
Abstract
Summary: The pattern of venous drainage from a dural arteriovenous fistula (DAVF) has been shown to affect the natural history of these lesions. Angioplasty and stent placement of the dural sinuses have been described to improve outflow in venous hypertensive states and may improve the venous drainage pattern from a DAVF. We report the case of a patient with a benign but stenosed type IIa transverse sinus DAVF who underwent angioplasty to improve venous outflow. This resulted in conversion of the DAVF to a more malignant type IIb drainage pattern with reflux into the cortical venous system.
Dural arteriovenous fistulas (DAVFs) demonstrate a widely variable anatomy and natural history and also may be managed with a variety of treatment options. The classification system for DAVFs proposed by Djindjian and Merland (1) and modified by Cognard et al (2) is possibly the most widely used, and it differentiates lesions primarily on the basis of venous drainage pattern. Type I lesions are generally considered more benign and demonstrate antegrade drainage directly into the venous sinuses. Type II lesions have a more “malignant” course and show retrograde drainage into the dural sinus system (IIa), the cortical veins (IIb), or the dural sinus system and cortical veins (IIa+b). Specific endovascular interventions are dictated by each lesion’s particular anatomy and include obliteration of arterial inflow, occlusion of venous outflow, or some combination of both. An alternative approach, recently described by Murphy et al (3), attempts to re-establish antegrade dural drainage through cortical veins when there is retrograde drainage. We report a case in which a patient with a type IIa DAVF draining into a partially thrombosed transverse sinus underwent angioplasty for recanalization in advance of a stent placement in an attempt to prevent complete thrombosis, and the DAVF developed a more malignant type IIa+b drainage pattern.
Case Report
A 37-year-old male patient presented with persistent headaches and a left-sided bruit approximately 2 years after being involved in an automobile accident. He underwent diagnostic angiography that demonstrated a DAVF in the region of the left transverse sinus near the confluence with the vein of Labbé. The fistula had complex arterial inflow, being fed primarily by multiple branches of the left external carotid artery, including the posterior division of the middle meningeal, superficial temporal, and occipital arteries (Fig 1). The lesion also received flow from the left internal carotid artery via a prominent branch of the meningohypophyseal trunk and from the cervical portion of left vertebral artery via a posterior meningeal branch. Minimal inflow was also demonstrated via a small branch off the contralateral occipital artery. Venous drainage was primarily into the midtransverse sinus with antegrade flow to the sigmoid and internal jugular veins (Fig 1). There were multisegmental stenoses and irregularities of the draining sinuses, and the flow was compromised by these stenoses so that some flow was also noted to be retrograde in the sinus across the torcular herophili into the right transverse sinus. There was no drainage into the cortical veins, making this a type IIa fistula. The vein of Labbé was noted to empty into the transverse sinus in the region of the proximal portion of the malformation. Drainage of the remaining supratentorial left hemisphere was through superficial cortical veins into the superior sagittal sinus, which emptied primarily into the right transverse sinus.

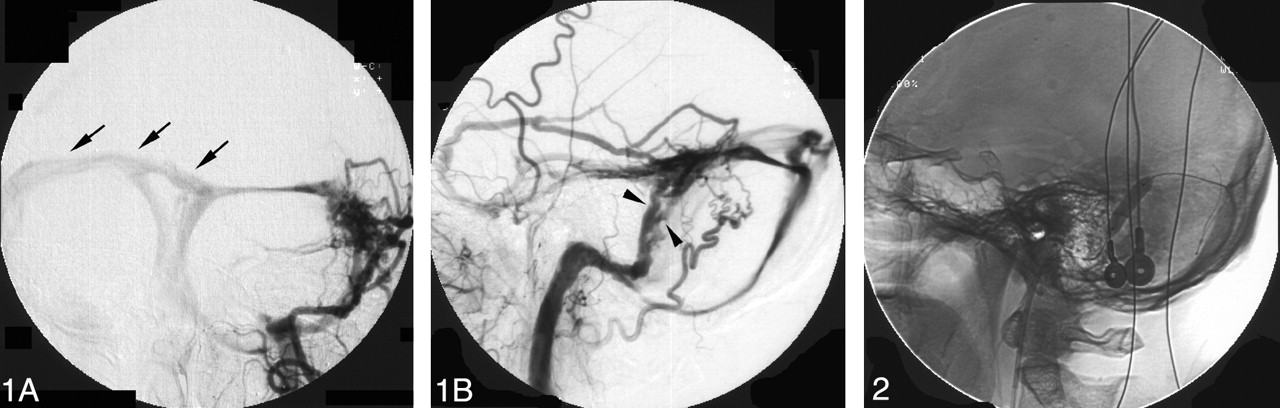
Anteroposterior (A) and lateral (B) angiograms of the left external carotid angiography demonstrate a type IIa DAVF with rapid arteriovenous shunt surgery from multiple branches of the left external carotid artery to the left transverse sigmoid sinus complex. Note multisegmental stenoses of the sigmoid sinus (arrowheads). This may represent a partially recanalized sinus with multiple channels. There is some flow in a retrograde fashion across the torcular herophili into the right transverse sinus (arrows).
Because there was relatively high flow through the fistula and evidence of significant stenoses in the draining sinus with retrograde flow, a sign of early venous hypertension, it was thought that the option of angioplasty and stent placement of the dural sinus might well reduce the possibility of the patient developing a more malignant drainage pattern. Endovascular treatment was performed under conscious sedation by using fentanyl and versed. The left femoral artery was accessed with a 5F sheath, and a 5F catheter was placed in the left external carotid artery on continuous drip after angiograms of the left internal and external carotid artery were obtained.
The right femoral vein was accessed with a 7F sheath. A 6F Envoy guide catheter (Cordis Endovascular Systems, Miami, FL) was then navigated into left internal jugular vein at the junction of the sigmoid sinus. A 0.014-inch guidewire was then advanced across the fistulous portion into the proximal left transverse sinus, and a 4 × 20-mm angioplasty balloon was inserted into the left transverse sinus and expanded. A repeat external carotid artery angiogram demonstrated increased antegrade flow through the transverse sinus, although retrograde flow persisted across the torcular herophili into the right transverse sinus.
We then used a 6 × 20-mm angioplasty balloon in the transverse and sigmoid sinuses in a similar fashion (Fig 2). A repeat external carotid angiogram again revealed rapid shunt surgery from the external carotid branches into the left transverse sinus, with increased flow across the transverse sinus. There was now, however, retrograde filling of an occipital cortical vein arising from the junction of the left transverse and sigmoid sinuses that was not present on the preangioplasty angiograms (Fig 3).

Lateral spot image obtained during angioplasty balloon inflation shows contrast material filled the balloon angioplasty catheter within the left sigmoid sinus in the region of the multisegmental stenoses.

Postangioplasty anteroposterior (A) angiogram from a left external carotid artery injection demonstrates conversion of type IIa to type IIa+b DAVF. Note appearance of a retrograde cortical draining vein in the left occipital region arising from the left transverse sinus (arrows). This cortical draining vein (arrowheads) is better seen on a lateral external carotid artery angiogram (B) after coil placement in the proximal portion of the draining venous pouch.
Because there was now retrograde filling of the cortical venous system, it was decided not to proceed with the plan to perform stent placement. We therefore decided to perform coil embolization of the left transverse sinus and occlude the fistula. A Rapid Transit microcatheter (Cordis Endovascular Systems) was advanced into the left transverse sinus. Coils were placed serially from the mid-left transverse sinus to the junction with the sigmoid sinus and internal jugular vein. Final angiography revealed obliteration of the fistula, and specifically the new occipital cortical draining vein was no longer present (Fig 4). The vein of Labbé, which had emptied into the transverse sinus near the origin of the DAVF, was now redirected to a cortical vein that fed into the superior sagittal sinus. Control angiography of the left internal carotid artery, the right external carotid artery, and the left vertebral artery were also done and showed the fistula was obliterated.

Anteroposterior (A) and lateral (B) angiograms of the left external carotid artery show complete obliteration of DAVF after coil embolization.
Discussion
The approach described by Murphy et al (3) has some theoretical advantages over attempts to occlude arterial supply into or venous drainage from these lesions. They described conversion of a type IV lesion to a type I lesion following angioplasty. Stents were then serially placed into the sinus, and the fistula was completely occluded. The authors thought that the radial force of the stent closed the intramural septations in the wall of the sinus that made up the fistulous communications. The complexities and potential complications involved with treating these lesions make this approach appealing. By recanalizing a thrombosed dural sinus, one may be able to transform a malignant lesion to a more benign one. Certainly more cases would require this treatment before being able to assess what the true benefits (and risks) are for this approach.
A number of reports have highlighted the successful transvenous obliteration of DAVFs (3–7). This approach, however, may not be ideal for all DAVFs. Venous infarction or hemorrhage can occur if collateral venous drainage is inadequate to compensate for the occluded sinus (8). Even rigorous attempts to occlude all the arterial supply may fail to cure the DAVF; expansion of angiographically transparent fistulas or recruitment of entirely new arterial feeders has been reported (3).
This case underscores an important potential complication that can follow endovascular attempts to use angioplasty and stent placement to treat DAVFs. Although we successfully reopened the stenoses in the sigmoid sinus, paradoxically, this caused retrograde flow into a cortical vein that was not seen on the pretreatment angiograms. It is unclear whether this represented an entirely new draining pattern or augmented flow through an existing cortical vein. Prior surgical and pathologic examinations of dural fistulas suggest a possible explanation. Analyses of DAVFs reveal a network of abnormally thickened dural arteries and dilated dural veins infiltrating the wall of the sinus through interruptions of the elastic lamina of the sinus lumen (9). Both Nishijima et al (10) and Barnwell et al (11) have found the key fistulous connection was within the sinus wall, and others have also seen direct fistulous communication within the sinus lumen (11). It is possible that our patient’s lesion was within the dural wall and that, in the process of angioplasty, a connection was established between the fistula and a cortical vein. This is in contradistinction to the report by Murphy et al (3), which suggested that stent placement probably closed these intramural connections. For this reason, we elected to occlude the venous sinus by use of coils.
It is certainly unclear how frequently this complication may arise. In cases in which venous hypertensive disease already exists, re-establishing flow through the venous sinuses with angioplasty may still yield great benefit with a malignant lesion demonstrating cortical venous drainage. It is far too early, however, to assess the risks and benefits of this treatment technique, and data from a far greater number of cases will be necessary before these judgments can be made.
References
- Received April 29, 2003.
- Accepted after revision October 21, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}