
Abstract
BACKGROUND AND PURPOSE: The association of cervical carotid artery bifurcation calcification to future stroke risk is unknown, though coronary artery calcification is a proven indicator of heart disease risk. Severity of white matter change has been correlated with future stroke risk. We sought to use white matter severity grade on CT as a surrogate predictor of relative future stroke risk and thus correlate white matter and future stroke risk with carotid calcification grade.
METHODS: We retrospectively reviewed unenhanced neck and brain CTs in 209 patients. Carotid calcification degree was scored by the Agatston method, adapted from that commonly used to quantify coronary artery calcification. White matter change severity was scored by the European Task Force for Age-Related White Matter Change scale. Both scores were measured blinded to each other, and to age and sex covariables. Association was tested by univariate and multivariate analyses.
RESULTS: Both carotid calcification and white matter scores were strongly, and independently, associated with increasing age (r = 0.61, P < .001; and r = 0.67, P < .001, respectively). Despite apparent association between carotid calcification and white matter scores on univariate analysis, there was no independent effect evident after adjusting for age as a covariant (r = 0.07, P = .14). Sex had no independent effect on white matter scores, though men had a marginally higher mean calcified carotid plaque load than women after controlling for age (P = .008).
CONCLUSIONS: Carotid calcification scores do not independently predict severity of white matter ischemia. Future stroke risk, assessed by white matter severity scores, cannot be predicted from carotid calcium scores.
Calcification of carotid artery bifurcation plaque is common, without established relationship to future stroke risk; however, calcification of the coronary arteries is a well-established marker of significant cardiovascular disease. The coronary artery calcium score, a measure of calcium burden, is now identified as an independent predictor of coronary heart disease events.1 Atherosclerosis of the cervical carotid artery bifurcation is a major cause of stroke and transient ischemic attack (TIA). Plaques typically form in the common carotid artery and extend distally into the internal carotid artery. The cervical carotid artery bifurcation provides a site at which progression of atherosclerosis can be monitored reproducibly and noninvasively. Although certain measures of carotid artery atherosclerosis—including carotid artery stenosis, intimal medial thickness, and carotid plaque burden—are identified factors for future stroke risk,2–4 the predictive value of carotid artery calcification is unknown.
Both CT5–7 and, more recently, MR imaging8–10–based studies have shown that white matter disease severity is an important predictor of future stroke risk, independent of traditional stroke risk factors. Because this was a retrospective study, we used white matter severity as a surrogate marker for future stroke risk. The purpose of our study was to quantify cervical carotid artery bifurcation calcification by using multidetector-row CT and determine its relationship to white matter disease severity assessed on CT. We quantified carotid calcification in unenhanced arteries, allowing optimal detection of smaller plaques of calcium that would otherwise be obscured if contrast CT angiography studies were analyzed. We also used a new rating scale for white matter disease assessment that appears applicable to both CT and MR imaging.11 By investigating the association between carotid artery bifurcation calcification and white matter disease, we hoped to determine whether the carotid calcium score could act as a predictor of future stroke risk, analogous to the way coronary artery calcium score predicts future heart disease risk. Babiarz et al adopted a similar rationale to investigate the association between cavernous carotid artery calcification and white matter ischemia.12 We hypothesized that the carotid calcium score would correlate with high white matter scores and could thus be used as a marker of relative stroke risk.
Subjects and Methods
We retrospectively reviewed the unenhanced neck and brain CTs of 209 patients for cervical carotid artery bifurcation calcification and white matter changes. Our cohort consisted of subjects older than 40 years of age who underwent unenhanced CT imaging of the brain and neck performed at the same sitting. There are few indications for performing simultaneous unenhanced CT brain and neck examinations in routine practice. Therefore, we examined the CT images of trauma patients, because this patient group regularly undergoes noncontrast CT head and cervical examinations for injury assessment. With so many multitraumas being imaged at our institution, patients without necessarily any clinical suspicion of head and cervical spine injury are studied, and these patients formed the bulk of the studied cohort. We excluded patients from the study if the CT quality was inadequate or showed evidence of intracranial injury and if they had any acute neurologic deficits on admission or were followed-up for questionable traumatic brain injury. Any patients with other possible sources of white matter hypoattenuation on a chart review—such as multiple sclerosis, acute disseminated encephalomyelitis (ADEM), vasculitis, or connective tissue diseases—were also excluded. Between August 2003 and September 2004, 209 patients met these criteria through our major trauma center and were included in the study. Demographic details, including age and sex, were recorded.
Imaging was performed on a 4-channel multidetector-row CT (LightSpeed, GE Medical Systems, Milwaukee, Wis). The CT neck protocol included helical scan mode, 2.5-mm section thickness, 1.25-mm image reconstruction, 7.5-mm rotation, 0.75 pitch factor, 90-mA tube current, and 120-kV tube voltage. CT head imaging was performed in the sequential scan mode with 2–5 mm section thickness for the posterior fossa and 5-mm section thickness above the tentorium.
CT images of the brain were analyzed with the reviewers blinded to the subjects’ demographic details and calcium scores. CT images of the neck were analyzed with the reviewer blinded to the subjects’ demographic details and white matter score. The unit of analysis in this study was the hemispheric white matter score and corresponding ipsilateral carotid calcium score; accordingly, 418 carotid-hemisphere units were analyzed. Two experienced neuroradiologists (N.F.F. and S.P.S.) quantified white matter scores and differences were resolved by consensus. One neuroradiologist (N.F.F.) quantified carotid calcification scores; this neuroradiologist had received specific training in the Agatston method for quantifying calcium load, which is a more analytic method than the white matter visual analog scale.
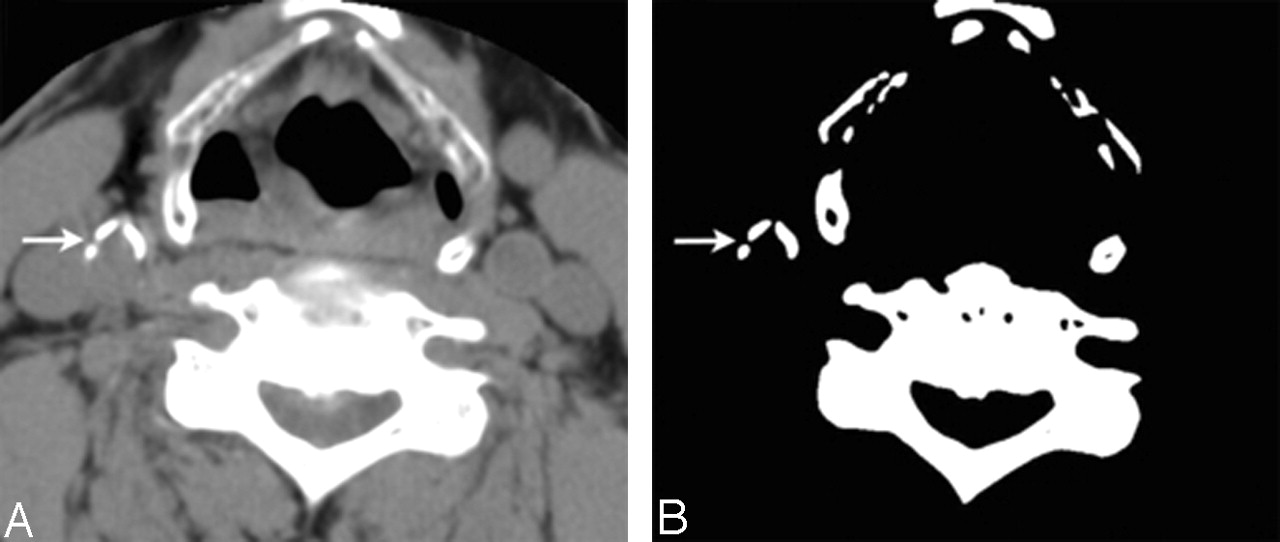
Calcium score was evaluated by the Agatston method13 on an independent workstation (Advantage Windows 4.1, GE Medical Systems). A calcified plaque was defined as a radiation-attenuating structure with an attenuation above a threshold of 130 Hounsfield units (HU) in an area ≥1 mm2. Carotid bulb calcium plaques were identified in a soft tissue window (width 340 HU, center 43 HU), and a narrow viewing window (width, 1 HU; center, 130 HU; Fig 1). For quantification, the region-of-interest function was used to measure the area and peak attenuation of the calcified plaques. A score for each calcified plaque was obtained by multiplying the plaque area by a weighted peak attenuation score (weighted peak attenuation is the product of peak attenuation and a cofactor of 1–4: cofactor 1, 130–199 HU; cofactor 2, 200–299 HU; cofactor 3, 300–399 HU; cofactor 4, ≥400 HU). The total calcium score represents the sum of all single calcium plaque scores at the cervical carotid artery bifurcation (common and internal carotid arteries). Scores for both right and left carotid arteries were recorded. Carotid artery calcium scores were also divided into 4 severity grades (none: calcium score = 0; minimal–mild: 1–100; moderate: 101–400; severe: ≥400 Agatston units) on the basis of coronary artery calcium data.14

Axial CT at level of thyroid cartilage shown on soft tissue window (width, 340 HU; center, 43 HU) in panel A and narrow window (width, 1 HU; center, 130 HU) in panel B. Three calcific plaques are seen at the right distal common carotid artery (arrow).
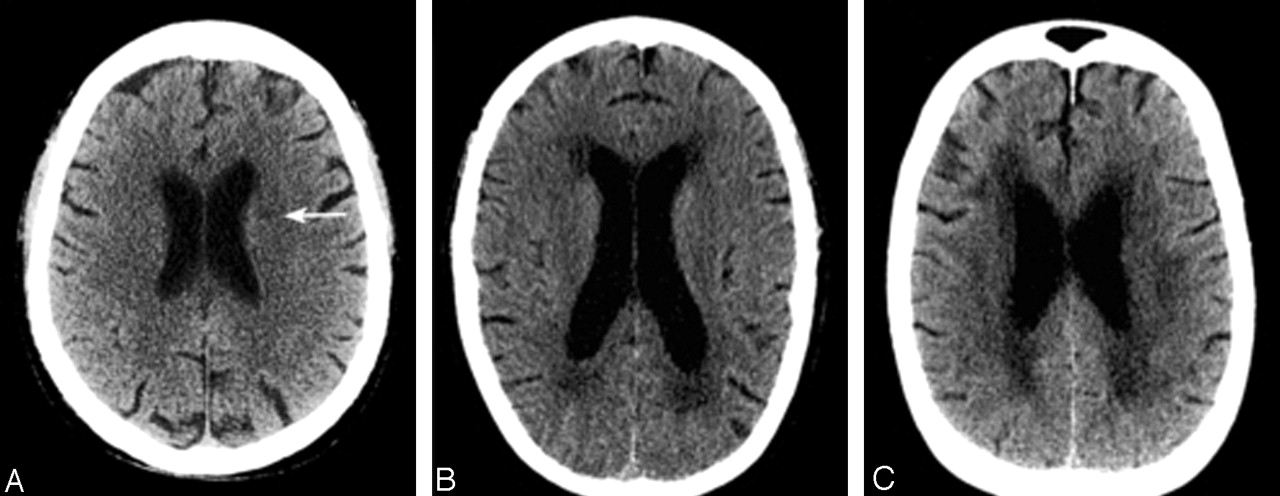
For white matter assessment, analysis was performed on a digital image workstation (Impax version 4.5; Agfa-Gevart, Mortsel, Belgium). We used a visual scale for white matter severity change based on the European Task Force on Age-Related White Matter Changes,11 which has been shown to correlate pathologically with severity of ischemic tissue damage.11, 15 A 4-point grading scale was used as follows: 0 (no lesions); 1 (focal lesions >5 mm); 2 (early confluent lesions); and 3 (diffuse involvement of an entire brain region). Five brain regions are used for rating: frontal, parieto-occipital, temporal, infratentorial, and basal ganglia. Examples of the grading system are given in Fig 2. For each patient, the highest score for each hemisphere was used in the analysis. As an aside, only 8 MR imaging brain and 7 CT angiogram studies were performed in this cohort, with no discordant MR brain findings compared with CT and no carotid dissections (data not shown).

Examples of the white matter rating scores by using the European Task Force on Age-Related White Matter Changes, from 3 separate study cases. Score 1 (A): focal ill-defined hypoattenuation in the left corona radiate (arrow); score 2 (B): beginning confluence of lesions; score 3 (C): diffuse involvement of the frontal and parieto-occipital region seen in this example.
Statistics
Univariate and multivariate analyses were used to examine for evidence of association between carotid artery calcium score and the severity of white matter changes. χ2 test with Yates’ correction was used to investigate associations with between dichotomous variables (carotid calcium score ≤100 or >100 and white matter score of ≤1 or >1). Inter- and intraobserver agreement was by Cohen’s weighted kappa statistic for ordinal categorical data (white matter scores) and intraclass correlation coefficient for continuous variables (carotid calcium scores). For white matter disease severity, 40 hemispheres were read twice by each reader. For the one reader who quantified carotid calcium scores, 40 carotid arteries were read twice. Statistical significance was established at P < .05. The statistical packages SPSS 11.0 (SPSS Inc., Chicago, Ill) and Analyze-It (Analyze-It Software, Ltd., Leeds U.K.) were used for analysis.
Results
Both carotid calcification and white matter scores were strongly, and independently, associated with increasing age (log10 carotid calcium score r = 0.61, P < .001; and white matter score r = 0.67, P < .001). Summaries of the white matter disease severity scores and carotid artery calcification scores are given in Tables 1 and 2, respectively; correlation values for calcium and white matter scores are detailed in Table 3. The prevalence of any carotid artery calcification was 38.5%, and any white matter disease was 48.8%.
Summary of white matter disease severity scores
Summary of carotid artery calcium scores
Pearson correlation scores
There was an apparent association between carotid calcification and white matter scores on univariate analysis (r = 0.45, P < .001 [Table 3]). χ2 test of the relationship between a total carotid calcium score of >100 (moderate or severe disease) and a white matter score of >1 (early confluent and confluent disease) showed that these 2 characteristics appeared significantly related (P < .001; odds ratio, 4.5; 95% confidence interval, 2.8–7.3). All of these effects were mediated by age, however, and there was no independent effect evident after adjusting for age as a covariant (white matter grade and log10 total calcium score with age adjustment; r = 0.07, P = .14). Sex had no independent effect on white matter scores, though men had a marginally higher mean calcified carotid plaque load than women after controlling for age (mean calcium plaque load of 185.8 Agatston units for men vs 96.3 Agatston units for women; P = .008). Sex had no effect on correlation of age and white matter scores or of age and carotid calcium score.
Inter- and intraobserver agreement correlation values for white matter grades were excellent (weighted kappa values of 0.93 and 0.94, respectively). For the one reader who quantified carotid calcium scores, there was excellent intraobserver correlation (intraclass correlation of 0.99).
Discussion
Ischemic cerebrovascular disease is the second leading cause of mortality in most developed countries. Therefore, factors associated with this disease are important to identify. The validity of quantifying extracranial carotid atherosclerosis as a marker of stroke risk is borne out by several large population studies. Risk of stroke has been correlated with specific measures of carotid atherosclerosis, including intimal medial thickness, plaque load and composition, and percent stenosis.2–4 Because calcification is a widely used indicator of atherosclerosis, there has been increased interest in CT quantification of calcification as a noninvasive measure of atherosclerotic load, with an increasing trend of screening for calcification in the carotid as well as coronary arteries. The accuracy of CT in quantifying calcification has been validated by a number of experimental studies on ex vivo carotid endarterectomy specimens and pathologic studies in the coronary arteries.16–18 Although sonography is the most common screening method for quantifying carotid atherosclerosis (measuring intimal medial thickness, plaque composition, and percent stenosis), sonography is less accurate than unenhanced CT in quantifying carotid artery calcium.17
The major limitation of our study was that it was not a prospective longitudinal study using stroke as an end point. To assess stroke risk, we used white matter disease severity as a valid surrogate marker. Data from the 5 major prospective population-based studies that investigated white matter severity and incident stroke rate are reviewed in Table 4. The association between white matter severity, ischemic stroke risk, and subtype of ischemic stroke risk (large-vessel thromboembolic strokes and small-vessel “lacunar” infarcts caused by occlusion of small perforating arteries) can be summarized by the following points: (1) The main predisposing factors for white matter change are age, arterial hypertension, and other risk factors for stroke.19, 20 (2) Stroke patients frequently have established white matter changes on baseline CT, with a reported incidence as high as 44%.21 Although all stroke subtypes may be associated with these established white matter changes, the strongest association is for small-vessel disease.21 (3) White matter changes increase over time both in stroke and asymptomatic patients.5, 22 (4) Prospective follow-up of stroke patients with and without white matter disease has shown that white matter changes are associated with an increased risk of stroke recurrence (multivariable adjusted hazard ratio 1.5–1.6).5, 7 In the Dutch TIA Trial, this increased risk was from large as well as small vessels, with a similar frequency of stroke subtypes in patients with and without white matter disease.7 The NASCET group found a slightly higher incidence of lacunar strokes in patients who developed white matter disease on follow-up compared with patients who did not (29% vs 21%; P = .45), which suggests that white matter development in stroke patients may be more closely related to small vessel disease; however, large artery stroke was the largest subtype of ischemic strokes in both groups (66% vs 73%).5 (5) In asymptomatic patients with no stroke history, white matter changes are associated with an increased risk of stroke (multivariable adjusted hazard ratio 3.0–4.7).8–10 Only one study assessed relative frequency of ischemic stroke subtypes, and found unexpected predominance of cardioembolic strokes (27%), compared with lacunar (15%) or atherosclerotic (5%) strokes; however, the data may be limited, because 47% of ischemic stroke subtypes were unknown.8
Prospective population-based cohort studies of white matter-lesion severity and incident stroke
Overall, these studies have shown that white matter changes are an established risk factor for all types of future stroke. The unexpected predominance of large-artery strokes on follow-up remains to be explained. The association between white matter changes and future stroke is probably not a direct causal one. Diffuse demyelination of the white matter is strongly associated with, and probably caused by, atherosclerosis. The white matter changes may reflect a more advanced stage of generalized atherosclerosis. Bots et al have shown that white matter lesions are associated with significantly greater cardiac, peripheral arterial, and carotid artery atherosclerosis.23
We have shown that the carotid bifurcation calcium CT score could not predict the extent of white matter disease once age was controlled for, and hence could not predict relative stroke risk. Similarly, Babiarz et al, found no association between cavernous carotid calcification and white matter ischemic severity after adjusting for age as a covariable.12 An earlier study showed that total (intimal and medial) carotid calcification of the horizontal cavernous segment was not associated with alterations in cerebral blood flow.24 Why do calcium scores predict future heart disease in the coronary circulation and not stroke risk in the cerebral circulation? The relationship between calcification and atherosclerosis appears to differ in various arteries. Coronary artery calcium scores are highly correlated with coronary plaque load.18 In the carotid circulation, Arad et al found no meaningful association between carotid calcium score and intimal medial thickness, a valid measure of plaque load,25 whereas a further report showed an apparent association (r = 0.45), but this was attenuated and weak (r = 0.25) after adjusting for age as a covariable.26 Thus, it appears that the tendency to deposit calcium per given amount of plaque varies among different arteries. In the coronary circulation the amount of calcium is correlated to the total atherosclerotic plaque burden and, consequently, to the likelihood of one or more vulnerable plaques being present somewhere in the coronary artery system.27 Although the presence of coronary calcium may not indicate vulnerability of a particular plaque, it may be useful to detect vulnerable cardiac patients.28,29 Carotid artery calcium load does not accurately reflect carotid atherosclerotic burden. In addition, unenhanced carotid CT cannot easily assess the extent of the noncalcific plaque or the relative plaque composition. It is the relative composition of carotid plaques that appears important in assessing carotid plaque stability, because most studies suggest that symptomatic carotid plaques are more likely to be ulcerated, less organized, and hemorrhagic,30–33 whereas calcified plaques are associated with fewer symptoms of stroke and TIA.34–36 Thus, it appears that carotid calcium plaque load reflects neither overall atherosclerotic plaque load nor relative plaque composition and instability.
This study correlated white matter disease extent with a single plaque component, calcification, and suggests that the future risk of stroke is not related to extent of plaque calcification. Atherosclerotic plaque composition and volume can now be determined by MR imaging,37, 38 and these emerging MR imaging techniques may prove to be a more accurate predictor of stroke risk than CT quantification of calcium plaque load.
Conclusion
Our results show no correlation between carotid CT calcium scores and white matter disease severity when age is included as a covariant; assessment of future stroke risk by white matter grade cannot be predicted from the carotid calcium score. From these data, there is no support for routine screening for carotid artery calcification for predicting stroke risk. A longitudinal study by using stroke as the primary outcome measure, rather than white matter severity scores, would be useful to confirm the findings of this study.
Footnotes
Presented at the 43rd annual meeting of the American Society for Neuroradiology, Toronto, Ontario, Canada, May 21–27, 2005.
References
- Received March 7, 2005.
- Accepted after revision June 21, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Correlation between carotid bifurcation calcium burden on non-enhanced CT and percentage stenosis, as confirmed by digital subtraction angiography
- Calcification in Major Vessel Beds Relates to Vascular Brain Disease
- The Relation of Carotid Calcium Volume with Carotid Artery Stenosis in Symptomatic Patients
- Carotid Artery Wall Thickness and Leukoaraiosis: Preliminary Results Using Multidetector Row CT Angiography
- Authors' response