
Abstract
PURPOSE: Carotid artery stent placement may be limited by the embolization of atheromatous material. We evaluated the safety and feasibility of the Medtronic Self-Expanding Carotid Stent (Exponent) in combination with the Medtronic Interceptor Carotid Filter System for the treatment of carotid stenosis among patients at high risk for carotid endarterectomy.
METHODS: Patients at high risk for carotid endarterectomy but amenable to percutaneous treatment with stent placement were enrolled. Clinical follow-up was performed at 30 days and 6 and 12 months postprocedure. The National Institutes of Health Stroke Scale was assessed before and within 3 days postprocedure and at 30 days and 6 months postprocedure. Angiography was performed pre- and postprocedure, and carotid duplex scans were performed at baseline and at 30 days and 6 months.
RESULTS: Fifty-two carotid procedures were performed in 51 patients (mean age, 69 years; 84% of patients were men). The major adverse event (MAE) rate (death, stroke, and myocardial infarction [MI]) at 30 days was 5.9%: 2 strokes and a single death from periprocedural MI. MAE rates after 6 and 12 months were 5.9% and 11.8%, respectively. The delivery success rate was 94.2% (49/52) for the Interceptor Filter System and 95.9% (47/49) for the Exponent Stent. The mean diameter stenosis of the target lesion was reduced from 62.4% preprocedure to 21.2% postprocedure.
CONCLUSION: High delivery success rates were achieved with a low rate of MAE (death, stroke, or MI) in a high-risk population. Treatment of carotid artery disease with the Exponent Carotid Stent combined with distal protection from the Interceptor Filter System is effective and safe.
Carotid endarterectomy (CEA) is a well-established and highly beneficial stroke-prevention treatment for patients with symptomatic severe internal carotid artery (ICA) stenosis.1,2 A significant number of symptomatic patients may not be surgical candidates because of comorbid medical disease or because of local contraindications for surgery, such as previous therapeutic radiation to the neck, previous carotid endarterectomy, challenging anatomy, or other technical reasons. These patients continue to have a high 2-year risk of recurrent stroke.1
Percutaneous transluminal angioplasty and carotid artery stent placement have now emerged as technically viable alternatives to carotid endarterectomy and have been offered especially for nonsurgical candidates. The Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS),3 a randomized multicenter trial comparing CEA with carotid angioplasty (including 26% of patients who underwent carotid artery stent placement as a bailout procedure), demonstrated virtually identical 30-day outcomes for these 2 techniques, though the rates of stroke and death were high, at 10%.4 Patients receiving carotid angioplasty had fewer complications with cranial nerve injury and perioperative myocardial infarction (MI). Case series reports have reported stroke and death rates ranging from 2.6% to 17.8%.5–11 These higher rates contrast with reports from routine stent placement of both asymptomatic and symptomatic patients where periprocedural rates of stroke and death ranged from 3.6% to 7.4%.12–16 A global survey revealed disabling stroke or death rate of only 2.4% for carotid artery stent placement.17
Complications of carotid artery angioplasty and stent placement may be caused by embolization of atheromatous material at the time of stent deployment.18,19 Filter, occlusion balloon, or basket devices placed distal to the carotid artery lesion have been developed to minimize this potential embolic complication. A recent comparison of stent placement with and without embolic protection by using data from published stent placement studies demonstrated substantial decreases in the combined stroke and death rate for patients who underwent stent placement with embolic protection.20 The recently completed SAPPHIRE (Stent Placement and Angioplasty with Protection in Patients at High Risk for Endarterectomy) study, which compared surgery with intervention by using a stent combined with a distal embolic protection device, showed noninferiority for carotid artery stent placement compared with CEA for the composite end point of stroke, MI, or death at 30 days postintervention and for death and ipsilateral stroke between 31 days and 1 year postintervention.21
The MAVErIC (Evaluation of the Medtronic AVE Self-Expanding Carotid Stent System with distal protection In the treatment of Carotid stenosis) International study was designed to assess the feasibility, safety, and efficacy of using a distal protection device, the Medtronic Interceptor Carotid Filter System (Medtronic, Minneapolis, Minn), in combination with the Medtronic Exponent Carotid Stent during carotid artery stent placement in patients at high risk for carotid endarterectomy.
Methods
Patients
All patients admitted for a percutaneous revascularization of the carotid artery were screened for study eligibility. Patients at least 18 years of age with a carotid artery stenosis (≥50% for symptomatic patients or ≥80% for asymptomatic patients) located between the origin of the common carotid artery (CCA) and the intracranial segment of the ICA, who were at high risk for carotid endarterectomy and were amenable to percutaneous treatment with stent placement, were eligible for enrollment. For patients with an eventual nondisabling stroke, the procedure was not performed until at least 4 weeks after the stroke, whereas for those with a transient ischemic attack (TIA)—including amaurosis fugax and central retinal artery occlusion—stent placement without delay was permitted, provided that a recent CT or MR imaging scan showed no recent infarction.
Additional inclusion criteria included a target vessel reference diameter suitable for use with a carotid filter system ranging from 5.5 mm to 6.5 mm, with no angiographic evidence of intraluminal thrombus. Patients also had to be considered high risk for carotid surgery, on the basis of anatomic and medical criteria (Table 1). Exclusion criteria included an intracranial or distally inaccessible stenosis ≥70% in the target carotid artery; previous stent placement of the target vessel; multiple lesions, which would require more than one stent; planned interventional procedure or vascular surgery (peripheral, coronary, or carotid) 30 days before, or 30 days after, the procedure; occlusion of the target carotid artery at the time of angiography; and MI within 72 hours of the index procedure. Patients with a history of bleeding diatheses or coagulopathy or those who refused blood transfusions or had an allergy or contraindication to aspirin, ticlopidine, clopidogrel, nickel, titanium, or a sensitivity to contrast media or had a platelet count <100,000 cells/mm3 or >700,000 cells/mm3 or a white blood cell count of <3000 cells/mm3 were also excluded. In addition, patients who had experienced significant gastrointestinal bleeding within 6 months before the study procedure, had excessive peripheral vascular disease that precluded safe sheath insertion, or had a concurrent embologenic cardiovascular disease that precluded safe sheath insertion or patients who were participating in another investigational drug or device study were also excluded.
Definitions of high-risk patients
All patients provided written informed consent, and the protocol was approved by the institutional review boards or ethical committees of each study center as appropriate.
Medtronic Exponent Carotid Stent and Medtronic Interceptor Filter System
The Medtronic Exponent Self-Expanding Carotid Stent is constructed of a nickel-titanium alloy (Nitinol), which is delivered to the carotid arteries via a 6- or 7F sheathed delivery system. The stent is delivered to the intended lesion site and then expanded by retraction of the protective sheath. The Medtronic Interceptor Carotid Filter System consists of 3 components: a filter/guidewire, a delivery/retrieval sheath, and a handle designed to open, close, and torque the filter. The filter is a basket constructed from a braided nitinol mesh with a pore size of 100 μm, with a low crossing profile (2.9F). The proximal end of the wire filter basket consists of 4 large openings (>1800 μm each), which allow particulate to enter the filter (Fig 1). Retrieval of the filters is performed by using either the retrieval sheath, or an over-the-wire angioplasty balloon, following postdilation of the stent.

The Interceptor distal embolic protection device. A, Closed (0.0039-inch crossing profile). B, Open, showing the 1800-μm proximal openings.
Catheterization Procedure
Antiplatelet therapy was administered according to local routine. The following schedule was, however, recommended (1) acetyl salicylic acid (ASA; minimum 75 mg daily) and ticlopidine (1000 mg loading dose followed by 250 mg BID), or (2) ASA (minimum 75 mg daily) and clopidogrel (300 mg loading dose followed by 75 mg QD), the day of the procedure, depending on the institution’s routine pre-stent medication practice. Whenever possible, ticlopidine or clopidogrel were started the day before the procedure, but no later than the conclusion of the catheterization. Postprocedure, subjects continued to receive ASA (minimum 75 mg daily) plus either ticlopidine 250 mg twice daily or clopidogrel 75 mg daily. Other concomitant medications were to be administered at the physician’s discretion. During the procedure, patients received intravenouns boluses of heparin appropriate to prolong the activated clotting time (≥250–300 seconds with the HemoTec device and 300–350 seconds with the Hemochron device), or ≥200 seconds if an intravenous GPIIb/IIIa-receptor blocker was administered. Thrombolytic agents and/or IIb/IIIa inhibitors were permitted at the discretion of the operating physician in cases of intraluminal thrombus formed during the stent placement procedure.
Vascular access was obtained through canulation of the femoral artery. Selective angiography of the carotid vessel was performed with standard frontal and lateral views and, if needed, in multiple oblique views to best isolate and define the carotid lesion. Baseline stenosis severity was assessed and the reference vessel size at appropriate locations (distal and possibly proximal to the stenosis) was precisely determined to enable selection of the correct size Interceptor filter. The recommendation was for selection of a carotid filter with a diameter 0.5 mm larger than that of the reference vessel.
The Interceptor Filter System (5.5, 6.0, or 6.5 mm in diameter) was positioned distal to the target lesion before predilation. In cases where the filter failed to cross the lesion, mild predilation to allow crossing of the distal protection device was permitted. The Exponent Stent was introduced by using the appropriate size device (available diameters between 6 and 10 mm, available lengths 20, 30, and 40 mm) on the basis of previous quantitative carotid angiographic analysis. Post-stent balloon inflations were permitted to ensure optimal stent apposition and expansion. Positioning and removal of the carotid filter system was documented angiographically. Implantation of the Interceptor carotid filter system and the Exponent Carotid Stent could only be performed by physicians trained in both a “dry” model and in the animal laboratory.
Analysis of Particulate Debris
Filters retrieved from patients were preserved in 10% buffered formalin. Gross observations of each filter were documented and the filters photographed before the removal of particulate for analysis. Particulate analysis was performed by the Biomedical Engineering Center, Harvard-MIT Division of Health Sciences and Technology Massachusetts Institute of Technology using new quantitative methods for particulate characterization as described elsewhere.22,23 Particle size distribution and total relative volume of the captured particulate were calculated by automated imaging techniques. Histologic analysis was performed by using standard hematoxylin-eosin (H&E) and HAM56 staining methods. Six unused sterile Interceptor filters provided comparative baseline negative control data (generated from SECURE particulate analysis by using 4.5-mm filters), and 5 samples of particulate retrieved by using the Medtronic GuardWirePlus were analyzed to provide comparative positive controls.23
Assessments
Angiography was performed both before and after the procedure, and angiograms were analyzed off-line by the centralized independent core laboratory (Heart Core, Leiden, the Netherlands). Quantitative angiography measurements were performed by using the Cardiovascular Measurement System (QVA-CMS, version 5.2; MEDIS Medical Imaging Systems, Leiden, the Netherlands).
Carotid duplex scans were performed within 30 days before the procedure, and at the 30-day and 6-month follow-up visits. Carotid duplex scans were reviewed off-line by the core laboratory. A preprocedural CT/MR imaging scan was optional, whereas postprocedural CT/MR imaging scans were performed on all patients with suspected or documented procedure-related neurologic events. Eventual neurologic treatment was performed according to routine hospital practice.
Clinical and Laboratory Assessments
An electrocardiogram (ECG) was required within 24 hours postprocedure. Cardiac enzymes (CK and CK-MB) were measured within 7 days of the procedure and between 8 and 16 hours postprocedure. In cases of a postprocedural elevation in CK levels, CK and CK-MB were monitored every 8 hours for 24 hours, starting with the first elevation noted.
Clinical Follow-Up
Patients underwent clinical follow-up at 30 days (range, 25–35 days), 6 months (range, 22–32 weeks), and 12 months (range, 48–56 weeks). All patients were evaluated by an independent neurologist for neurologic events by means of the National Institutes of Health stroke scale ≤10 days before the procedure, within 3 days postprocedure, and at the 30-day and 6-month follow-up visits.
Outcome Measures
The primary safety outcome was the incidence of major adverse events (MAEs) at 30 days postprocedure. MAEs were defined as death, MI (Q-wave or non Q-wave), or stroke. The primary efficacy outcomes were the delivery success rates for the Medtronic Interceptor Carotid Filter System and Exponent Carotid Stent.
Statistical Analysis
This was an observational, noncomparative trial. Therefore, the primary statistical analysis was based on descriptive statistical techniques. Data were analyzed on an intent-to-treat basis. In general, all continuous variables were summarized by counts, means, and SDs. All discrete variables are reported as percentages.
Results
Patients
Between November 2001 and December 2002, 51 patients (84% men; mean age, 69 years) were enrolled and underwent carotid stent placement at 11 sites in Europe, Canada, and the Middle East. All had significant comorbid illness (Table 2). Baseline angiographic data were available for 51 procedures. In 46 patients, the target lesion was located in the ICA, while in 5 patients (10%) the target lesion was located in the CCA (Table 3). The percentage diameter stenosis as assessed by the angiography core laboratory decreased from 62.37 ± 10.46% preprocedure to 2.16 ± 13.37% postprocedure. The acute gain was 42.11 ± 14.40 mm. A total of 52 procedures were performed. For one patient, the contralateral carotid artery was treated with the study devices 34 days after the original procedure.
Patient baseline characteristics
Lesion and angiographic characteristics as assessed by core laboratory
Procedural Success Rates
The delivery success rate of the Interceptor filter system was 94.2% (49/52). Three cases were classed as delivery failures. In one case, the insertion of the filter system was complicated because of extreme vessel tortuosity. The investigator attempted twice to insert the guiding catheter and the filter system, but as the patient failed to tolerate the procedure, the procedure was cancelled. In the second case, the filter could not be positioned, because of significant tortuosity of the vessel distal to the lesion. The device was withdrawn and stent implantation was performed without distal protection. In the third case, the investigator decided to use the filter system only during the post-stent deployment dilation part of the procedure. Some damage occurred to the distal wire tip during the introduction of the filter system. Difficulties occurred with getting the filter system to open properly when it was finally positioned distal to the stent. Retrieving the filter through the stent also caused problems. These problems were likely due to improper preparation of the filter system. Predilation before filter insertion was required during 4 procedures (7.7%). In one case this was an elective predilation, and in the other 3 cases it was due to the filter system failing to cross the lesion.
The Medtronic Carotid Stent was used in 50/52 procedures. Two patients did not receive the Medtronic stent. One could not be implanted because the guidewire was too short to use an over-the-wire delivery system, and a carotid Wallstent (Boston Scientific, Natick, Mass) was successfully implanted without a distal protection device. The second patient did not tolerate the procedure and no stent was implanted (described above). In the remaining 50 cases, 2 delivery failures of the carotid stent occurred. One occurred as a result of severe vessel tortuosity. In this case, the guiding catheter lacked sufficient support during introduction of the stent, causing retraction of the filter device. The procedure was successfully continued by using 2 overlapping carotid Wallstents without distal protection. A second delivery failure occurred after the first stent jumped to a point distal to the intended deployment location, and a second overlapping stent was required to cover the lesion. The second Medtronic carotid stent was advanced but could not be deployed, because of a stenosis in the proximal end of the first stent. The stent was removed and not reused. The proximal lesion was dilated with a balloon catheter, and, after several dilations, a third Medtronic carotid stent was introduced and deployed proximal to, and overlapping, the first stent. Stent placement was therefore classed as technically successful in 47/49 patients—a delivery success rate of 95.9%. Fifty-seven stents were used.
The results of the sonography evaluation of the carotid arteries are shown in Fig 2. At 6 months a stenosis of >50% was observed in 20.9% of patients in the proximal ICA, in 19.1% of patients in the distal ICA, and in 2.4% of patients in the CCA.

Percent diameter stenosis in carotid arteries over time, as determined by sonography evaluation (core laboratory analysis). prox, proximal; dist, distal. The following criteria were used for determination of %DS: PSV (peak systolic velocity) ≤ 125 cm/s: <49% DS; PSV > 125 cm/s and EDV (end diastolic velocity) ≤ 140 cm/s: 50%–79% DS; PSV > 125 cm/s and EDV > 140 cm/s: 80%–99% DS; no flow in ICA: 100% DS.
Adverse Events
At 30 days postprocedure, 3 patients (5.9%) had experienced a total of 4 MAEs (Table 4). One patient suffered an MI and died several hours postprocedure, and 2 patients developed ipsilateral stroke. In one case the stroke occurred during the procedure, and in the second case the patient suffered a TIA during the procedure and a stroke 1 day postprocedure. Between 30 days and 6 months postprocedure, one additional patient suffered a stroke. The MAE rate at 6 months was therefore 7.8%. At the 12-month follow-up, 6 patients (11.8%) had experienced a total of 8 MAEs (Table 4). Additional MAEs occurring after the 6-month follow-up included one patient who died as a result of an MI 12 months postprocedure and another patient who suffered an MI 8–9 months postprocedure.
Cumulative incidence of major adverse events
Analysis of Filters
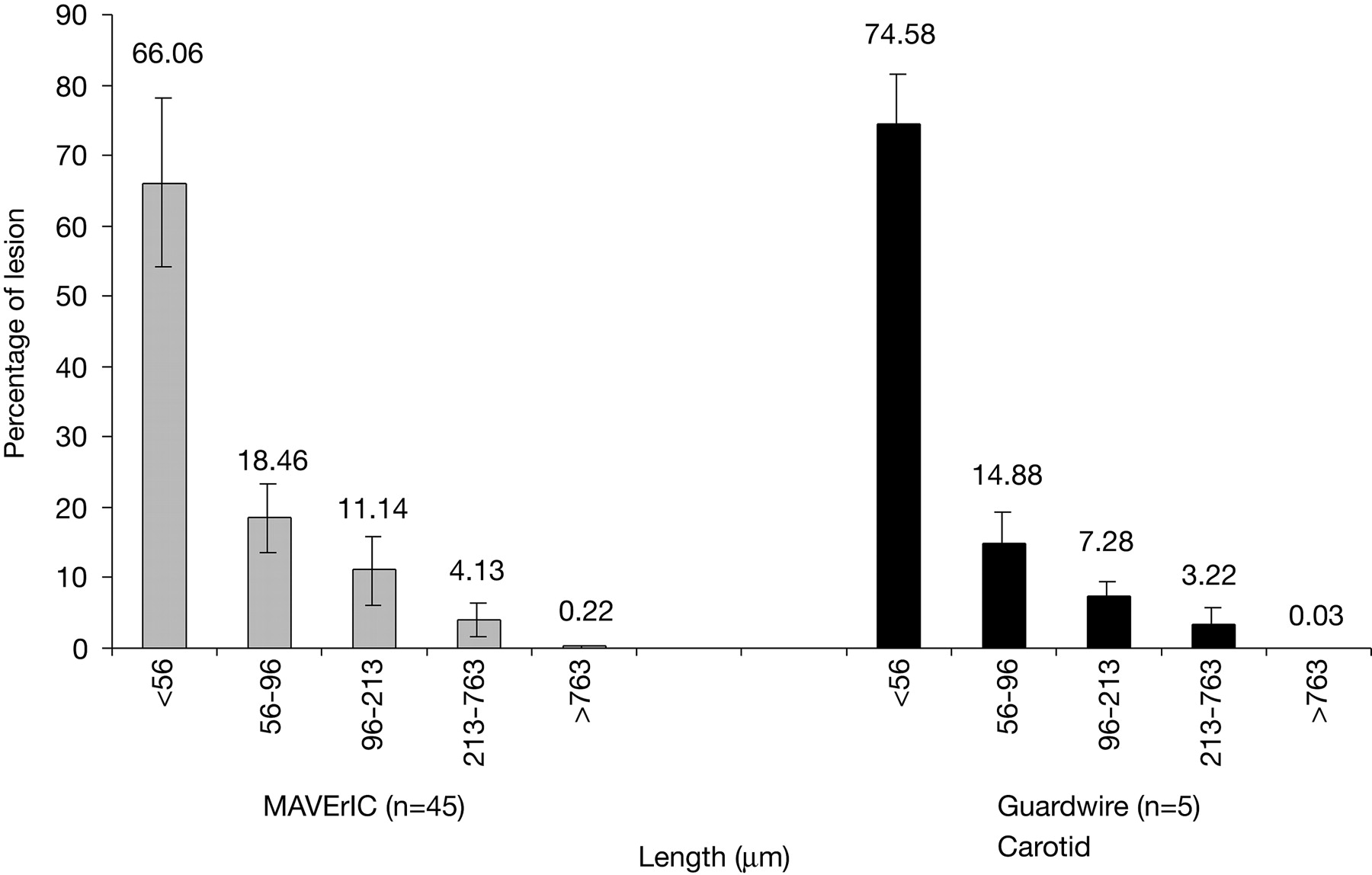
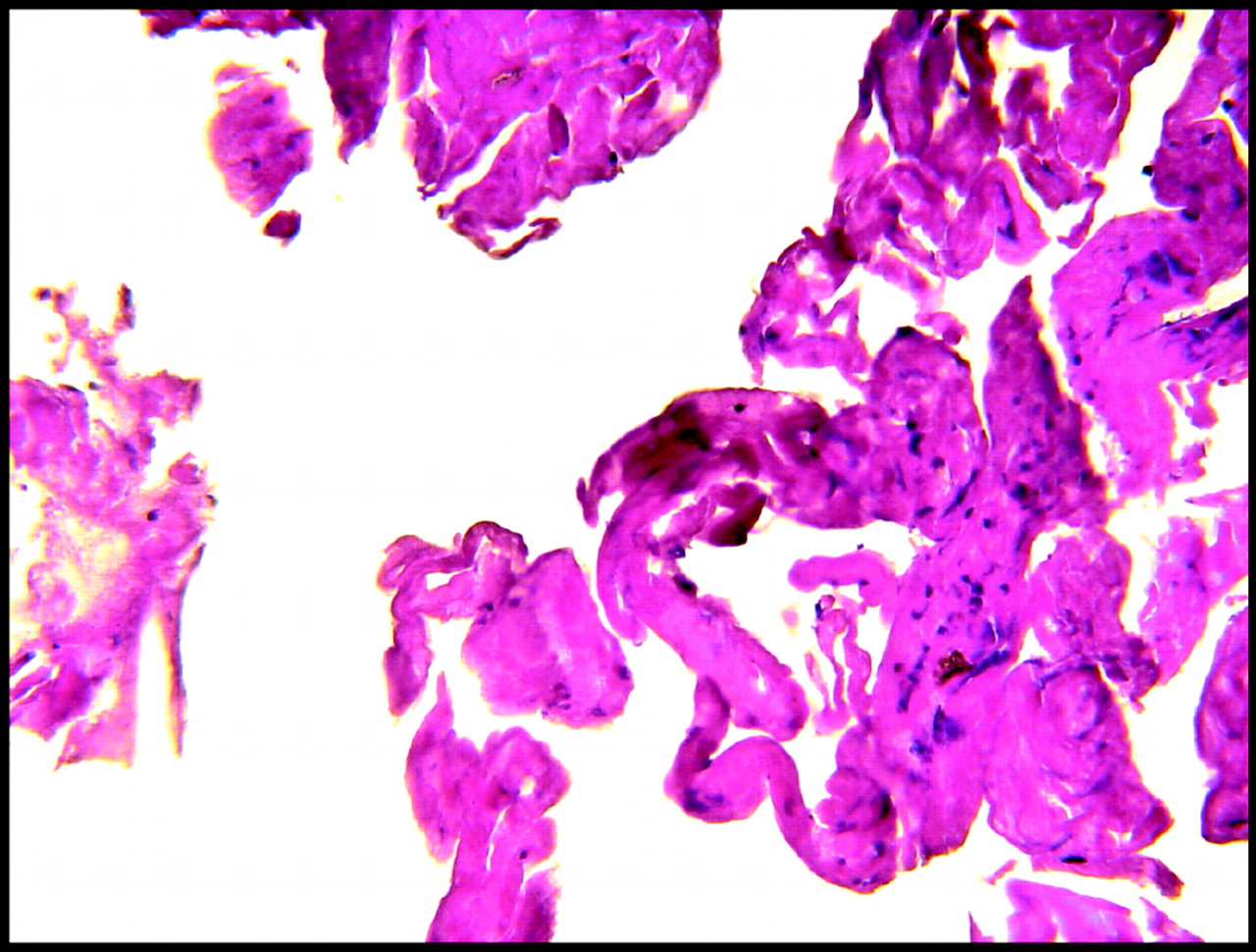
All the filters that were deployed for use and subsequently analyzed (n = 45) contained particulate. Results from the analysis of particulate size distribution indicated that most (85%) of the retrieved material was <96 μm in size (Fig 3). The mean particle width (n = 45) was 39.72 μm, and the mean particle length (n = 45) was 68.0 μm. This particle size distribution is essentially the same as that obtained for the 5 GuardWirePlus samples. The median particulate volume of the filters was 9.71 mm3 (range, 0.0–54.61 mm3). The largest particle captured by the distal protection device was 3374 μm across the major axis. All particulate volumes were within the capacity of the smallest carotid filter (5.5-mm diameter and 120-mm3 volume). The median particulate volume of the 5 GuardWirePlus samples was 10.91 mm3 (range, 2.3–29.5 mm3). Examination of a subset of filters showed that they containd plaque constituents: pools of foam cells; cholesterol clefts; extracellular matrix-/plaquelike material; and, thrombus (Fig 4).

Particulate size distribution results compared with GuardWire+ positive controls.

H&E staining of particulate demonstrating diverse cellular elements including macrophages and foam cells (200×).
Discussion
The purpose of the MAVErIC International Study was to evaluate the feasibility and safety of carotid artery stent placement with distal embolic protection by using the Medtronic Exponent Self-Expanding Carotid Stent in combination with the Medtronic Interceptor Carotid Filter System. In this study, both asymptomatic and symptomatic patients who were at high risk for carotid endarterectomy and who were scheduled to undergo elective stent placement of the carotid artery were included.
The results of MAVErIC International demonstrate high delivery success rates for both the Interceptor Filter System and the Exponent Carotid Stent. Furthermore, the results also show that the procedure was safe, with a low 30-day and 6- and 12-month incidence of MAE. In addition, analysis of most of the Interceptor filter devices used in the procedure demonstrated that most of the particulate retrieved by the study filter-based distal protection device was <100 μm in size, which means that the distal pore size of the filter (approximately 100 μm) was adequate for capturing debris of size comparable to that retrieved by other filters or occlusive balloon-based embolic protection devices such as the GuardWirePlus.24–28 The particulate was positively identified to be of plaque origin, which suggests that the Medtronic Interceptor Carotid Filter captured material liberated from the vessel wall during lesion treatment. The use of the Exponent Stent was also associated with a low restenosis rate, as determined by angiography and by duplex sonography evaluation.
Carotid artery stent placement is rapidly becoming a widely offered alternative to carotid endarterectomy, which is considered the current “gold standard” therapy, particularly in patients with significant comorbidities that make them unsuitable or high-risk candidates for surgical intervention.5,9,10,29 Several studies have demonstrated that carotid artery stent placement can be performed with a complication rate that is similar to that of conventional surgery.15,17,30 A potential concern of angioplasty without protection, however, is distal embolization of particulate matter. Although this may be better tolerated by the myocardium in coronary angioplasty, the brain is more susceptible and small vessel occlusion may lead to catastrophic clinical stroke.
The use of distal protection devices, therefore, affords some measure of control over distal embolization that occurs at the time of stent deployment. Clinical studies have demonstrated the potential of embolic protection devices to reduce the incidence of stroke and death.20 Furthermore, a number of recent studies have demonstrated the potential of such devices in reducing the incidence of embolization of intracranial debris, thereby reducing the frequency of major neurologic adverse events and providing results comparable with those obtained by using surgery.21,25,29–31
Comparison of data obtained with the Exponent Stent coupled with the Interceptor Filter System with those previously reported show that the high rate of delivery success seen here (94.2% for the filter and 95.9% for the stent) is comparable to that obtained elsewhere.21,24–26,29–31 In this patient population, which was considered high risk for carotid endarterectomy, with complex carotid anatomy and comorbidities, the procedure was generally well tolerated. One death occurred because of perioperative MI, and one minor perioperative stroke occurred; however, the rates of stroke and death observed during the 30-day follow-up period are similar to those obtained in controlled clinical studies of carotid endarterectomy in patients generally at lower risk than those enrolled in the present study. The results are also consistent with observations in previous studies where embolic protection in combination with stent placement has been used.21,24–26,29–31 Similarly, the longer-term results are also promising, with the incidence of MAEs at 12 months no higher than that observed in other studies with similar long-term follow-up.29,31 The proportion of patients with a diameter stenosis <49% also remained high, at approximately 80%, at the 6-month follow-up visit.
A lingering question about carotid stent placement is its durabilty. In studies examining the effectiveness of coronary stent placement, restenosis is a frequent problem. Restenosis after carotid artery surgery is rare,32 and it remains to be determined, through studies with long-term follow-up, whether restenosis following stent placement in carotid arteries occurs and whether it is clinically relevant.33 It appears likely that bioengineered drug-eluting stents may provide a solution to the problem of restenosis due to intimal hyperplasia.
The findings from the MAVErIC International Study support the safety and feasibility of carotid artery stent placement with the Exponent Carotid Stent combined with the Interceptor Filter System to prevent distal embolization during carotid endovascular procedures. In light of the encouraging safety data and the pathologic evidence of captured debris presented here and in other studies, it seems probable that distal protection will eventually become the standard of care for all carotid stent placement procedures; however, the effectiveness of embolic protection devices will require further evaluation in long-term randomized clinical studies.
Acknowledgments
The MAVErIC International Study Group: Dr. W. Morrish and Dr. M.D. Hill, Foothills Medical Center, Calgary, Alberta, Canada; ProfessorA. Bona A. Nevelsteen, University Hospital Gasthuisberg, Leuven, Belgium; Dr. K.E. Hauptmann, Krankenhaus der Barmherzigen Brüder, Trier, Germany; Dr. G. Soulez, Hôpital Notre Dame, Montreal, Québec, Canada; Professor A. Bonafé, Hôpital Gui de Chauliac, CHU Montpellier, France; Professor R, Beyar, Rambam Medical Center, Haifa, Israel; Professor Dr. med. J. Schofer, Center for Cardiology and Vascular Intervention, Hamburg, Germany; Dr. M. Amor, Polyclinique d’Essey-Lès-Nancy, Nancy, France; Professor Dr. med. H. Sievert, Kardiologische Zentrum Bethanien KH, Frankfurt, Germany; Dr. T. Lefèvre, Clinique du Bois de Verrières, Antony, France; and Dr. B. Escude, Nouvelle Clinique de L’Union, Saint-Jean, France.
Statement of Authorship: Drs. Hill and Morrish drafted the manuscript. The final manuscript was reviewed by all, and the services of a professional editor were used. All authors contributed to design and data collection and can take responsibility for the data.
The MAVErIC International Study was funded by Medtronic, Inc. Dr. Hill was funded by the Heart & Stroke Foundation of Alberta/NWT/Nunavut and the Canadian Institutes for Health Research. We gratefully acknowledge Philip Seifert, the Biomedical Engineering Center, Harvard-MIT Division of Health Sciences and Technology, for his expert assistance with the histology analysis.
References
- Received May 22, 2005.
- Accepted after revision August 21, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- New Ischemic Brain Lesions on Diffusion-Weighted MRI after Carotid Artery Stenting with Filter Protection: Frequency and Relationship with Plaque Morphology
- Evaluation of the Medtronic Exponent Self-Expanding Carotid Stent System With the Medtronic Guardwire Temporary Occlusion and Aspiration System in the Treatment of Carotid Stenosis: Combined From the MAVErIC (Medtronic AVE Self-expanding CaRotid Stent System with distal protection In the treatment of Carotid stenosis) I and MAVErIC II Trials
- Endarterectomy and Stenting for Asymptomatic Carotid Stenosis: A Race at Breakneck Speed