
Abstract
Summary: Calcium pyrophosphate dihydrate deposition (CPDD) disease is a disorder that occasionally affects the temporomandibular joint (TMJ) and temporal bone, causing pain (66.6% of cases), swelling (50%), trismus (36.8%), and hearing loss (22.2%). Diagnosis of CPDD is challenging because clinical symptoms and imaging features are not characteristic and may mimic a chondrosarcoma. When the diagnosis of CPDD of the TMJ is under consideration, conventional radiographs of the wrist or the knee may contribute to the final diagnosis. Imaging features of CPDD are discussed with a review of the literature.
Calcium pyrophosphate dihydrate deposition (CPDD), or “pseudogout,” is an uncommon disorder that primarily affects patients older than 50 years. First described by Zitban and Sitaj in 1958 (1), it is a crystal deposition disease similar to gout. Although gout is defined by deposits of nonrefringent crystals of uric acid, synovial fluid analysis of CPDD patients shows weakly birefringent crystals in polarized light. The most common targets affected by calcium deposits are joints with fibro-cartilaginous menisci (knee and wrist joints).
Case Reports
Case 1
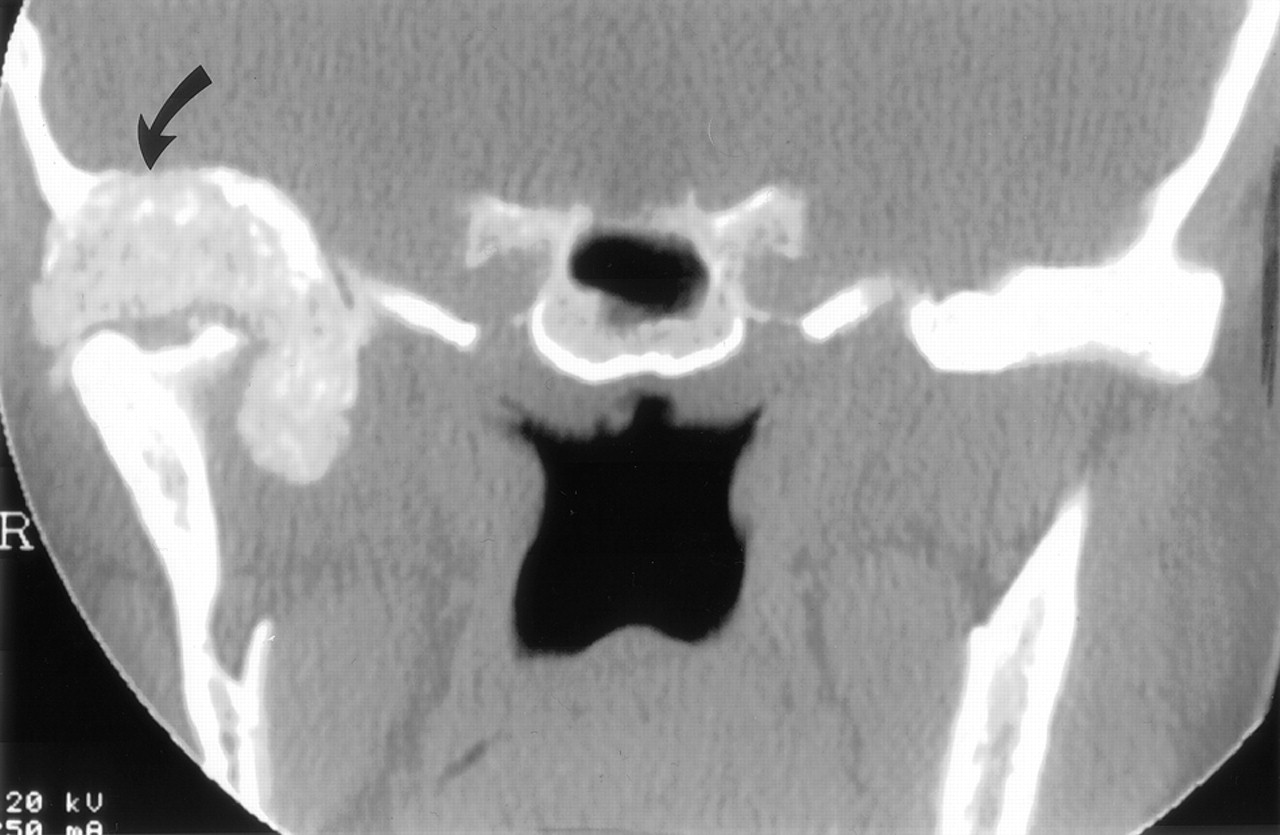
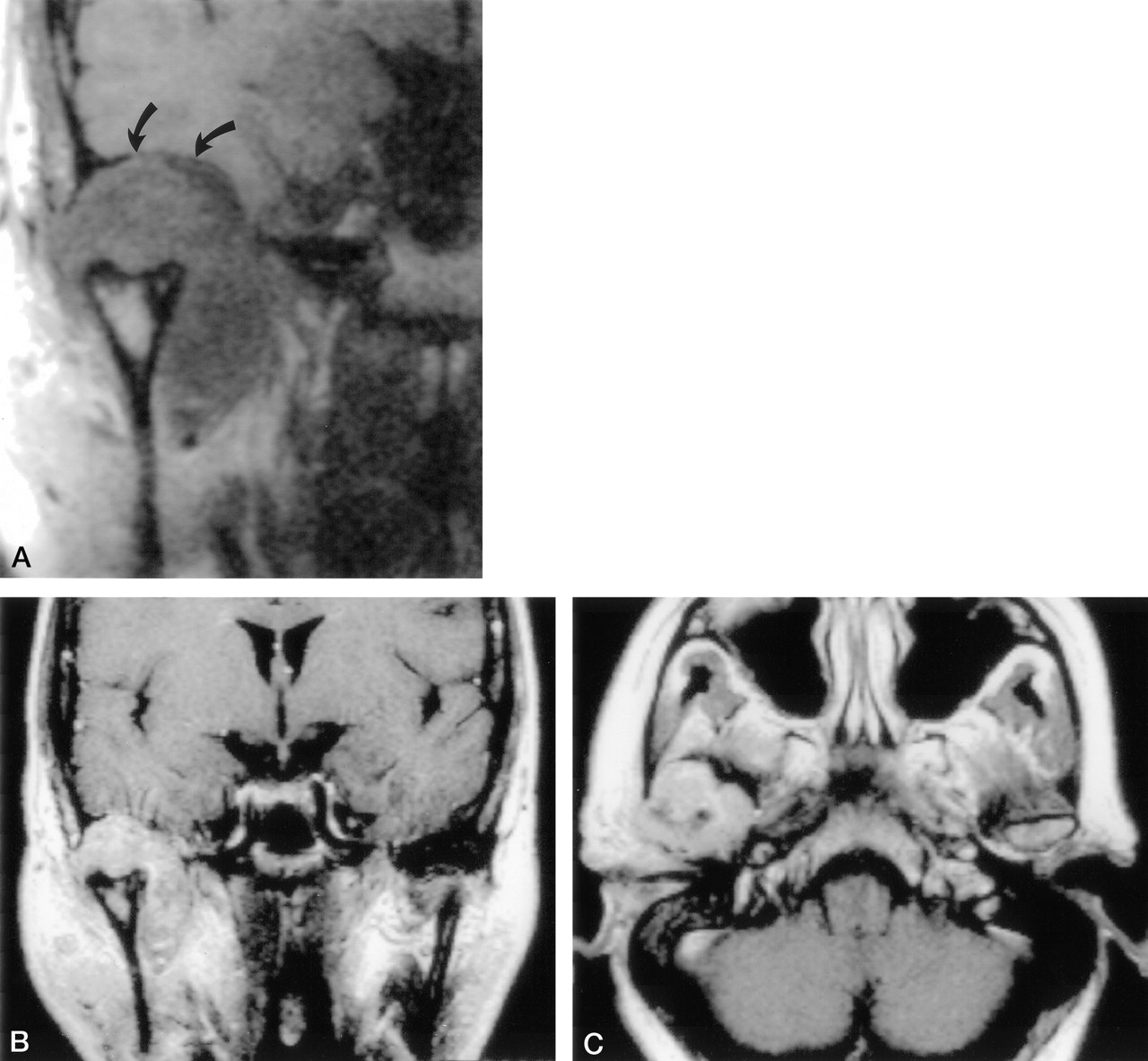
A healthy 70-year-old woman presented with a 10-year history of right temporomandibular joint (TMJ) pain and an ear lump. She was referred for acute worsening, new onset of left TMJ pain, and right-sided hearing loss. Left TMJ pain was successfully treated by steroid eardrops. Hearing function rapidly improved, but the right ear remained painful with a slight increase in pain with jaw movements. CT showed a calcified soft tissue TMJ mass associated with osseous remodeling and widening of the articular space (Fig 1). No other joints were affected, and she had no history of other joint pain. Renal function was considered within normal limits. Because the osseous changes were suggestive of a synovial tumor, MR imaging was performed (Fig 2A–C). An approximately 4-cm heterogeneously enhancing mass was identified, centered in the right TMJ, displacing the mandible inferiorly and expanding the condylar fossa. No abnormal marrow signal intensity or enhancement was noted within the adjacent mandibular condyle. A CT-guided biopsy of the lesion was performed to rule out a chondrosarcoma (Fig 3). Subsequently, detection of birefringent crystals in polarized light established the diagnosis of CPDD disease.

Coronal CT demonstrates a large calcified mass centered within the glenoid fossa bulging into the right middle cranial fossa (arrows). Note mass effect and remodeling of the right mandibular condyle.

Coronal T1-weighted image (A) demonstrates a large TMJ mass of intermediate signal intensity bulging into the middle cranial fossa (arrows). Note marked widening of the joint space (TR/TE/NEX = 358/25/4). Postcontrast T1-weighted coronal (B) and axial (C) images reveal inhomogeneous enhancement of the mass (TR/TE/NEX = 550/25/1).

Needle biopsy under CT guidance. Axial section shows the central position of the needle within the lesion, which encroaches on the middle ear cavity and abuts the ossicles (arrow).
Case 2
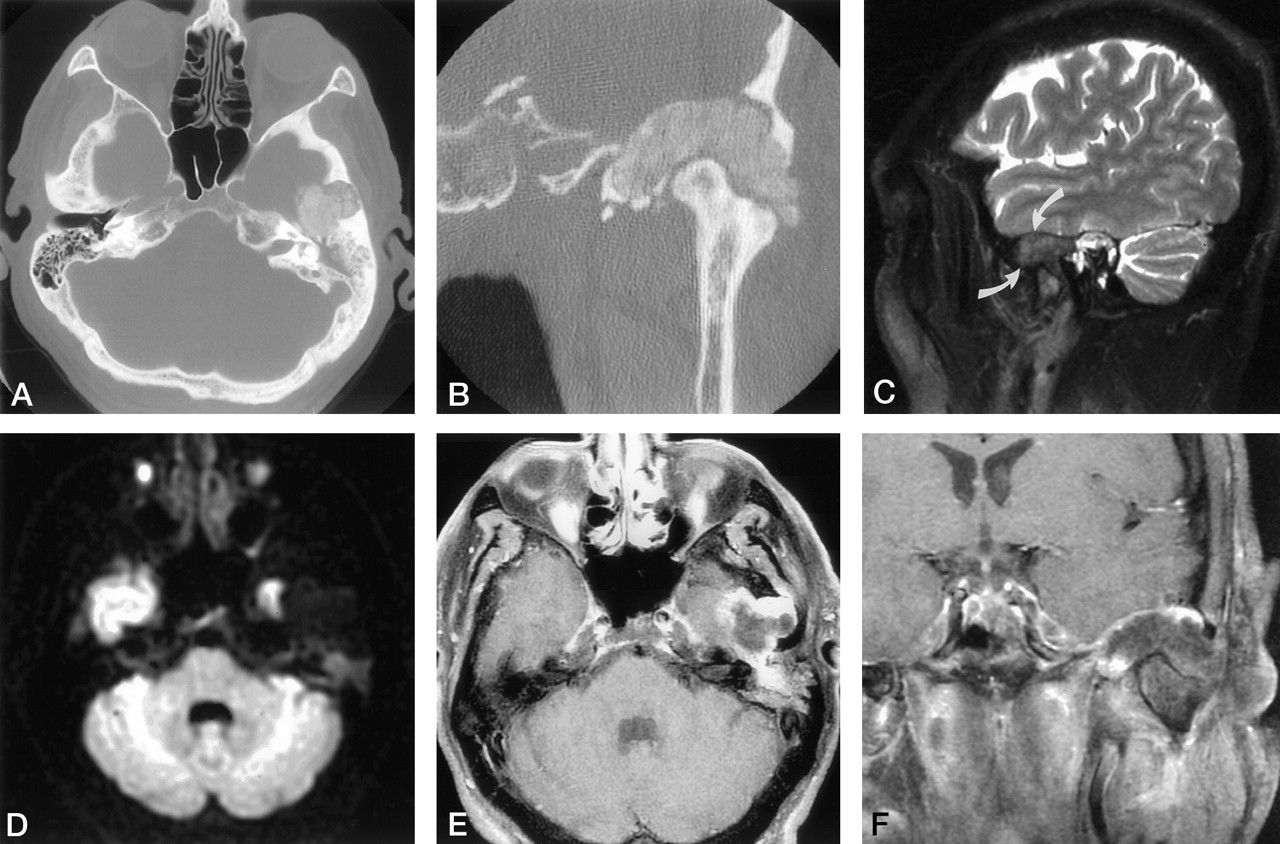
A 53-year-old man was referred for a 1-year history of acute left aural fullness and conductive hearing loss. Found to have otitis media, he had previously been treated at an outside institution with myringotomy and tube placement without improvement in his symptoms. He denied any otorrhea, otalgia, vertigo, or tinnitus. Before the past 1.5 years, he had no history of recurrent ear infections. Medical history was notable for insulin-dependent diabetes. Clinical examination demonstrated an opaque left tympanic membrane. Both MR and CT images demonstrated a large mass centered in the glenoid fossa eroding into the middle cranial fossa (Fig 4). Synovial osteochondromatosis was suspected, although a low-grade chondrosarcoma could not be excluded. Under general anesthesia, a biopsy of the mass was performed via a preauricular approach. Multiple biopsies were sent for frozen and permanent sections. Frozen section demonstrated crystalline material within a benign-appearing stroma.

Axial (A)and coronal (B) CT images demonstrate a hyperattenuated mass eroding the roof of the glenoid fossa, abutting the Eustachian tube, and remodeling the mandibular condyle. Sagittal T2-weighted MR image (C) reveals the mass of low signal intensity (arrows) centered within the TMJ anterior to high signal intensity of fluid within the mastoid air cells (TR/TE/NEX = 3000/100/2). Diffusion-weighted image (D) demonstrates restricted diffusion. Axial (E) and coronal (F) contrast-enhanced T1-weighted images reveal a large lobulated mass eroding the squama, extending into the middle cranial fossa, with a superficial rim of enhancement (TR/TE/NEX = 600/20/2)
Discussion
CPDD is a metabolic disease associated with periarticular and intra-articular calcification, known as chondrocalcinosis (1). Men and women older than 50 years are equally affected. According to frequency of occurrence, main target sites are the knee, symphysis pubis, hand, wrist, hip, shoulder, and spine.
Acute and chronic forms are reported (2). The acute form more frequently affects the knee and is characterized by joint effusion. The less frequent, chronic form is usually indistinguishable from osteoarthritis. The TMJ is more commonly affected in the chronic form than in the acute form. Of 36 reported cases of chronic CPDD, 20 involved the TMJ (3).
Symptoms related to joint involvement are restricted motion, morning stiffness, and contractures. The most frequent complaints of patients with TMJ CPDD are pain (66.6% of cases), joint swelling (50%), trismus (36.8%), abnormal occlusion (22.2%), and conductive hearing loss (22.2%). Some patients may be asymptomatic (2, 4–16). Conductive hearing loss is related to middle ear effusion, which decreases after myringotomy but rapidly reaccumulates. This unusual location of CPDD may be mistaken for a chondrosarcoma as extensive destruction of the temporal bone may be present.
A variety of names have been given to massive CPDD, including “tophaceous pseudogout,” “pseudotumor,” “destructive CPDD arthropathy,” and “CPDD deposition disease.” “Pseudodegenerative” joint disease, “pseudogout,” or “pseudoneuropathic” patterns are reported (3).
Patients with TMJ CPDD may present with degenerative articular changes of the condyle and temporal bone. CT usually demonstrates a calcified mass involving the joint space with degenerative changes of the surrounding bones (articular space narrowing, osteophytosis, subchondral cyst formation).
MR features have rarely been described, except in tumoral forms, which demonstrate low signal intensity periarticular formation on T2-weighted images. Postcontrast T1-weighted images demonstrate inhomogeneous enhancement of the articular mass, probably linked to a foreign body granulomatous inflammation due to periarticular crystal deposits. Low signal intensity periarticular formation may be encountered in other cartilaginous diseases such as amyloid, gout, and synovial chondromatosis, as well as post-traumatic sequelae.
Rarely, CT imaging features may suggest an expansile bony or cartilaginous proliferative mass of the condylar fossa. Furthermore, extensive destruction of the temporal bone may suggest a malignant tumor such as a chondrosarcoma. Diagnosis is based upon identification of calcium pyrophosphate crystals in synovial fluid; however, synovial fluid aspiration may not be diagnostic. Extensive cellular metaplastic chondroid tissue with pleomorphic hyperchromatic nuclei present in periarticular tissue with crystal deposits may lead to a misdiagnosis of malignancy and unnecessary surgery (2).
Metabolic diseases such as gout and primary or secondary hyperparathyroidism may cause calcium deposits in periarticular areas. Birefringence of intra-articular crystals in CPDD differs from that of gout.
The diagnosis of CPDD remains challenging, because the disease may mimic chondrosarcoma or chondroblastoma. Diagnosis is based on involvement of multiple joints (approximately 50%) (4) and on fine needle aspiration/biopsy. Unfortunately, this examination may be insufficient to ascertain a correct diagnosis (2).
Deposition of calcium-containing crystals in articular tissues is probably under-recognized. It occurs within the synovial membrane and the joint capsule as well as tendons and ligaments. Radiologically, these deposits may give rise to cloudlike synovial calcifications, fine irregular joint calcifications, and linear calcification spreading far from the joint. Tumorous calcified collections are occasionally observed, especially in the digits, but also in the TMJ (13–18).
The cause of CPDD is still under discussion. Crystal deposits are probably related to damage of the cartilage from trauma or chronic inflammation (16). Recent studies suggest that crystal deposits amplify the degenerative process as the presence of these crystals in the articular space stimulates secretion of cellular proteases to clear the joint (19). Therefore, treatment of CPDD is based on prevention of crystal formation, dissolution of crystals, and decrease of biologic consequences of crystal-cell interactions. Lavage of the joints or repeated aspiration with injection of intra-articular hyaluronan is proposed for therapeutic management of these patients. Surgical excision of the calcified mass may be attempted to improve joint mobility.
Conclusion
The diagnosis of CPDD should be considered when evaluating patients with pain or a swollen TMJ. It should be included in the differential diagnosis of periarticular soft tissue calcifications because this disease may commonly mimic a bone tumor. Unenhanced CT is the best imaging technique to establish the diagnosis. When the diagnosis is doubtful, conventional radiographs or CT of the wrist or of the knee may contribute to the diagnosis by demonstration of calcium deposition in the menisci (knees) or triangular cartilages (wrist). Diagnosis by MR imaging is difficult, because subtle forms of CPDD may be completely overlooked and “tumoral” forms may mimic a cartilaginous malignancy; however, any low signal intensity periarticular formation on T2-weighted images should suggest the diagnosis of CPDD.
References
- Received March 24, 2003.
- Accepted after revision August 23, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.