
Abstract
Summary: We report a rare complication following parent-artery occlusion in a patient with radiation-induced carotid pseudoaneurysms. Both the right internal carotid artery pseudoaneurysm and the recurrent external carotid artery pseudoaneurysm were treated by parent-artery occlusion with coils. Although rebleeding was not observed after the second embolization, angiography and endoscopy at the 12-month follow-up showed dispersion and migration of coils into the pharynx and the external auditory canal due to progressive radiation necrosis.
Radiation-induced carotid artery pseudoaneurysm is a rare complication of radiation therapy for head and neck carcinoma, but it is a life-threatening disease. Surgical treatment for such a condition is quite difficult because of the fibrous tissue surrounding the carotid artery and the fragile vascular wall caused by radiation. Owing to recent advances in the technology of interventional radiology, several cases treated successfully by endovascular techniques, including coil embolization with or without stent placement, have been reported (1–5). The long-term results of these treatments, however, remain unclear. We present a case with radiation-induced internal carotid artery (ICA) pseudoaneurysm treated by coil embolization of the ICA. Progressive radiation necrosis and dispersion of coils were observed during the 14-month follow-up period after the occlusion of the ICA.
Case Report
A 58-year-old man was admitted in July 2002 because of repeated epistaxis of several days’ duration. In 1985, the patient had nasopharyngeal carcinoma treated by systemic chemotherapy with 80 mg of cisplatinum and external beam irradiation with a dose of 60 Gy by the two opposite lateral-field techniques. In 1991, he underwent partial resection of the right mandible under the diagnosis of radiation-induced osteonecrosis. Pharyngoscopy and otoscopy at admission showed an ulcer with a clot at the right pharynx and the external auditory canal. A biopsy of the right pharynx showed granulation tissue and necrosis.
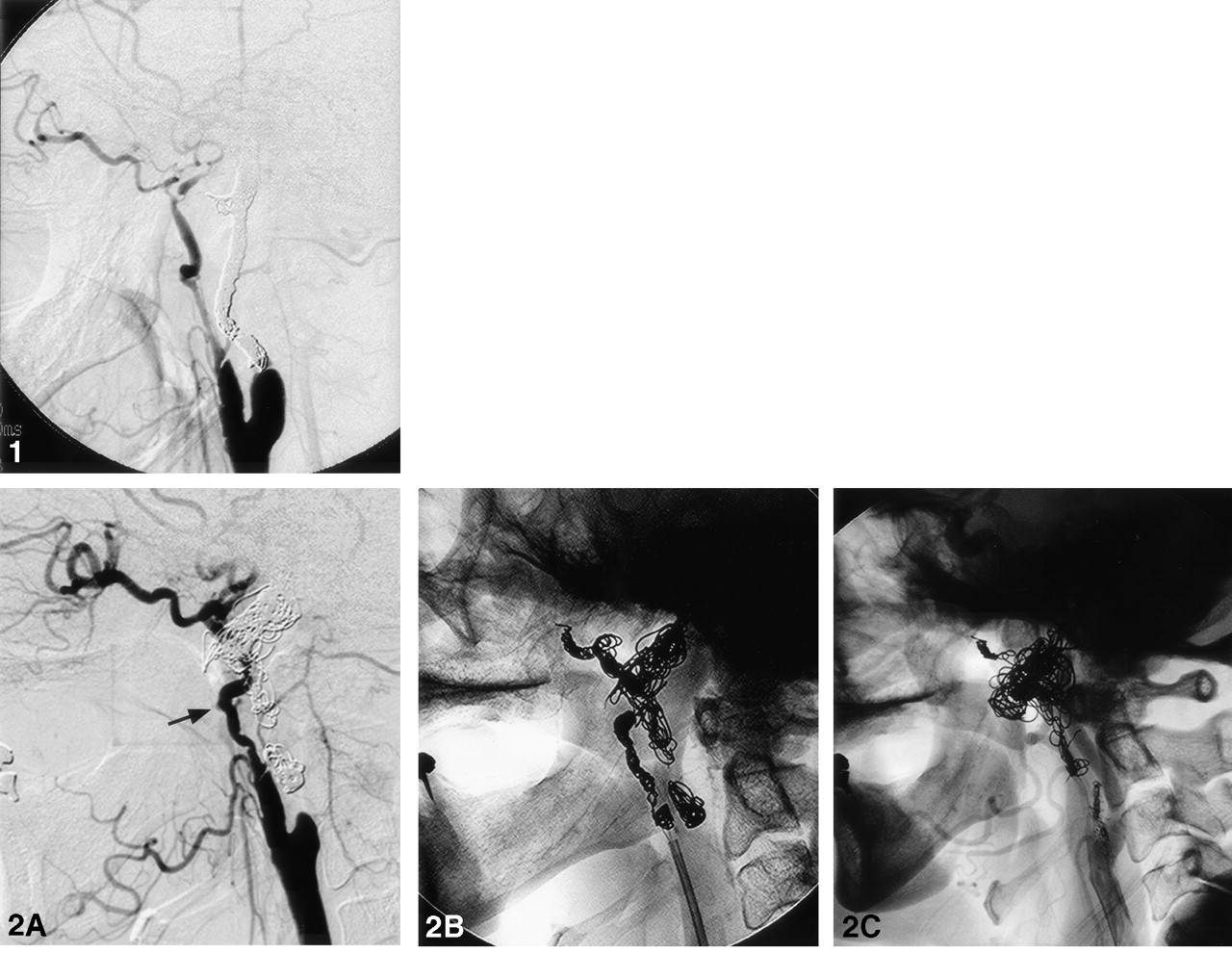
Two days after admission, severe epistaxis and otorrhagia occurred. The right common carotid angiogram showed a pseudoaneurysm at the pharyngeal portion of the right ICA and significantly irregular narrowing of the right ICA and external carotid artery. The left common carotid angiogram obtained with temporary balloon occlusion of the right ICA showed sufficient collateral flow via the anterior communicating artery. Endovascular occlusion of the right ICA was performed. Under temporary balloon occlusion of the right ICA with a 6F balloon catheter, 12 detachable coils (Detach 18; Cook Europe, Bjaerverskov, Denmark), and two fibered minicoils (Target Therapeutics/Boston Scientific, Fremont, CA) were placed tightly in all portions of the ICA included in the radiation field (Fig 1).

Angiogram obtained after embolization shows complete occlusion of the ICA with coils tightly packed in all affected portions of the right ICA.
An angiogram obtained after embolization showed total occlusion of the right ICA and good collateral supply via the anterior communicating artery. Left hemiparesis, probably due to hemodynamic infarction, occurred 2 days after embolization. The hemiparesis gradually improved, and he was discharged with mild disability. Three months after the embolization, he presented again with recurrent otorrhagia. Otoscopy and pharyngoscopy showed progression of the ulceration with a clot. Cerebral angiography showed a small pseudoaneurysm at the right internal maxillary artery (Fig 2A). The right ICA showed stable complete occlusion, although the coils were dispersed and had migrated into the surrounding tissue. Embolization of the external carotid artery was performed again with seven detachable coils. A postembolization angiogram showed complete occlusion of the external carotid artery (Fig 2B). The patient remained well without recurrence of severe hemorrhage.

Follow-up angiograms obtained 3 and 12 months after embolization of the right ICA.
A, Right common carotid angiogram obtained 3 months after embolization of the right ICA shows a small aneurysm of the right internal maxillary artery (arrow).
B, Fluoroscopic image obtained after embolization of the ECA shows that the coils are placed in the ECA from the distal portion of the internal maxillary artery to the origin of the ECA. Note the dispersion of the coils previously placed in the ICA.
C, Fluoroscopic image obtained 12 months after the first intervention shows further dispersion of the coils.
Follow-up angiography 10 months after the second embolization showed stable occlusion of the right internal and external carotid arteries. Further progression of the dispersion of coils, however, was also noted (Fig 2C). Concomitant endoscopy showed ulceration of the right pharynx and right external auditory canal had progressed and migrated coils were observed in the ulcer. Repeat biopsy of the ulcer showed granulation tissue and necrosis without findings of malignancy.
Discussion
Rupture of the carotid artery is highly associated with radical head and neck surgery and occurs frequently within a few months after radiation therapy, but only rarely more than 10 years after irradiation (6). The pathogenesis of radiation-induced carotid artery aneurysm is still speculative. Some authors have suggested that the accelerated atherosclerosis is the essential pathogenesis of radiation-induced aneurysm. The angiographic findings of radiation-induced stenosis, however, are more severe and longer segmentally than those of standard atherosclerosis. In the case presented herein, disruption of the carotid arteries and necrosis of the surrounding tissue were in progress within a few months. These processes would not be caused by accelerated atherosclerosis alone.
A few case reports of carotid rupture have described histologic findings (7, 8). Okamura et al (7) described the histopathologic findings of two cases of carotid artery rupture after the irradiation. The histopathologic examination of two cases showed carotid artery necrosis. Silverberg et al (8) reported postmortem findings of a radiation-induced aneurysm that included an incomplete and fragmented endothelial lining, resulting from focal loss of endothelial cells. Injuries to the endothelial cells, ground substance, elastic lamina, and smooth muscle of the vessels involved have been proposed as the primary pathogenic mechanisms. Accelerated atherosclerosis caused by the irradiation would also promote formation of the pseudoaneurysm.
Recent studies on endovascular treatment of the carotid artery pseudoaneurysm showed good short-term results (1–5). Most cases are currently treated by the endovascular technique of parent-artery occlusion with a detachable balloon or coils, or a combination of the two (1, 2). Endovascular stent placement has also been employed in limited cases intolerable of carotid artery occlusion (3–5). Although these reports describe relatively good results, they include various causes such as penetrating trauma, surgical procedure, dissection, and irradiation. In radiation-induced carotid artery injury, all arteries and arterial segments with the surrounding tissue in the radiation field would have radiation-induced damage. Therefore, recurrent bleeding can occur from any site in the radiation field.
The case herein raises some important issues in the treatment of radiation-induced ICA pseudoaneurysm. Parent-artery occlusion should be performed with coils that are tightly placed in all portions of the ICA included in the radiation field. The use of a detachable balloon alone seems to be inadequate for a radiation-induced ICA pseudoaneurysm, because radiation-induced injury often involves the long segment of the ICA, including its origin, and is often associated with significant stenosis. Early migration of the detachable balloon due to progressive disruption of the artery may occur. Treatment of cases intolerable of permanent carotid artery occlusion is quite difficult. Bypass surgery is often precluded by prior radiation in the neck. Endoluminal packing of the pseudoaneurysm with coils has a high risk of rebleeding (9). Recently, some authors have described the application of stent-assisted endoluminal packing with coils for such lesions (3–5). Although some cases have been successfully treated by the combined technique, the long-term results are unknown. Collignon et al (10) presented a case of late migration of coil and stent following stent-assisted endoluminal packing with coils of a radiation-induced ICA pseudoaneurysm. More recently, endovascular stent grafts with native venous grafts or synthetic materials such as polytertafluoroethylene have been successfully used in a few cases of carotid artery pseudoaneurysm (5). Endovascular stent grafting would reduce the risk of rebleeding with preserving the patency of the carotid artery when it can be safely placed across the pseudoaneurysm covering all the pathologic portions of the carotid artery. Unfortunately, the endovascular stent grafts currently available are of relatively large size and have a stiff shaft. It would often be difficult to introduce the device into the affected portion of the ICA. Further advances in the technology of materials used for stent grafts, such as reducing the size and improving the flexibility, will provide more sufficient results in the treatment of radiation-induced ICA pseudoaneurysms.
References
- Received August 28, 2003.
- Accepted after revision October 8, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}