
Abstract
Summary: We present two cases of subclavian steal syndrome from the ipsilateral vertebral artery (VA) to the subclavian artery (SCA), one with the left VA originating from the aortic arch and the other with the left VA originating very close to the origin of the SCA, proximal to the occluded segment. In both cases, angiographic demonstration of these anatomic variations and successful endovascular treatment are presented.
Subclavian steal (SS) syndrome is a well-recognized phenomenon. Although color Doppler sonography is a safe method, diagnosis of SS has some difficulties in the presence of antegrade flow in the ipsilateral vertebral artery (VA). We present two cases of SS syndrome from the ipsilateral VA, one with the arch originating from the VA and the other with the VA originating very proximal to the subclavian artery (SCA). In both cases, angiographic demonstration of these anatomic variations and successful endovascular treatment outcomes are presented.
Case Reports
Case 1
A 65-year-old man with a 4-month history of left upper extremity claducation and vertigo was admitted to the hosptial. Neurologic examination revealed pressure difference between the arms (180/100 mm Hg [right], 150/80 mm Hg [left]), cerebellar ataxia, and gait disturbance. He had been taking aspirin 325 mg daily for 2 years after a myocardial infarction.
Color Doppler sonography of VAs revealed a hypoplastic right VA and normal left VA with antegrade flow and normal flow pattern. Total flow volume of the VAs was 220 mL/s (40 mL/s [right], 180 mL/s [left]). Cranial MR imaging showed normal posterior fossa and small-vessel lesions in the supratentorial white matter, and MR angiography of the arch revealed occlusion of the left SCA. The patient was referred to us for diagnostic angiography and endovascular treatment if applicable. Informed consent was obtained for diagnostic angiography and endovascular treatment. Standard digital subtraction angiography (DSA) of the arch and both carotid vertebral systems was performed under local anesthesia via a unilateral femoral approach.
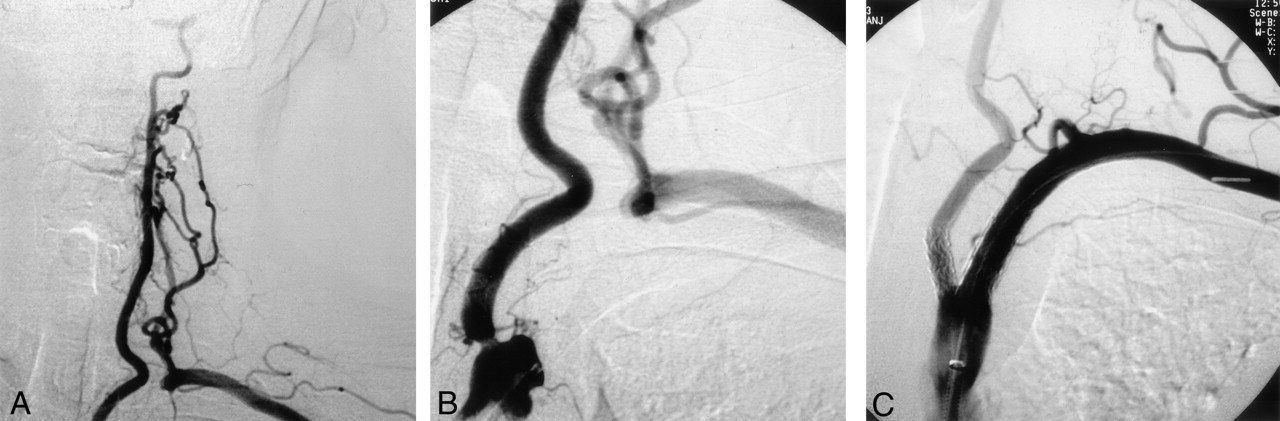
Arcus aortography confirmed occlusion of the left SCA and the arch origin of the left VA (Fig 1A). Selective injections of the right VA demonstrated the presence of a hypoplastic right VA, which terminated as a posterior inferior cerebellar artery (PICA). Selective catheterization of the left VA was possible, because it was originating from the arch and revealed collateral filling of the distal SCA via muscular branches of the ipsilateral VA (Fig 1B). Patent posterior communicating arteries were absent on both sides, and no carotid-vertebral steal was seen.

Case 1, 65-year-old man with SS from the ipsilateral VA and VA origin from the aortic arch.
A, Arcus aortogram shows the arch that originated from the left VA, occlusion of the left SCA, and collateral filling from cervical collaterals.
B, Selective angiogram of the left VA demonstrates SS from the ipsilateral VA.
C, Postoperative left SCA injection reveals good recanalization and filling.
D, Postoperative left VA angiogram shows lack of collateral filling of the left SCA.
The angiography session was extended for the treatment. An anesthesiologist monitored the patient’s oxygen saturation, heart rate, and invasive blood pressure throughout the procedure. The occluded left SCA was recanalized and stent placement was successful (Fig 1C). Control angiography of the left VA demonstrated disappearance of collateral filling of the SCA (Fig 1D).
Postoperatively, the patient received an oral 300-mg loading dose of clopidogrel followed by a daily maintenance dose of 75 mg in combination with 325 mg daily of aspirin. The patient had no adverse events, and his 6-month follow-up angiogram showed no change from the findings of the immediate post-treatment examination.
Case 2
A 60-year-old man was seen for pain in the left upper limb on exertion and vertigo of many years’ duration. Clinical examination revealed an absence of the left brachial and radial pulses as well as significant blood pressure difference between the two arms (160/100 mm Hg [right] and 98/78 mm Hg [left]), gait disturbance, and left upper extremity weakness, but no abnormality on cardiac auscultation.
Color Doppler examination of the brachiocephalic vessels showed occlusion of the left SCA at its origin. Angiography and endovascular treatment were planned with a consulting neurologist, and informed consent was obtained from the patient. Standard DSA of the arch revealed occlusion of the left SCA, patency of the very proximally originated left VA from the SCA with a short segment tight stenosis at its origin, and collateral filling of the distal SCA (Fig 2A). The right VA was normal throughout its course, and selective injection of the right VA did not show flow reversal on the left. Left VA injection revealed antegrade flow and reconstruction of the distal left SCA via muscular branches of the ipsilateral VA. There were no patent posterior communicating arteries on either side, and no carotid-vertebral steal was seen.

Case 2, 60-year-old man with SS from the ipsilateral VA originating from the very proximal segment of the SCA.
A and B, Selective left SCA angiograms show a proximally originated left VA with 70% stenosis at the origin, occlusion of the left SCA, and collateral filling from the ipsilateral VA.
C, Postoperative selective left subclavian angiogram demonstrates good recanalization of the left SCA and no residual stenosis at the left VA origin.
Under local anesthesia and monitoring of oxygen saturation, heart rate, and invasive blood pressure by an anesthesiologist, the occluded left SCA was opened and stent placement was successful (Fig 2B).
The patient received 300 mg clopidogrel as a loading dose just after the procedure, followed by an oral dose of 75 mg in combination with 325 mg of aspirin daily. The patient had no adverse events.
Discussion
SS syndrome is the association of stenotic-occclusive disease of the SCA and cerebrovascular episodes (1, 2). Although color Doppler sonography is a safe diagnostic method in cases with partial steal or in those in which antegrade VA flow is maintained, it might fail. VA flow is cephalad throughout the cardiac cycle, and any deviation from this pattern is abnormal. The features of precursory changes in VA wave forms are a transient sharp decline in blood flow velocities at mid-systole, the rounding of a subsequent second systolic peak, and restoration of forward flow in diastole (1–6).
Although the VA usually originates as the first branch of the SCA, in 6% of the population, the left VA arises directly from the aortic arch (7, 8). VAs comprise two types of cervical branches: muscular and spinal. Multiple, unnamed muscular branches that supply the deep cervical musculature originate from the V2 segment of the VA during its ascent through the transverse foramina (9). In 0.2% of cases, a VA terminates as a PICA (7); in such a case, the VA is small and the opposite VA provides most of the posterior fossa blood supply.
Typical symptoms are episodic dizziness, diplopia, dysarthria, perioral numbness, visual disturbances, and nausea (1, 2). One theory suggests that SS does not produce symptoms of cerebral ischemia in the absence of other arterial lesions, implying that hemodynamically important disease elsewhere in the cerebral arterial circulation is a prerequisite of SS syndrome (4, 10–12). VA origin from the aortic arch or in a very proximal location in the involved SCA and absence of connections between the anterior and posterior circulation would establish SS from ipsilateral VA. Although similar cases have been reported (11, 12), to the best of our knowledge, this is the first report demonstrating angiographic data and endovascular treatment outcomes in the same patients.
When the SS phenomenon presents with dizziness, vertigo, ataxia, visual disturbances, motor deficits, focal seizures, confusion, or syncope, treatment with angioplasty and stent placement has been recommended (2, 10, 11). The first passage of the guidewire and catheter from the occluded segment should be performed carefully to avoid plaque disruption and resultant intracranial emboli (2). Because in both of our cases VAs originated proximal to the occlusion, we did not use a protective device to prevent intracranial embolization. We used our standard antithrombotic drug regimen for carotid and vertebral stents and did not encountered any problem with it.
The origin of the VA from the aortic arch or in a very proximal location in involved SCA and the absence of connections between the anterior and posterior circulation would establish the diagnosis of SS from ipsilateral VA. The anomalous origin of the ipsilateral VA from the aortic arch and very proximal part of the SCA determined peculiar situations in the cases presented herein. The goal of this report was to present angiographic data and successful endovascular treatment in these rare situations with good clinical results.
- Received July 17, 2003.
- Accepted after revision August 10, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.