
Abstract
PURPOSE: To explore the role of single-photon emission CT (SPECT) in initial diagnostic evaluation of patients with mild traumatic brain injury (MTBI) and to identify subgroups in which it may serve as a useful diagnostic tool.
MATERIALS AND METHODS: Patients with MTBI seen during a 14-month period were prospectively included in this study. All patients had a CT of head within 12 hours of injury and SPECT by using technetium Tc99m ethyl cysteinate dimer (Tc99m-ECD) within 72 hours of injury. Both SPECT and CT findings were compared with clinical features such as posttraumatic amnesia (PTA), postconcussion syndrome (PCS), and loss of consciousness (LOC).
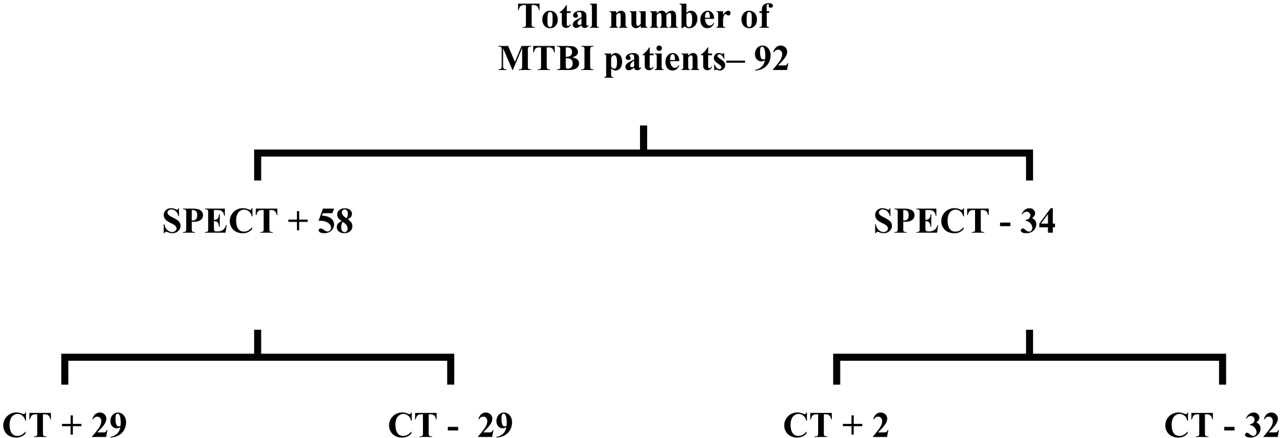
RESULTS: Ninety-two patients with MTBI underwent SPECT in the study period. There were 28 children and 64 adults, with male-to-female ratio of 4.5 to 1. CT findings were abnormal in 31 (34%) and SPECT in 58 (63%). The most common abnormality was hypoperfusion in the frontal lobe(s) in adults and the temporal lobe in children. A significantly higher number of perfusion abnormalities were seen in patients with PTA (P = .03), LOC (P = .02), and PCS (P = .01) than in patients without these symptoms. Compared to CT, SPECT had a much higher sensitivity for detecting an organic basis in these subgroup, of patients (P < .05).
CONCLUSION: Tc99m-ECD SPECT can be used as a complementary technique to CT in initial evaluation of patients with MTBI. It is particularly useful in patients having PCS, LOC, or PTA with normal CT scan.
Brain injury is a common cause of morbidity and mortality in all age groups and represents a major public health problem with high annual cost.1 The mortality rate due to brain injury at the global level is estimated to be 97/100,000 population per year.2 In India, it is the seventh-leading cause of mortality contributing to 11% of total deaths; 78% of cases are due to road traffic injuries alone.3 Mild brain injury has been consensually defined by the Mild Traumatic Brain Injury (MTBI) Committee of the brain injury interdisciplinary special interest group of the American Congress of Rehabilitation Medicine as:
Loss of consciousness (LOC) not exceeding 30 minutes.
After 30 minutes, an initial Glasgow Coma Score (GCS) of 13–15 is observed.
Posttraumatic amnesia (PTA) not exceeding 24 hours.
The definition includes patients with direct head trauma as well as those who suffer an acceleration/deceleration injury (“whiplash”) without specific direct head trauma.4 In one of the recent studies in patients with brain injury in India, it was observed that severe, moderate, and mild brain injuries constituted 16%, 14%, and 70% of cases, respectively. It is surprising that only 24.3% patients with “mild” brain injury showed good recovery, 74.3% showed moderate recovery, and 1.4% died. As many as 10% of the patients with mild brain injuries needed continuous and long-term supportive care. A disturbing fact is that the productive 20–29-year-old age group is the most commonly affected.5
Historically, the options for evaluation in MTBI have included skull radiography, CT, MR imaging, and inpatient observation. Various newer modalities such as cerebral perfusion studies, brain stem–evoked potential, and serum markers are presently being evaluated for the diagnosis, characterization, and prognostication of MTBI.6 Although single-photon emission CT (SPECT) has shown promise in evaluation of MTBI, most of the reported studies were retrospective, involved a small number of patients, and SPECT was done more than 1 week postinjury,7 thus negating its usefulness as an initial diagnostic tool. We therefore decided to study prospectively the role of SPECT within 72 hours of injury.
Another objective of this study was to attempt to correlate SPECT findings with common clinical symptoms such as postconcussion syndrome (PCS), PTA, and LOC, which can be present in these patients.
Materials and Methods
This was a prospective study carried out during a 14-month period (November 2001 to December 2002). One hundred twenty patients with MTBI underwent SPECT during this period. Patients were included if they had fulfilled the criteria of MTBI as described above. In accordance with our hospital policy, patients with even MTBI have to be admitted for 24 hours for observation. We therefore offer admission to all such patients. Informed consent was obtained from all the patients enrolled into the study. Patients with past history of head injury or any known neurologic disease were excluded from the study. Ninety-two consecutive patients who fulfilled our inclusion and exclusion criteria were analyzed in the study. All the patients had CT within 12 hours of injury and SPECT within 72 hours of injury.
Detailed history and demographic information was noted in all patients. This included age, sex, duration of MTBI, presence of symptoms of PCS, and presence of other disease with particular reference to the nervous system. Patients who presented with symptoms suggestive of PCS were reviewed by a neurosurgeon 1-week postinjury for further management and re-evaluation.
CT Scan.
A noncontrast CT was done on a Picker 2000 scanner with 8-mm sections in all patients. The presence of any contusion(s), hematomas, or subarachnoid blood was considered as an abnormal finding.
SPECT.
SPECT was performed in all patients in a silent, dimly lit room with eyes open and ears unplugged, 45 minutes after intravenous injection of 555–925 MBq (15–25 mCi) 99mTc-ECD (BARC, Mumbai). For patients less than 18 years of age the dose was calculated based on the patient’s weight (10 MBq /kg). Acquisition was done on a dual-headed rotating scintillation gamma camera (Elscint, Varicam) with the patient supine, headrest attached, smallest permissible radius of rotation, 128 × 128 matrix, 360°, 120 projections, 25 seconds per projection by using either low-energy ultrahigh-resolution fan beam collimator or a low-energy high-resolution parallel hole collimator.
Raw data were smoothed with Butterworth filtered Nyquist of 1.404 cycles/cm and cutoff frequency of 0.56. Chang attenuation correction was applied. Images were then reoriented in axial, coronal, and sagittal planes. Final data were displayed on a computer monitor and analyzed by using 10-graded color scale. The cerebellum was used as reference site (100% maximum value). Any decrease in cerebral perfusion in the cortex or basal ganglia <70% or <50% in the medial temporal lobe compared with the cerebellum was considered abnormal. This method has been described elsewhere.8
The studies were analyzed independently by 2 experienced nuclear physicians who were blinded to the patients’ clinical symptoms as well as the CT findings. Only if there was concordance between them was the study considered positive. SPECT data were then compared with the CT scan and clinical findings by the neurosurgeons.
There is normal variation of the radiotracer uptake pattern on SPECT throughout the entire brain, which depends on the radiopharmaceutical used. We therefore carried out SPECT by using Tc99m- ECD on healthy subjects to further validate our results. Brain SPECT was performed on 40 healthy volunteers to develop an institutional normal data base. There were 30 men and 10 women, ranging in age from 18 to 65 years. None of these patients showed any abnormality with the criteria used above. The consensus rate between 2 observers for SPECT study of normal controls was 100%. For the patients with MTBI, the consensus rate was 93%.
Statistical Analysis.
Pearson χ2 statistic was used to compare SPECT and CT findings in patients who had PTA, LOC, or symptoms of PCS, with patients who did not have these symptoms. McNemar test was used to compare the SPECT and CT findings within each of these groups separately. A χ2 test for trend analysis was carried out to examine whether positive SPECT and CT findings were related to duration since head injury and GCS.
Results
There were 64 adults and 28 children (less than 18 years of age). Twenty of the 28 children were less than 10 years. There were 75 male and 17 female patients, with a male-to-female ratio of 4.5 to 1. Ages ranged from 2 years to 72 years. (27.6 ± 17.5 years). Twelve patients had GCSs of 13, 25 patients had GCSs of 14, and remaining 55 patients had GCSs of 15 at presentation. Thirty patients had SPECT within 24 hours, 26 patients within 24–48 hours, and the remaining 36 patients within 48–72 hours. The cause of trauma was road traffic accident in 69 (75%) patients, domestic accidents such as falls in 14 (15.2%) patients, and direct blunt injury in 9 (9.8%) patients.
The main symptom was pain at the site of injury that was present in all the patients, followed by headache in 57 patients (62%), nausea and vomiting in 39 patients (42.4%), PTA in 30 patients (32.6%), sleep disorders in 25 patients (27.2%), dizziness in 23 patients (25%), and anxiety in 15 patients (16%). Transient LOC lasting less than 30 minutes was seen in 51 patients. Because the percentage of patients displaying symptoms of PCS drops drastically in the first week postinjury,9 patients were re-evaluated clinically in department of neurosurgery 1 week after injury to observe whether the symptoms persisted. The ICD-10 criterion was used for PCS.10 By use of these criteria, the symptoms of PCS lasted in 26 patients even 1-week postinjury.
SPECT showed perfusion abnormalities characterized by decreased uptake of the radiotracer Tc99m-ECD in 58 (63%) patients. CT findings were abnormal in just 31 (34%) patients (Figs 1 and 2). Of the 28 children, CT findings were abnormal in 7 (25%), whereas SPECT findings were abnormal in 15 (53.5%) patients. Of the 64 adult patients, CT findings were abnormal in 24 (37.5%) and SPECT findings were abnormal in 43 (67.2%). The frontal lobe was commonly affected in adults, whereas the temporal lobe was most commonly involved in children (Table 1).

Comparison of SPECT and CT in patients with mild traumatic brain injury.

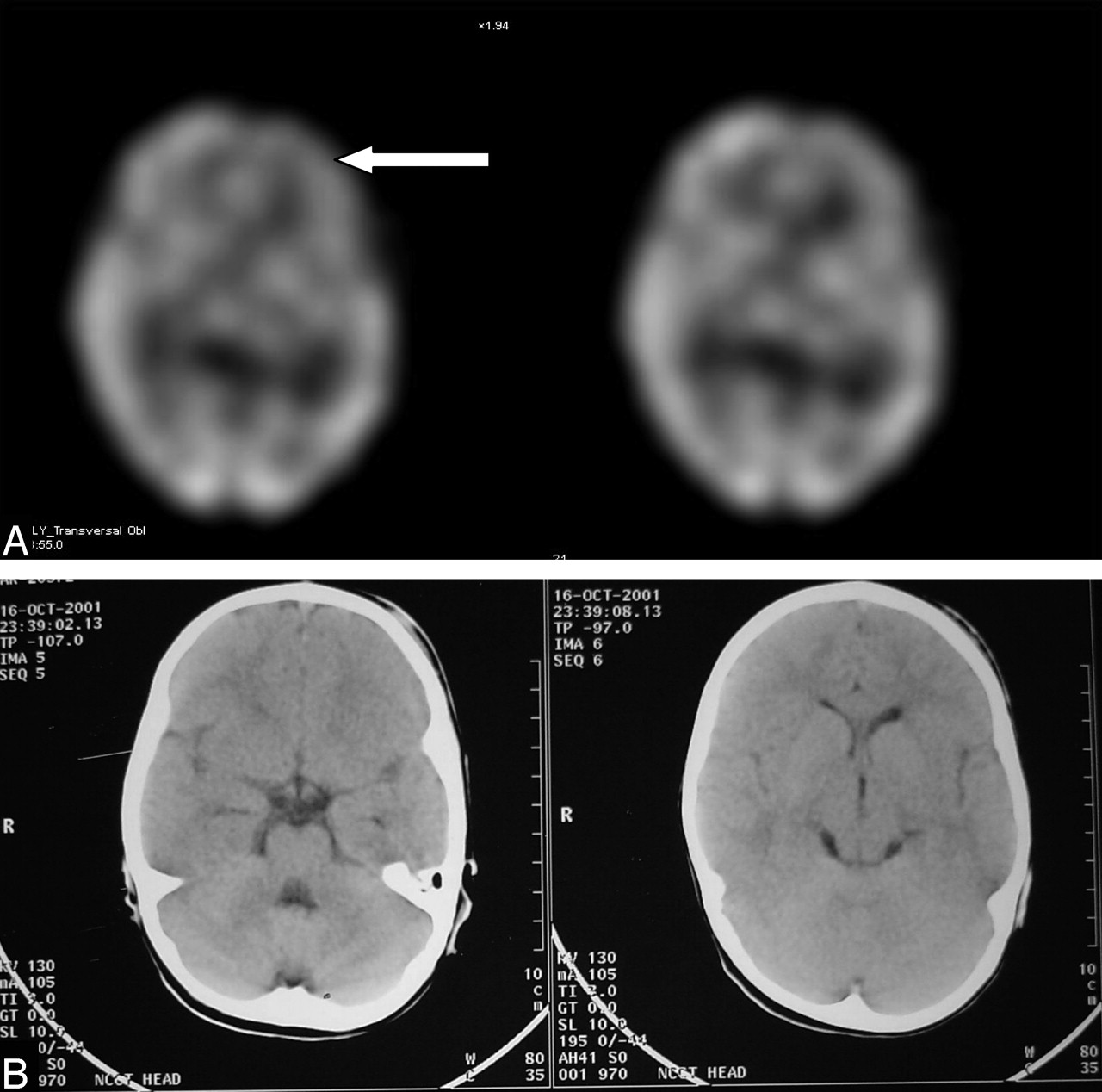
SPECT (A) showing hypoperfusion in left frontal lobe in an 8-year-old male patient with normal plain head CT (B).
Distributions of brain lesions seen in SPECT following MTBI
CT showed epidural hematoma in 7 patients, hemorrhagic contusion in 25, and subarachnoid hemorrhage in 3 patients. In all the patients with epidural hematoma and hemorrhagic contusion, SPECT showed an area of hypoperfusion corresponding to a lesion seen in CT. SPECT also showed hypoperfusion in sites that appeared normal in CT. SPECT was normal in 2 of the 3 patients who had subarachnoid hemorrhage.
A significantly higher number of perfusion abnormalities were seen in patients with PTA (P = .03), LOC (P = .02), and PCS (P = .01) compared with patients without these symptoms. On comparing with CT, SPECT had a much higher sensitivity for detecting an organic basis in these subgroups of patients (P < .05; Table 2).
Comparison of SPECT and CT findings in patients with PTA, LOC, and PCS
There was a significant association between SPECT and CT positive findings with GCS at presentation (P < .05). No similar association was found, however, when SPECT and CT findings were compared with duration of head injury (Tables 3 and 4).
Number of patients showing SPECT- and CT-positive findings compared to duration of injury
Number of patients showing SPECT- and CT-positive findings compared to GCS
Discussion
“No head injury is too trivial to ignore” (Hippocrates, 460–377 BC, in Ingebrigsten)11
Head trauma has been one of the major causes of morbidity and mortality in all ages. The incidence is particularly high in the productive age group.1 Although accounting for more than 70% cases of head injury, MTBI has lacked attention by neurosurgeons and neurologists alike. The situation, fortunately, has improved dramatically in recent years, and the long-term effects of concussion are now being recognized so much so that MTBI is now considered a silent epidemic.5 Of all the imaging modalities, CT has revolutionized the management of head injury and is considered the investigation of choice.6, 12 It can be easily performed, is less expensive, and bony injuries and hematomas are better visualized.13 On the other hand, studies comparing CT with MR imaging have shown that CT can be relatively insensitive and that MR imaging is more sensitive than CT particularly for nonhemorrhagic lesions.14, 15 MR imaging, however has its own limitations, mainly due to the expenses involved, associated motion artifacts in agitated patients, and the deterioration in image quality in the presence of ferromagnetic monitoring equipment.16 Even if one manages to overcome these limitations, not all lesions following MTBI may be detected.17 Although positron-emission tomography provides information on cerebral metabolism and has shown promise in MTBI,12 it is not widely available, not regularly reimbursed, and is more expensive than SPECT. The discovery of significant changes in relative cerebral blood flow (rCBF) in patients with MTBI by various researchers18–20 makes SPECT a promising tool in evaluating patients with MTBI. Previous studies have shown that SPECT may be a viable technique in evaluating MTBI.8, 21, 22 Most of these studies, however, are retrospective by design8, 20 or involve small study populations.17, 20
In their prospective study, Jacobs et al evaluated 136 patients with MTBI,22 who underwent initial SPECT within 4 weeks after trauma. The patients were followed at 3, 6, and 12 months after injury. They concluded that normal SPECT findings are a reliable tool to exclude clinical sequelae of mild injury. Also at 12 months postinjury, a positive SPECT study is also a reliable predictor for clinical outcome.23 It has been suggested that, the earlier the SPECT is done after MTBI, the greater the number of lesions that will be detected.8 In our study, SPECT demonstrated perfusion abnormalities in 63% patients, whereas CT showed brain parenchymal lesions in only 34% of patients. This confirms earlier studies, which have shown that SPECT is more sensitive than CT in detecting underperfused areas of the brain in MTBI.8, 23–29 Lesions were mainly localized to the frontal and temporal lobes followed by the basal ganglia and thalamus. Similar results were seen by Abdel-Dayem et al.8 Frontal and temporal lobes are commonly affected in head injury mainly due to the gliding effect of the brain over the underlying skull.6 All patients in our study had hypoperfusion in the affected regions. Although this hypoperfusion is generally attributed to the cerebral edema that surrounds the damaged brain and limits cerebral blood flow,20 it may also result from vasospasm, direct vascular injury, and perfusion changes due to alterations in remote neuronal activity (diaschisis).17, 27, 28 There is evidence to show that the brain is more vulnerable to ischemic injury after minor head injury, and it has been hypothesized that SPECT findings representing hypoperfusion may in fact lead to secondary ischemic injury.17
In patients showing lesions on CT, hypoperfusion on SPECT corresponded to the CT lesions, and in most of the cases hypoperfused lesions were much larger than the lesions seen on CT. In some of these patients SPECT showed hypoperfusion in regions that appeared normal on CT. In 29 patients with normal CT, SPECT demonstrated areas of hypoperfusion. This may be due to relative changes in the rCBF not detected by CT. Similar findings have been observed in other studies as well.8, 21, 23 Two of the patients had positive CT findings but negative SPECT findings. Both had subarachnoid hemorrhages. The possible reasons are due to the poorer resolution of SPECT and the absence of significant cerebral blood flow changes in the underlying brain in these patients.8
Some authors have observed hyperperfusion with Tc99m HMPAO SPECT in regions corresponding to the CT lesions.7 We did not observe hyperperfusion in any case, and this could be because of the use of Tc99m-ECD in all cases. Hyperperfusion is generally reported in moderate to severe brain injury patients, in whom there may be dissociation between cerebral blood flow and reduced metabolic demand in the lesions.7 Tc99m-ECD shows predominant cellular-metabolic uptake, and hexamethyl propylene amineoxine (HMPAO) reflects blood flow arrival to cerebral regions.30 This accounts for the slight differences in the SPECT perfusion patterns. For cerebral perfusion-metabolic uncoupling, increased HMPAO uptake may occur, thus reflecting the luxury perfusion phenomenon whereas ECD uptake remains low, reflecting hypometabolism at the site of ischemia. Image interpretation is therefore more straightforward with ECD. Moreover image quality obtained by using ECD is relatively better than images obtained with HMPAO.30
When comparing SPECT and CT findings with the presenting complaints such as LOC, PTA, and the symptoms associated with PCS, SPECT was found to be more sensitive in detecting brain lesions in all the groups. SPECT positivity was greater in patients having these symptoms compared with patients without these symptoms. In the 37 patients who showed LOC and normal CT findings, SPECT was positive in 16 patients (43.2%). In patients with PTA and normal CT (n = 17), SPECT was positive in 12 patients (70.1%). Similar findings have been reported by Lorberboym et al.31 SPECT was positive in 84.6% of patients showing PCS and the findings are similar to the study by Kant et al.32 Unlike previous studies in which frontal lobe lesions were most common, however, we found temporal lobes to be most commonly involved in patients having PCS. Ten of the 28(35.7%) children showed PCS, whereas 16 of 64 adults (25%) had PCS 1 week following injury. Of these 26 patients, SPECT was abnormal in 22 (84.6%) and revealed temporal hypoperfusion in 18 (69.2%), frontal hypoperfusion in 12 (46.2%), and hypoperfusion in the basal ganglia and thalamic regions in 12 (46.2%; Table 2).
Previous studies have suggested that a significant proportion of children admitted with MTBI may have moderate disability at follow-up.33 In a recently published study, posttraumatic symptoms in children did not correlate with somatic, neurologic, or electroencephalographic findings observed immediately after the injury or at the follow-up investigation after 6 weeks.34 Our study shows that SPECT with its higher sensitivity may therefore help in predicting persistent post-traumatic symptoms in children with MTBI. Our data also support the contention that functional brain imaging with SPECT could be a useful investigational tool in patients having PTA, LOC, or PCS, particularly in patients who have normal anatomic imaging.
In the absence of a gold standard to detect brain lesions following MTBI, however, one cannot calculate the exact sensitivity and specificity of SPECT and CT. Nevertheless, with the available data, we can conclude that SPECT is much more sensitive in detecting lesions than CT. There was a significant increase in the number of brain lesions detected by SPECT as the GCS decreased from 15 to 13 (Table 4), reiterating the importance of GCS in evaluation of MTBI; however, no similar association was found when SPECT findings were compared with duration of head injury. This disparity could be because relatively less symptomatic patients were imaged within the initial 48 hours and discharged from hospital, whereas more symptomatic patients were imaged on the third day and were observed for longer duration.
A meta-analysis by the World Health Organization has suggested that financial compensation was a strong risk factor for long-term disability, symptoms, and objective findings after MTBI.35 SPECT being more sensitive can be useful in solving legal aspects in MTBI better than CT by ruling out any underlying brain lesion in a symptomatic case. According to the current standard of practice, the treatment of patients with MTBI with a normal head CT is purely based on symptoms, irrespective of SPECT findings. We believe that this mode of management should be reassessed and investigated based on the findings of our study. Serial SPECT imaging may possibly serve as a platform to test the efficacy of various drugs and neurobehavioral interventions in symptomatic patients with MTBI.
Conclusions
SPECT, with better sensitivity for detection of cerebral perfusion abnormalities, can complement CT in initial diagnostic evaluation of abnormal areas of the brain following MTBI. It is particularly useful in patients having PTA, LOC, or PCS with normal anatomic imaging.
References
- Received December 24, 2005.
- Accepted after revision July 7, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging Evidence and Recommendations for Traumatic Brain Injury: Advanced Neuro- and Neurovascular Imaging Techniques
- What evidence exists for new strategies or technologies in the diagnosis of sports concussion and assessment of recovery?
- Forensic Applications of Cerebral Single Photon Emission Computed Tomography in Mild Traumatic Brain Injury