to identify those patients who are likely to experience recurrent stroke.
Acknowledgments
We are grateful to Drs. Naokado Ikeda, Tsugumichi Ichioka, Koji Nagao, and Kittipong Srivatanakul for assistance in preparing the data for analysis.
References
- Received June 23, 2003.
- Accepted after revision October 14, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Cerebral Microbleeds: Is Antithrombotic Therapy Safe to Administer?
- Brain Regulation of Thrombosis and Hemostasis: From Theory to Practice
- Leukoaraiosis on Magnetic Resonance Imaging Correlates With Worse Outcomes After Spontaneous Intracerebral Hemorrhage
- Association between Carotid Artery Plaque Type and Cerebral Microbleeds
- Cerebral Microbleeds Are Predictive of Mortality in the Elderly
- Previous Statin Use Is Not Associated With an Increased Prevalence or Degree of Gradient-Echo Lesions in Patients With Acute Ischemic Stroke or Transient Ischemic Attack
- Positional Relationship between Recurrent Intracerebral Hemorrhage/Lacunar Infarction and Previously Detected Microbleeds
- Antithrombotic Drug Use, Cerebral Microbleeds, and Intracerebral Hemorrhage: A Systematic Review of Published and Unpublished Studies
- Brain Microbleeds Relate to Higher Ambulatory Blood Pressure Levels in First-Ever Lacunar Stroke Patients
- Cerebral microbleeds in the population based AGES-Reykjavik study: prevalence and location
- Bleeding Risk Analysis in Stroke Imaging Before ThromboLysis (BRASIL): Pooled Analysis of T2*-Weighted Magnetic Resonance Imaging Data From 570 Patients
- Cerebral Microbleeds Are Associated With Lacunar Stroke Defined Clinically and Radiologically, Independently of White Matter Lesions
- Cerebral Microhemorrhages Predict New Disabling or Fatal Strokes in Patients With Acute Ischemic Stroke or Transient Ischemic Attack
- Cerebral microbleeds on MRI: Prevalence, associations, and potential clinical implications