
Abstract
SUMMARY: We report a case of a 17-month-old child affected by Sturge-Weber syndrome who had unusually rapid overgrowth of the left frontal, temporal, orbital, and maxillary regions. CT angiography illustrated osteohypertrophy with periostitis and associated soft tissue hypertrophy directly corresponding to the distribution of the cutaneous port-wine stain. Extended maxillectomy was performed because of rapid growth and clinical debilitation, with surgical pathology revealing juvenile ossifying fibroma.
Osseous and soft tissue hypertrophy can accompany various soft tissue vascular malformations. In Sturge-Weber syndrome (SWS) where there is cutaneous capillary angioma involving the maxillofacial distribution, there are a few reported cases of associated osteohypertrophy. This osteohypertrophy has been described as angiodysplasia, and “angiodysplastic syndrome” implies a vascular malformation that is associated with secondary changes including further vascular abnormalities, soft tissue and bone hypertrophy, which is more frequently encountered in Klippel-Trenaunay-Weber (KTW) syndrome involving the extremities.1 In the context of this case we define osteohypertrophy as a benign overgrowth of bone. We distinguish osteohypertrophy from a bone neoplasm that has a biologic potential of local recurrence and locally destructive growth pattern or metastasis (WHO classification of tumors). Here we describe the imaging features, differential diagnosis, and histologic findings of a case of SWS in a child with port-wine stain who had a rapid ipsilateral oromaxillofacial osseous overgrowth requiring surgical resection.
Case Report
A 17-month-old boy had a left port-wine stain affecting V1 and V2 distribution, ipsilateral congenital glaucoma, and initial onset of tonic-clonic seizures at 9 months of age. He presented with a 4-month history of rapidly enlarging left face and maxilla, with complaints of drooling, malocclusion, inability to eat solid foods, failure to thrive, and difficulty breathing at night. CT angiography (CTA) was performed for evaluation of possible underlying vascular malformation as the cause of apparent craniofacial deformity.
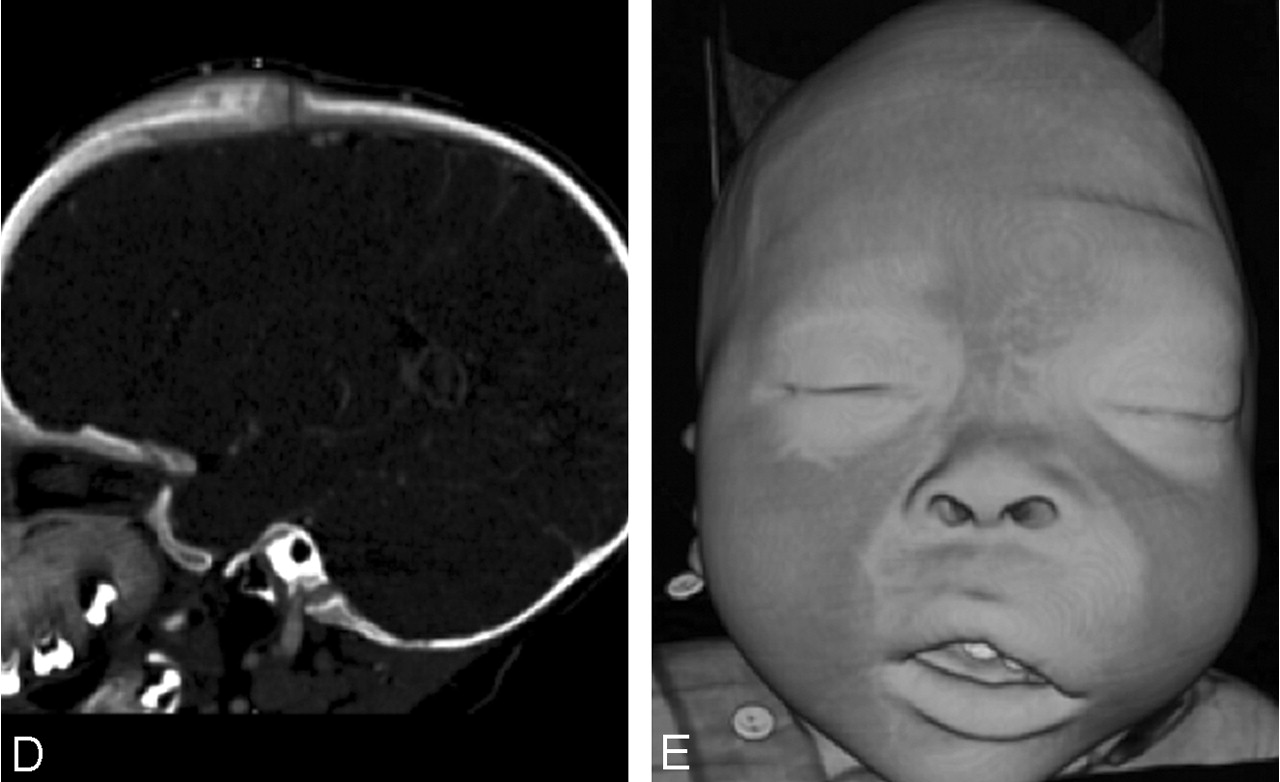
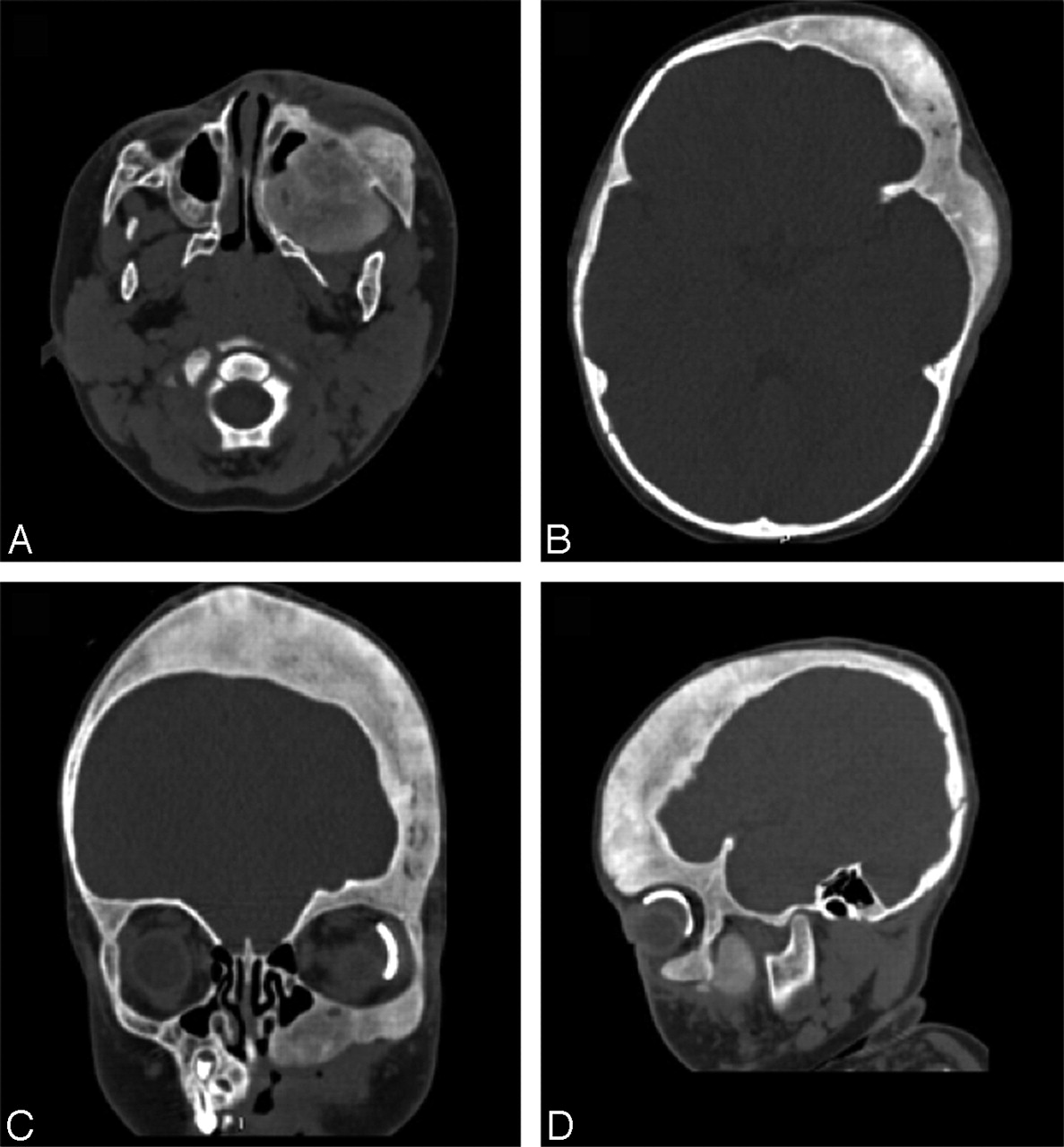
CTA showed facial asymmetry with marked osseous expansion and periostitis affecting the left frontal and temporal skull, zygoma, orbital rims, and maxilla (Fig 1). Asymmetric, premature fusion of the left coronal suture could be seen. There was mild hypertrophy of the overlying soft tissue, in addition to hypertrophy of the hard and soft palate causing airway narrowing and deviation to the right side. On the 3D surface-rendered images, it was apparent that osteohypertrophy conformed to the distribution of the cutaneous capillary angioma (Fig 2).


Axial (A–C) and reformatted sagittal (D) images from CTA obtained after intravenous injection of 1 mL/kg of Omnipaque 350 showing osseous expansion and periosteal elevation involving the left maxilla, orbital rim, and left frontal-temporal skull. Note a left orbit prosthetic device from previous surgery for congenital glaucoma. Prominent focal meningeal enhancement is noted beneath the left frontal calvaria (C), and there is narrowing of the left coronal suture (D). These changes cause oromaxillofacial asymmetry depicted on the surface-rendered 3D image (E).

Surface-rendered 3D images in vascular algorithm (by using a 3D image workstation Vitrea II, Vital Imaging) demonstrate capillary blush in the left vertex crossing the midline, left temporal-parietal skull, periorbital, and maxillary regions corresponding to the known facial port-wine stain (V1 and V2 distribution), as well as sites of osseous hypertrophy.
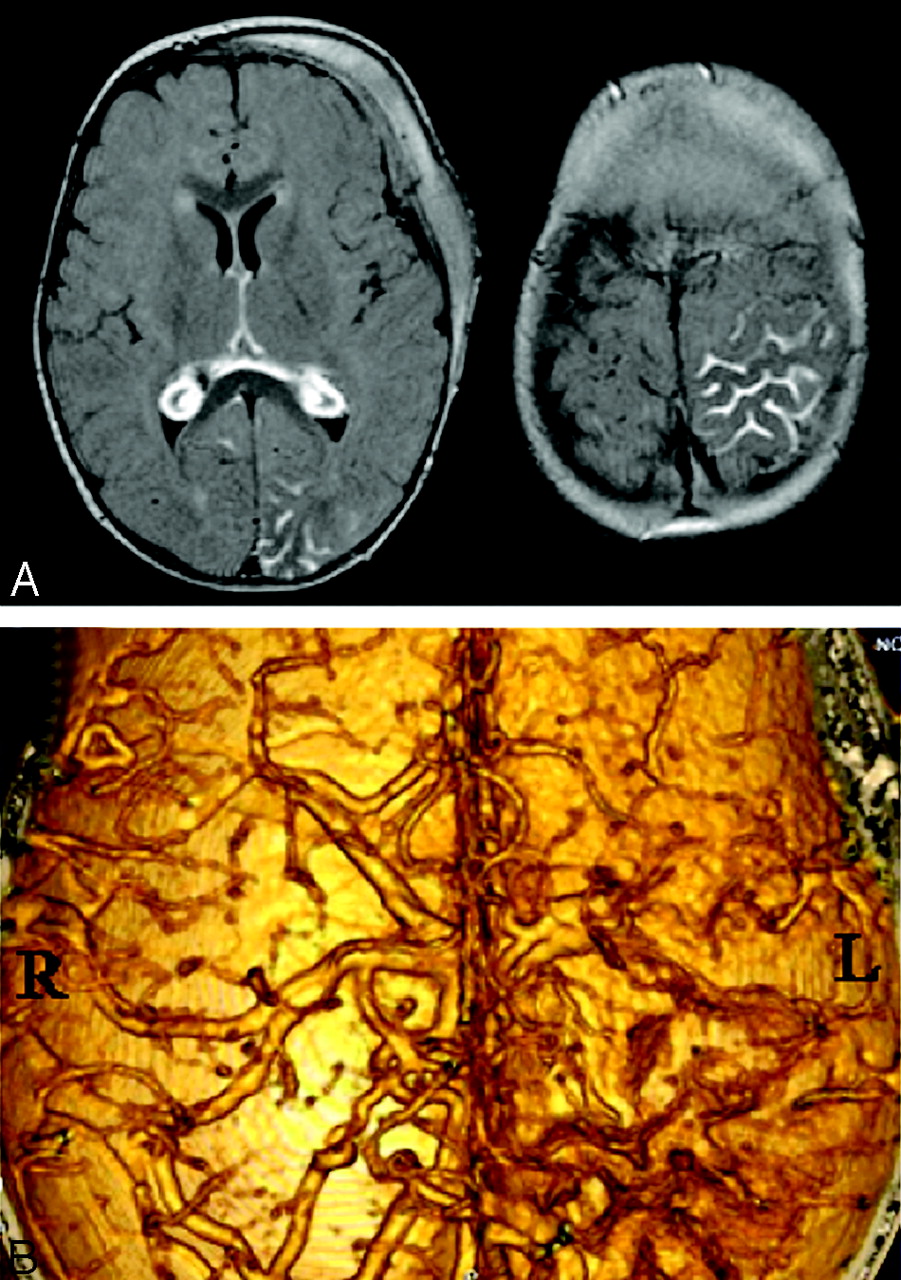
Intracranially the child had mild volume loss and leptomeningeal angiomatosis in the left occipital and parietal lobes that was best illustrated on contrast-enhanced MR imaging (Fig 3A; contrast-enhanced CT findings in Figs 1B, -C). CTA 3D surface rendering (Fig 3B) depicted dysplastic venous structures predominantly along the surface of the left parietal lobe.

A, Axial contrast-enhanced FLAIR (TR/TE/TI, 8802/133/2200) images show leptomeningeal enhancement in the left parietal and occipital regions, and bilateral choroid glomus. B, Surface-rendered 3D image of the interior of the skull depicts dysplastic, irregular vascular structures over the surface of the left cerebrum most prominent in the parietal regions. This is in sharp contrast to a normal appearance of the cortical veins on the right side.
On the basis of clinical and radiologic assessments, an agreement could not be reached on the neoplastic versus angiodysplastic nature of the osseous abnormality. Biopsy of bone from the maxilla and left temporal skull revealed histologic features consistent with a juvenile ossifying fibroma. Because of the aggressive course of its development and the debilitating effects, the boy underwent extended maxillectomy with en bloc resection of the roof of the left hard palate, followed by reconstruction. His airway and feeding issues, as well as his failure to thrive, subsequently resolved, and development to date was appropriate compared with other children of similar age with normal expected milestones.
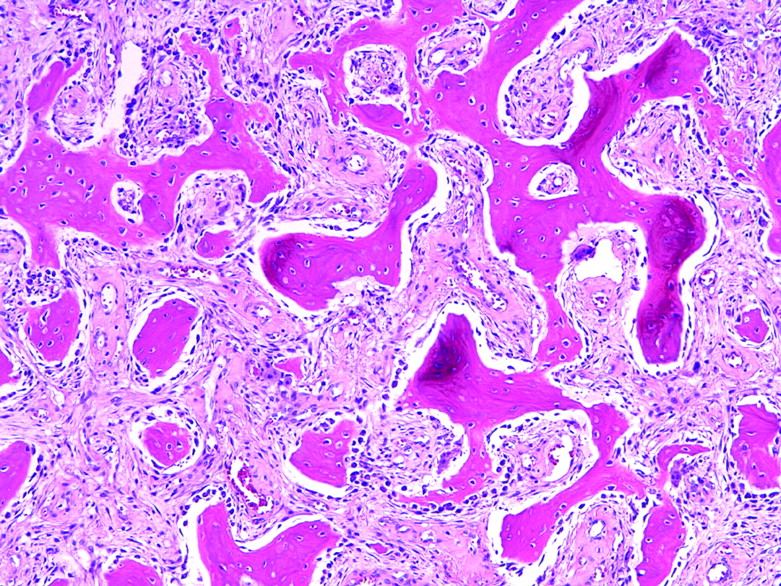
On histologic examination, the lesion had features of a benign bone-forming neoplasm consisting of woven bones in a loose fibrovascular stroma (Fig 4). Bone formation was abundant and uniform. The bone was deposited by plump osteoblasts with occasional osteoclasts. These features were consistent with an ossifying fibroma.

Low-powered photomicrograph (H&E ×20) showing woven bone distributed randomly throughout a fibrovascular stroma.
Follow-up CT examination 8 months later showed a markedly expansile lesion, in the same distribution of the cutaneous capillary malformation, involving the remaining left frontal-temporal skull extending to the orbital rims and maxillary sinus walls that had a typical ground-glass appearance of a fibro-osseous lesion (Fig 5). Bony expansion was more prominent since the initial presentation, though periostitis was no longer present.

Follow-up CTA 8 months after the initial scan and 2 months after surgery shows extended maxillectomy with reconstruction of the left maxillary sinus. There is marked thickening and ground-glass appearance to the remaining left frontal and temporal skull, orbital rim, and maxillary sinus wall. Active periostitis has resolved.
Discussion
SWS is a rare neurocutaneous disorder, thus far mostly considered sporadic occurrence without identified genetic abnormality. It has variable phenotypic expression with common manifestations including port-wine stain, congenital glaucoma, and intracranial leptomeningeal angiomatosis.2 Even though osseous abnormality (hypertrophy, hypoplasia, distortion, lytic destruction, or density changes) has been described for various vascular malformations,3 the incidence of osseous involvement in the cutaneous capillary angioma (or, more correctly, “capillary malformation”) associated with SWS is not known. In their analysis of 224 vascular malformations, Boyd et al3 showed that both in head and neck and, in the extremities, capillary malformations tend to affect size (hypertrophy) alone. In contrast, the other low-flow lesions (venous, lymphatic, or combined malformations) have a high propensity of altering osseous shape as well as size, and high-flow lesions (arterial malformation without or with fistula) may in addition cause destructive change and altered bone mineral density.
In SWS, one of the prevalent radiologic findings is thickening of the skull cap.4 In our experience it is common to see in SWS an asymmetrically smaller hemicranium and, in as many as 50% of cases, mild osseous hypertrophy involving the entire or part of the calvaria ipsilateral to port-wine stain and at times accompanied by increased intraosseous enhancement; however, this pattern of bony changes appears to be rather different from the current case, in which there was profound bony expansion, aggressive periostitis, and rapid progression. This more frequently observed mild bony overgrowth in SWS is most likely a compensatory changes in response to underlying brain parenchymal atrophy rather than related to cutaneous capillary angioma.
In the literature, there is a report5 of a very similar pattern to the current case of oromaxillofacial osteohypertrophy in a patient with SWS; thus, a presumed “angiodysplasia” as a direct association between the syndrome itself and clinical findings, but no pathologic corroboration was available. Another case report6 with pathologic correlation describes fibrovascular tissue within the expanded marrow stroma. More fre-quently reported are incidences of gingival hyperplasia in SWS that may be a cause of dental loosening and disease.6–9 Very similar manifestations of marked maxillofacial angiodysplasia have been described at a greater frequency in patients with KTW syndrome,10,11 which is characterized by cutaneous capillary malformation similar to that in SWS, venous varicosity, and underlying soft tissue and bony hypertrophy and not infrequently occurring in conjunction with SWS with some overlapping manifestations.12 It has also been suggested that SWS and KTW may represent different manifestations of the same pathologic entity.6,13
Even though a vascular malformation–induced osseous change is a strong consideration by virtue of close association with the distribution of capillary angioma in this case and others reported in the literature, the underlying mechanism may be varied and remains elusive at this time. Boyd et al3 suggested possible mechanisms including mechanical, physiologic, and developmental processes that could account for the alteration of skeletal growth pattern in various vascular malformations. Physiologic consideration would suggest that alternation of hemodynamic and metabolic properties adjacent to or within the bone directly affects bony growth. An intrinsic, congenital mesenchymal defect leading to growth alteration is also a strong consideration and may be supported by the discovery of genetic factors. One also wonders whether the secondary effects of the vascular malformation upon the underlying bone could predispose to mutations and thus neoplastic transformations.
Neoplastic occurrence in the setting of vascular malformation is very rare but has been reported. For example, Fay et al described a case of 3-year-old child with Klippel-Trenaunay syndrome (KTS, also called Klippel-Trenaunay-Weber syndrome) and conjunctival soft tissue mass that was proved on pathology to be an orbital rhabdomyosarcoma.14 This case was worthy of note because it also presented with diagnostic confusion and initially was presumed as an orbital lymphatic malformation on the basis of clinical and radiologic examinations in the context of KTS. There were also reports of malignant transformation of benign hemangioma, including in one case of KTS, following radiation therapy.15,16 Juvenile ossifying fibroma is an uncommon, expansile bone-forming neoplasm within the broad category of fibro-osseous lesions including ossifying fibroma, fibrous dysplasia, and cemento-osseous dysplasia.17–19 On histology, an ossifying fibroma shows a wide variation in the mineralized material made of woven bone, laminar bone, and calcified spheroids that in some areas resembles a fibrous dysplasia and may, in fact, represent a part of continuous pathologic spectrum.19 It has various names, including “juvenile,” “active,” and “aggressive” form of ossifying fibroma, or active fibrous dysplasia,18,20 and is distinguished from other fibro-osseous lesions not by histopathlogic features alone but also by radiologic appearance and clinical presentation such as age at onset and potential behavior. It is most often seen in patients 5–15 years of age,17,21 contains cellular stroma and sometimes increased mitotic activity, and typically demonstrates an invasive, often rapid, growth pattern causing local destruction of bone and a high rate (30%–58%) of recurrence commonly affecting paranasal sinuses, orbital and frontal bones, and maxilla. In our case, the area of involvement was extensive, and it was uniquely interesting in that the involvement followed cutaneous capillary malformation. With initial biopsy samples taken from both maxilla and left temporal skull, and later a larger surgical specimen of maxilla yielding the same histologic appearance, it was presumed that the remaining skull that is contiguous with the resected portion also represented juvenile ossifying fibroma. Alternatively, the sampled regions (particularly the maxillary lesion) contained neoplastic growth that was within a larger area of vascular-induced osseous dysplasia morphologically similar to fibro-osseous lesions. The latter is an intriguing possibility, because it has been noted that juvenile ossifying fibroma has a tendency of local recurrence if not resected completely yet may also be induced by a dysplastic process in bone metabolism.22
The current case presented a clinical dilemma at the time of the boy’s presentation because of the uncertainty of diagnosis and aggressive course of osseous hypertrophy. On the basis of the location of osseous abnormality and territory of cutaneous capillary angioma, one may presume a benign etiology related to vascular effect (angiodysplasia) rather than neoplastic growth. The degree of periostitis and rate of osseous expansion, however, was concerning for an aggressive primary osseous neoplasm. Because of progressive cosmetic and functional deformity, after 6 months of observation a decision was made to excise the maxillary lesion. Pathologic specimen confirmed a neoplastic lesion—juvenile ossifying fibroma. Although a vascular effect on bone proliferation was originally considered in light of the clinical context of SWS, the rapid local progression of the mass led one to question this diagnosis in favor of a bone tumor. It remains uncertain, however, whether this represents a coincidental osseous neoplasm or an associated fibro-osseous neoplastic transformation related to cutaneous vascular malformation.
References
- Received January 12, 2005.
- Accepted after revision May 9, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}