
Abstract
SUMMARY: We report an unusual case of primary intracranial germinoma involving the sphenoid bone and sinus. To the best of our knowledge, paranasal sinus and bone invasion of primary intracranial germinoma has not been previously reported. Recognition of this rare form of presentation by imaging is important because early radiation and chemotherapy can result in a cure of this neoplasm.
Germinomas, the most frequent intracranial germ cell tumors, are rare tumors of children and young adults. They comprise about 0.5%–3% of all primary central nervous system tumors.1 The most common sites of involvement of intracranial germinomas are the pineal and suprasellar regions,2 but they can also involve other locations, such as the thalamus and basal ganglia.3 Germinomas have a propensity to spread throughout the ventricular system and subarachnoid spaces, and their ability to infiltrate adjacent soft tissue structures has already been demonstrated.4 We present an unusual case of primary intrasellar germinoma that destroyed the bony components of the central skull base and invaded the sphenoid sinus at presentation.
Case Report
A 16-year-old Hispanic boy with a long-standing history of polyuria, polydipsia, delayed puberty, and poor growth and development presented with new-onset diplopia. His physical examination was remarkable for short stature with height and weight less than the fifth percentile for age-matched adolescents. He was Tanner stage I and had signs of sixth nerve palsy. Diabetes insipidus was suspected because of the complaints of polyuria and polydipsia. Serum levels of alpha-fetoprotein (AFP) and human chorionic gonadotropin (βHCG) were undetectable.
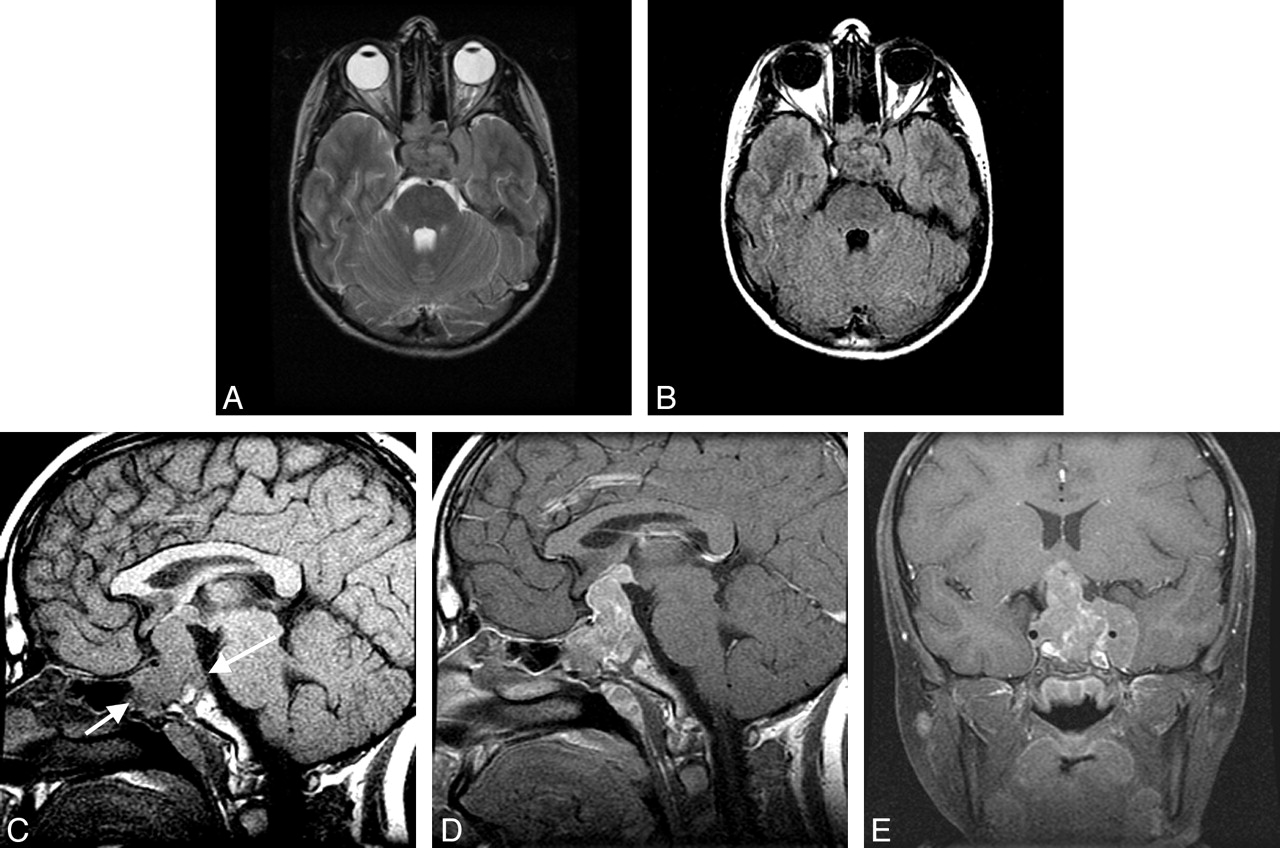
MR imaging of the pituitary revealed a large, solid mass with its epicenter in the sella turcica, extension into the suprasellar cistern and hypothalamus superiorly, sphenoid sinus inferiorly, and cavernous sinuses bilaterally. Total encasement of the left internal carotid artery with mild stenosis and partial encasement of the right internal carotid artery were noted. The optic chiasm and hypothalamus were compressed. The lesion exhibited isointense signal intensity on T2-weighted (Fig 1A), fluid-attenuated inversion recovery (FLAIR; Fig 1B), and T1-weighted images (Fig 1C). It enhanced heterogeneously on contrast enhanced T1-weighted images (Figs 1D, -E). An MR imaging of the spine was normal.

A–D, MR images from 16-year-old boy who presented with a long-standing history of poor growth, delayed puberty, polydipsia, and polyuria.
A, Transverse T2-weighted image at the level of the cavernous sinuses shows an isointense mass involving the sella turcica, posterior sphenoid sinus, left greater than right cavernous sinus, the left middle cranial fossa, and the prepontine cistern.
B, FLAIR-weighted image at the level of the cavernous sinuses shows an isointense mass involving the sella turcica, posterior sphenoid sinus, left greater than right cavernous sinus, the left middle cranial fossa, and the prepontine cistern.
C, Midline sagittal T1-weighted image shows an isointense mass involving the basiocciput portion of the clivus, the sella turcica, the sphenoid sinus (short arrow), and the suprasellar cistern. The expected hypointense posterior cortex is absent (long arrow).
D, Midline sagittal contrast-enhanced T1-weighted image shows a heterogeneously enhancing mass involving the basiocciput portion of the clivus, the sella turcica, the sphenoid sinus, the suprasellar cistern, and the hypothalamus.
E, Coronal contrast-enhanced T1-weighted image at the level of the sella shows a heterogeneously enhancing mass involving the basiocciput portion of the clivus, the sella turcica, the sphenoid sinus, the suprasellar cistern, and the hypothalamus. There is extension into the left greater than the right cavernous sinus with encasement and stenosis of the left internal carotid artery. The typical hypointense cortex of the floor of the sella is not visible. The mass appears to abut the nasopharynx.
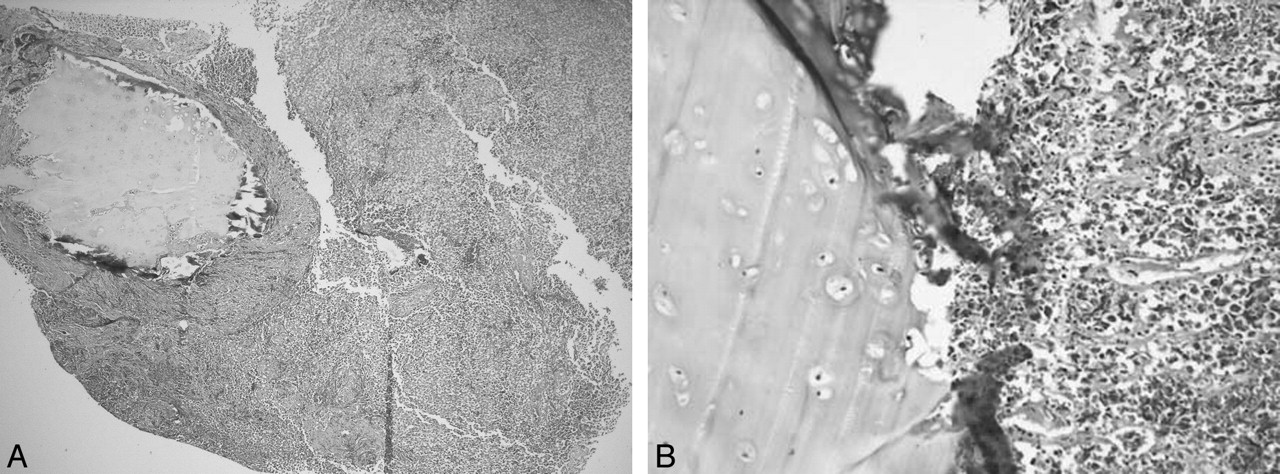
The patient underwent a thorough neurosurgical assessment, and it was concluded that the lesion was not completely resectable. Following hormonal stabilization, decompression surgery was performed via a trans-sphenoidal approach. Specimens from the suprasellar and sphenoid sinus components of the mass, as well as CSF samples, were submitted for histopathologic evaluation. This revealed a highly cellular neoplasm comprising sheets and lobules of polygonal tumor cells traversed by fibrous septae rich in lymphocytes. The tumor cells were characterized by large round nuclei and prominent nucleoli. They wrapped around and invaded bone and cartilage, including the epithelium, and covered sphenoid sinus walls (Figs 2A, -B). The tumor cells showed weak reactivity to placental alkaline phosphatase but were strongly and diffusely reactive for OCT4 nuclear stain, which confirmed the diagnosis of germinoma.5 Immunoreactivity for AFP, β-HCG, epithelial membrane antigen (EMA), cytokeratin, and chromogranin were appropriately absent. A CSF sample collected via lumbar puncture was negative for tumor cells.

A, Low-power image shows sheets of germinoma cells invading and wrapping around the bone and cartilage of the sphenoid process (left upper) (40×, hematoxylin and eosin).
B, High-power image depicts direct invasion of germinoma tumor cells (right side) into adjacent bone and cartilage (200×, hematoxylin and eosin).
The patient was treated with craniospinal irradiation (CSI) with a boost to the tumor bed involving the sella and the sphenoid region. He received 2340 cGy to the craniospinal axis, a boost of 1260 cGy to the ventricles, and an additional 1440 cGy to the sella and the sphenoid area, thereby increasing the tumor bed dose to 5040 cGy. Radiation therapy, delivered during a 6-week period, was well tolerated by the patient. No chemotherapy was administered.
The patient has been closely followed by an ophthalmologist, to monitor for visual field deficiencies, and by an endocrinologist, to monitor for hypopituitarism. He has received desmopressin for treatment of diabetes insipidus. He also receives maintenance doses of corticosteroids and synthyroid for hypocortisolemia and hypothyroidism respectively. Surveillance MR imaging of the brain obtained annually has shown no evidence of recurrence (Figs 3A, -B). The patient continues to receive growth hormone replacement therapy. He has shown adequate growth velocity. At his most recent follow-up visit, 28 months after cessation of radiation therapy, he was without evidence of tumor recurrence and his ophthalmic examination was stable.

A, Midline sagittal T1-weighted image shows no residual mass.
B, Midline sagittal contrast-enhanced T1-weighted image shows no residual mass or pathologic enhancement.
Discussion
Germinomas are thought to arise from a midline streaming of totipotential cells very early in rostral neural tube development or from abnormal implantation in the midline during the migration of germ cells that result in the formation of the urogenital ridge.6 Local spread of intracranial germinoma within the brain and throughout the subarachnoid space,7 including synchronous lesions, is not uncommon. This type of spread, however, is usually limited to the soft tissues within the cranial cavity showing little or no propensity toward bone invasion. Primary intrasellar germinomas are rare.8 They may develop as secondary intrasellar extension of primary suprasellar tumors9 or originate as primitive intrasellar growth. A germinoma may be designated as primary intrasellar if the lesion exclusively resides within the sella turcica or if both intrasellar and extrasellar components are present.10,11 In advanced stages, however, the site of origin cannot be differentiated and tumor may traverse the hypophyseal-hypothalamic axis (HHA). The epicenter of the germinoma in our patient was in the sella turcica (Fig 1); hence, it is classified as a primary intrasellar germinoma. The patient’s long-standing history of signs and symptoms of panhypopituitarism, which is atypical for HHA lesions, supports the primary intrasellar origin of this germinoma.
Our case is unique in demonstrating direct invasion and destruction of the sphenoid bone and basiocciput, which are the major components of the central skull base. Furthermore, overt invasion of the floor of the sella with extension into the sphenoid sinus has not been previously reported. This patient had no complaints of paranasal sinus symptoms, though, like other patients with cavernous sinus invasion and HHA lesions, he had symptoms of both visual disturbance and diabetes insipidus.10–14 The isointense signal intensity on MR imaging, contrast enhancement,2 extension along the HHA8,10,13 and into the cavernous sinuses are typical10 of HHA germinomas. This case clearly demonstrates that germinomas may present as central skull base lesions and therefore should be included in the differential diagnosis. The presence of bone destruction with extension into the adjacent paranasal sinuses, though rare, should not dissuade the radiologist from suggesting the diagnosis of primary intracranial germinoma in the appropriate clinical setting.
CSF dissemination of primary intracranial germinoma throughout the ventricular system and subarachnoid space is common4,7; therefore, before any surgical intervention, MR imaging of the entire spine with contrast is essential for the detection of metastasis.7,15
Surgery is required for histologic confirmation of the diagnosis, and no attempt to achieve total resection is usually made, because germinomas are exquisitely sensitive to radiation and chemotherapy.16 The patient presented here responded well to CSI, which has long been regarded as the conventional therapy for intracranial germinomas. There is, however, an increasing trend toward use of the combined approach of adjuvant chemotherapy and radiation in an effort to reduce the dose and/or field of radiation and ultimately decrease the late effects of radiation therapy in young, developing patients.16
Conclusions
Although histologic sampling is necessary for definitive diagnosis, we propose that primary intracranial germinoma should be considered in the differential diagnosis of central skull base lesions in children or young adults, especially those presenting with signs of pituitary dysfunction and diabetes insipidus. Recognition of this rare form of presentation by imaging is important because early radiation and/or chemotherapy can result in a cure of an otherwise locally destructive neoplasm.
Footnotes
This study was presented, in part, at the 2004 scientific assembly and annual meeting of the American Society of Head and Neck Radiology, Philadelphia, Pa, September 29–October 3, 2004.
References
- Received February 11, 2005.
- Accepted after revision May 9, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.