
Abstract
Summary: We describe a case of carbon monoxide poisoning that led to pallidoreticular damage and delayed leukoencephalopathy. Serial diffusion-weighted MR imaging was performed. A restricted water diffusion pattern was demonstrated in the globus pallidus and substantia nigra in the early stage. Diffusion-weighted imaging is useful for early identification of the effects of acute carbon monoxide poisoning.
MR imaging clearly demonstrates various brain abnormalities following carbon monoxide poisoning (1, 2). Although the lesions more commonly involve the globus pallidus and cerebral deep white matter, they occasionally involve the putamen, caudate nucleus, thalamus, or hippocampus (1, 2). Alterations in the substantia nigra are a less common and conspicuous result of carbon monoxide poisoning (3, 4).
Abnormalities of the white matter on diffusion-weighted images have been reported elsewhere (5–7). To the best of our knowledge, however, diffusion-weighted imaging findings of the pallidoreticular pattern of brain damage due to carbon monoxide poisoning have not been described. We present the serial diffusion-weighted MR imaging findings in a patient with carbon monoxide poisoning with pallidoreticular brain damage.
Case Report
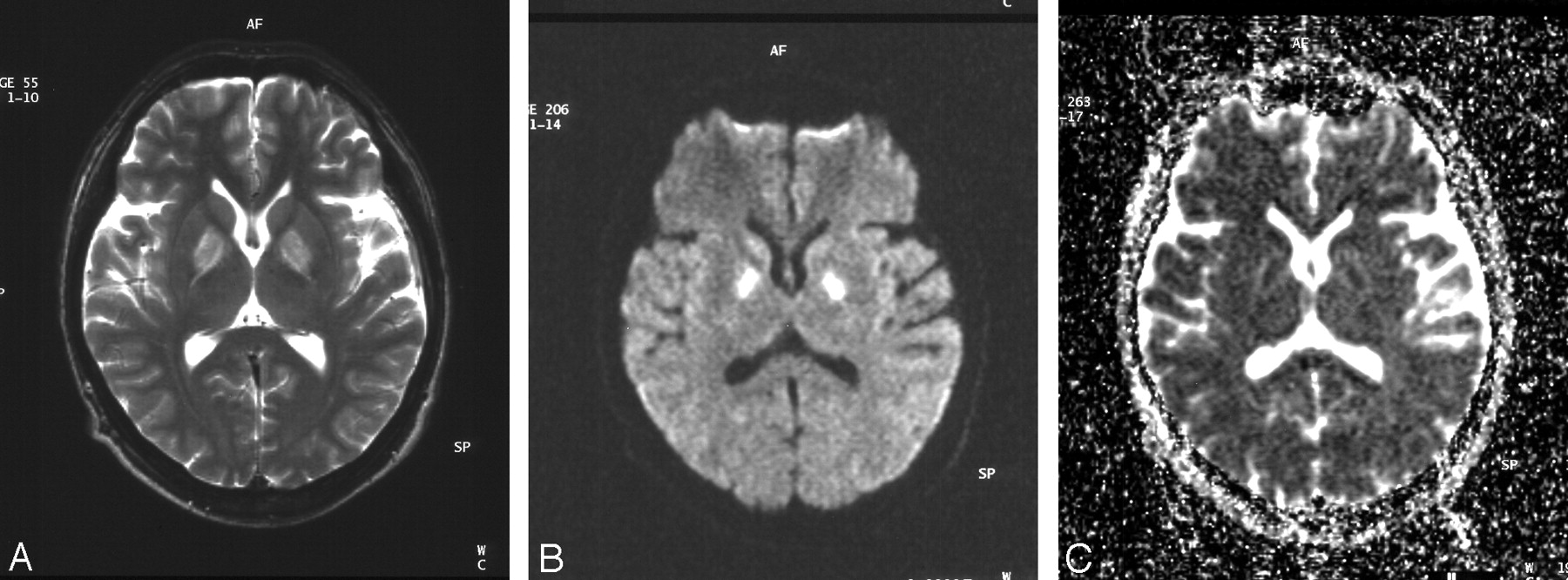
A 35-year-old man was admitted to our hospital in an unresponsive condition. He was found after a fire in an automobile. Hyperbaric oxygen therapy was undertaken. Over the next few days, the patient became more alert. MR imaging was performed 5 days after exposure to carbon monoxide. T2-weighted images showed high signal intensity in the bilateral globi pallidi (Fig 1A).

T2-weighted image obtained 5 days after exposure to carbon monoxide (A) shows symmetrical high-signal-intensity lesions in the bilateral globi pallidi. Diffusion-weighted image (B) reveals symmetrical high-signal-intensity lesions in the globi pallidi. Corresponding ADC map (C) demonstrates low-signal-intensity lesions with high-signal-intensity rims in the bilateral globi pallidi.
Diffusion-weighted imaging was performed by using 2 levels of diffusion sensitization (b = 0 and 1000 s/mm2) acquired in 3 orthogonal orientations to calculate apparent diffusion coefficient (ADC). Diffusion-weighted imaging revealed high signal intensity in bilateral globi pallidi (Fig 1B). On ADC maps, the corresponding regions revealed discrete areas of low signal intensity (Fig 1C). The ADC values of the right and left globi pallidi were 0.76 × 10−3mm2/s and 0.75 × 10−3mm2/s, respectively, whereas the ADC value of the right putamen was 0.86 × 10−3mm2/s. High-signal-intensity rims consistent with vasogenic edema were also noted around the darker restricted areas in the bilateral globi pallidi.
A subsequent MR imaging was performed 12 days after exposure. T1-weighted images showed relatively high-signal-intensity lesions with low-signal-intensity rim in the bilateral globi pallidi (Fig 2A). T2-weighted images showed slightly low-signal-intensity lesions with high-signal-intensity rims in the bilateral globi pallidi (Fig 2B). Coronal T2-weighted images demonstrated high-signal-intensity lesions in the bilateral substantia nigra (Fig 2C). Diffusion-weighted images obtained at the level of the basal ganglia revealed no high-signal-intensity lesions, and no areas of decreased ADC were found in the basal ganglia. Diffusion-weighted images obtained at the level of the midbrain disclosed discrete high-signal-intensity lesions in the pars reticulata of the bilateral substantia nigra (Fig 2D). On ADC maps, the corresponding regions revealed low signal intensity (Fig 2E). The pars compacta of the substantia nigra seemed to be spared relatively on diffusion-weighted images. Hyperbaric oxygen therapy was undertaken until the 18th day after exposure. He was discharged 24 days after exposure to carbon monoxide.

T1-weighted image obtained 12 days after exposure to carbon monoxide (A) shows slightly high-signal-intensity lesions with relatively low-intensity rim in the bilateral globi pallidi. T2-weighted image (B) shows slightly low-signal-intensity lesions with high-signal-intensity rim in the bilateral globi pallidi. Coronal T2-weighted image (C) reveals high-signal-intensity lesions in the bilateral substantia nigra, in addition to high-signal-intensity pallidal lesions. Diffusion-weighted image (D) reveals high-signal-intensity lesions in the pars reticulata of the bilateral substantia nigra. Corresponding ADC map (E) demonstrates low signal intensity in the bilateral substantia nigra.
The patient was readmitted 35 days after exposure to carbon monoxide because he had memory disturbance, dysarthria, urinary incontinence, and Parkinsonian symptoms, including rigidity and gait disturbance. He demonstrated a short-stepping gait. Hyperbaric oxygen therapy was again undertaken.
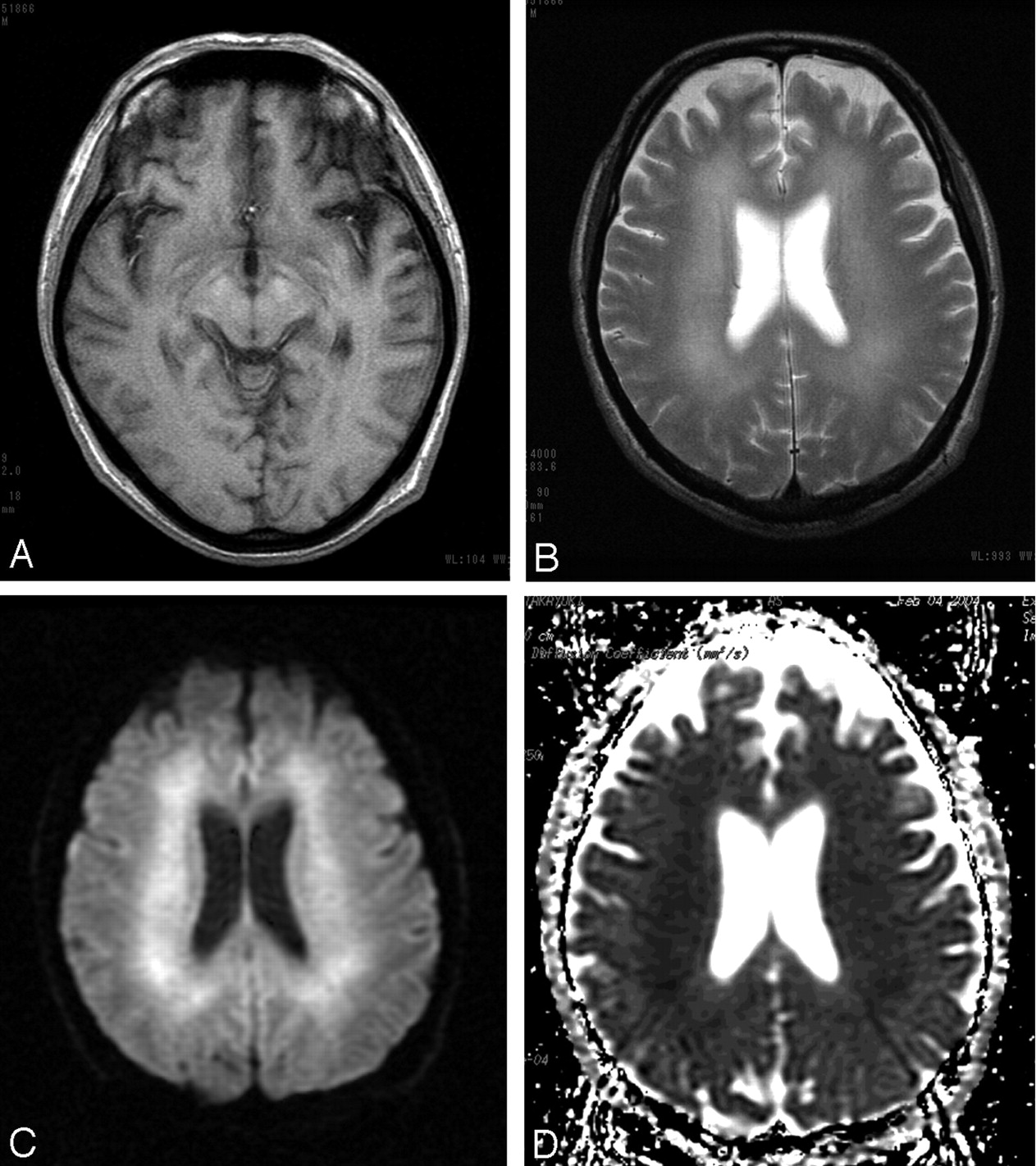
Follow-up MR imaging was performed 2 months after exposure to carbon monoxide. T1-weighted images revealed slightly high-signal-intensity lesions in the pars reticulata of the bilateral substantia nigra (Fig 3A). T2-weighted images showed diffuse high-signal-intensity lesions in the bilateral periventricular deep white matter (Fig 3B). Diffusion-weighted images showed diffuse high-signal-intensity lesions in the bilateral periventricular deep white matter (Fig 3C). Corresponding ADC maps showed low signal intensity in the periventricular deep white matter (Fig 3D). The ADC values of the hypointense deep white matter and isointense subcortical white matter were 0.58–0.69 × 10−3mm2/s and 0.78–0.83 × 10−3mm2/s, respectively. In addition, the symmetrical lesions in the bilateral globi pallidi showed low signal intensity on T1-weighted images and markedly high signal intensity on T2-weighted images. On ADC maps, the signal intensity of the pallidal lesions was increased. The ADC value of the right globus pallidus was 2.1 × 10−3mm2/s. The patient’s symptoms gradually improved, although mild Parkinsonian symptoms with slight dysarthria persisted at the 6-month follow-up examination.

T1-weighted image obtained 2 months after exposure to carbon monoxide (A) shows slightly high-signal-intensity lesions in the bilateral substantia nigra. T2-weighted image (B) shows confluent high-signal-intensity lesions in the bilateral periventricular deep white matter. Diffusion-weighted image (C) reveals diffuse high-signal-intensity lesions in the bilateral periventricular deep white matter. Corresponding ADC map (D) demonstrates low-signal-intensity in the bilateral periventricular deep white matter.
Discussion
Carbon monoxide intoxication is one of the most common causes of morbidity due to poisoning (8). It may be intentional or accidental, and exposure can be lethal (8). Carbon monoxide crosses the alveolar capillary membrane and binds strongly to heme-containing compounds. The affinity of hemoglobin for carbon monoxide is approximately 250 times as great as its affinity for oxygen (8, 9). Carbon monoxide toxicity appears to result from a combination of tissue hypoxia and direct carbon monoxide–mediated damage at the cellular level (8).
A sharply demarcated area of necrosis is seen in the pars reticulata of the substantia nigra as well as the globus pallidus when the brain is studied at autopsy after carbon monoxide poisoning (3). The globus pallidus and the pars reticulata of the substantia nigra are the brain regions with the highest iron content (3). Carbon monoxide binds directly to heme iron in these two brain regions (3). This direct histotoxicity explains the selective vulnerability of the pallidoreticularis to carbon monoxide poisoning (3).
To the best of our knowledge, Kawanami et al (4) are the only authors to have reported the MR imaging features of the pallidoreticular pattern of brain damage caused by carbon monoxide poisoning. In their case report, MR imaging was performed 1 year after exposure to carbon monoxide (4). T2-weighted MR imaging disclosed high-signal-intensity lesions in the bilateral substantia nigra in the midbrain, in addition to bilateral high-signal-intensity pallidal lesions (4).
Our case demonstrated that involvement of the identical sites in the early stage of pallidoreticular damage could be visualized by using diffusion-weighted imaging. Reduced water diffusivity could be due to early cytotoxic edema resulting in acute tissue necrosis. The increased ADC of pallidal lesions in the subacute stage is likely to represent a series of pathologic changes from cytotoxic edema to vasogenic edema, and destruction of the cell membrane, culminating cell necrosis.
The lesions with decreased ADC in the globus pallidus and substantia nigra shared a slight increase of signal intensity on follow-up T1-weighted images. This increased signal intensity on T1-weighted images may indicate the deposition of hemoglobin degradation products due to previous petechial hemorrhage in the globus pallidus, as described elsewhere (9). An alternative explanation for T1 shortening in the globus pallidus and substantia nigra is a nonhemorrhagic mechanism, such as deposition of fat-laden macrophages, degradation of protein, or presence of free radicals or cellular components of necrotic tissue, as described in cases of ischemic injury in the basal ganglia (10, 11). High T1 signal intensity is likely to represent the sequela of acute necrosis.
Carbon monoxide poisoning can lead to demyelination and destruction of cerebral white matter in the late subacute period (3, 5). A local cytotoxic effect of carbon monoxide along with moderate reduction in blood flow may be responsible for the clinical syndrome of delayed deterioration of neurologic and psychiatric symptoms, including cognitive and personal changes, Parkinsonism, urinary or fecal incontinence, mutism, dementia, and psychosis (2, 5, 6, 8). White matter T2 hyperintensities in the centrum semiovale are reported to be significantly associated with cognitive impairment (2). Although extensive white matter lesions may be related to the delayed onset of neuropsychiatry symptoms, pallidoreticular damage is likely to be partially associated with Parkinsonian symptoms. Further studies are needed to investigate this in detail.
In patients with delayed anoxic encephalopathy of carbon monoxide poisoning, bilateral, confluent, white matter lesions show decreased water diffusivity on diffusion-weighted imaging (5, 6). A decrease in ADC persists much longer than the few days after acute cell necrosis (5, 6). A relatively persistent decrease in ADC might be caused by slowly progressive cytotoxic edema in the white matter demyelination (5, 6). Alternatively, spongiform leukoencephalopathy with vacuole formation might be involved in restricting the mobility of water molecules in the white matter, as seen in heroin poisoning (12, 13).
In conclusion, diffusion-weighted imaging is useful for delineation of the pallidoreticular pattern of early brain damage, as well as evaluation of delayed white matter damage, in carbon monoxide poisoning.
References
- Received August 25, 2004.
- Accepted after revision October 5, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cortical abnormalities on MRI: what a neurologist should know
- The Role of MR Imaging in Assessment of Brain Damage from Carbon Monoxide Poisoning: A Review of the Literature
- Chronic carbon monoxide poisoning resulting in bilateral cataracts and a cystic globus pallidus lesion
- White Matter Damage in Carbon Monoxide Intoxication Assessed in Vivo Using Diffusion Tensor MR Imaging