
Abstract
SUMMARY: A 60-year-old woman developed right-eye vision loss secondary to rhinocerebral mucormycosis. Routine MR imaging sequences including enhanced MR imaging showed normal optic nerves, but a diffusion-weighted sequence and apparent diffusion coefficient maps revealed markedly restricted diffusion in the right optic nerve. This MR imaging abnormality of optic nerve infarction due to mucormycosis has not been reported previously.
A 60-year-old woman presented with swelling and redness of the right eye for 14 days. She denied any vision loss or any history of eye trauma. Her medical history was significant for diabetes mellitus and myelodysplastic syndrome. Examination of the right eye on day 1 was remarkable for proptosis, conjunctival injection, and restricted extraocular motility in all directions. Visual acuity and findings of a fundus examination were completely normal, as was the left eye. Her white blood cell count was 4000/cubic millimeter, and her blood sugar level was 200 mg/dL. CT showed mucosal thickening compatible with sinusitis involving the right maxillary, frontal, ethmoid, and sphenoid sinuses with retro-orbital and periorbital inflammatory changes and no evidence of abscess formation. She was admitted with a working diagnosis of right orbital cellulitis and right pansinusitis. The patient was started on broad-spectrum antibiotics and steroids. She also underwent a sinus surgery involving right maxillary antrostomy with partial ethmoidectomy. The pathologic examination of the surgical specimen revealed islands of fungal elements suggestive of Aspergillus organisms. The bacterial cultures were negative for any growth. Voriconazole was added to the treatment regimen, which lead to significant clinical improvement.
On day 15, the patient's symptoms relapsed, and she developed vision loss in the right eye, altered mental status, and complete right orbital apex syndrome. Right afferent pupillary defect was present. The left eye was normal. Findings of a fundus examination were normal in both eyes. MR imaging of the brain, performed on day 16, showed evidence of extension of inflammation to the right buccal space, infratemporal fossa, and masticator space, with retromaxillary abscess formation as well as necrotic changes in the muscles of the region. The optic nerves appeared normal on all sequences including postcontrast and the diffusion-weighted images (DWI). On the basis of the MR imaging findings, an invasive fungal infection was suspected, with primary consideration for mucormycosis. The pathology specimens were also reviewed, and they were consistent with invasive Mucor infection. On the basis of the MR imaging findings and review of pathology specimens, a diagnosis of rhinocerebral mucormycosis was considered, and the patient was started on amphotericin B. Surgery was also considered but the patient refused it.
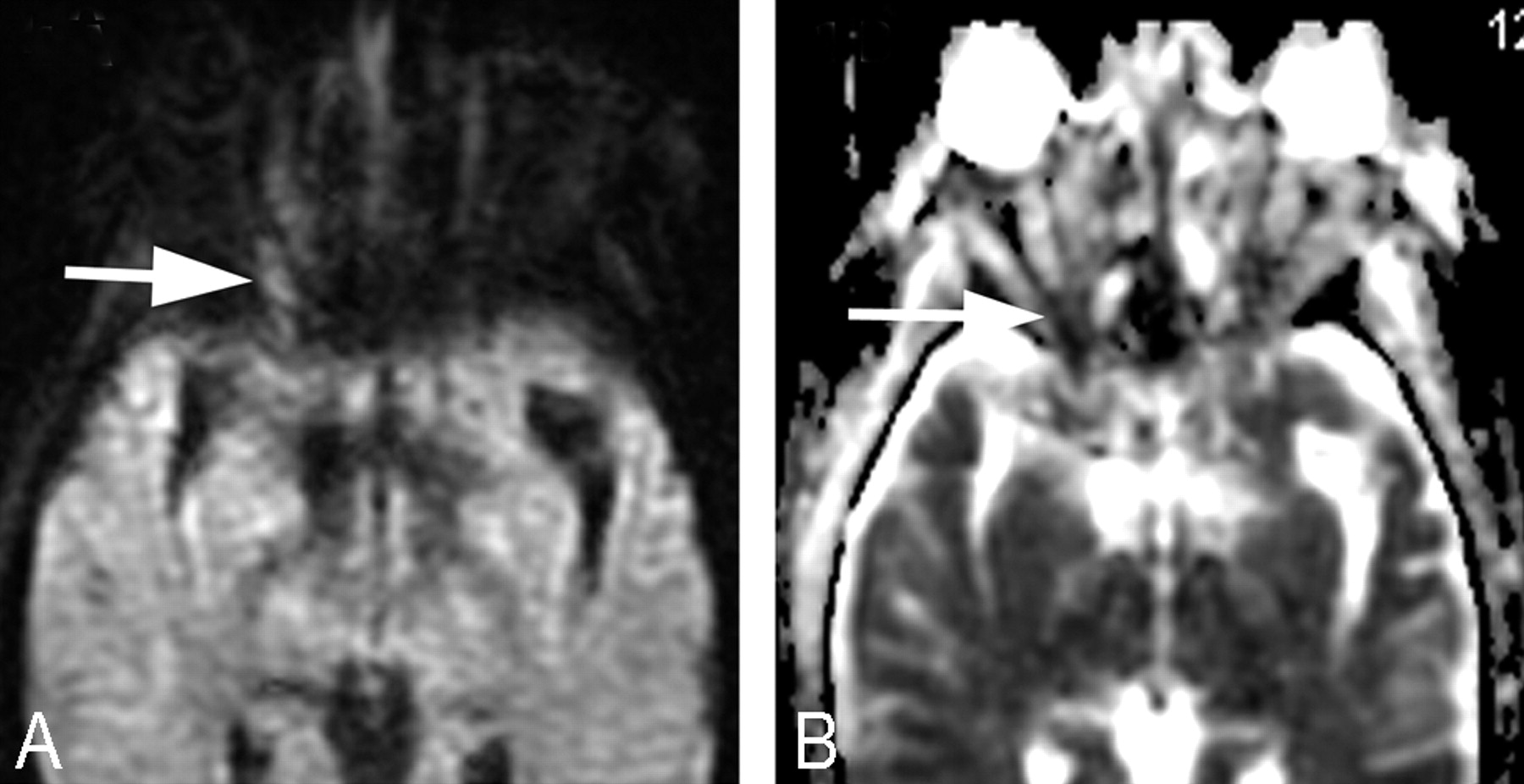
Despite aggressive medical management, the patient's visual loss progressed rapidly in the right eye, leading to complete blindness by day 19. A repeat MR imaging on day 21 showed worsening of the inflammatory process, which now involved the right cavernous sinus. The right optic nerve showed subtle findings of restricted diffusion on DWI (Fig 1). However, the T2-weighted, fluid-attenuated inversion recovery (FLAIR), and T1-weighted postcontrast sequences did not show any optic nerve abnormality.

MR imaging performed 6 days after vision loss in the right eye. A, DWI shows subtle high signal intensity in the posterior right optic nerve (arrow). B, ADC map shows hypointense posterior right optic nerve (arrow).
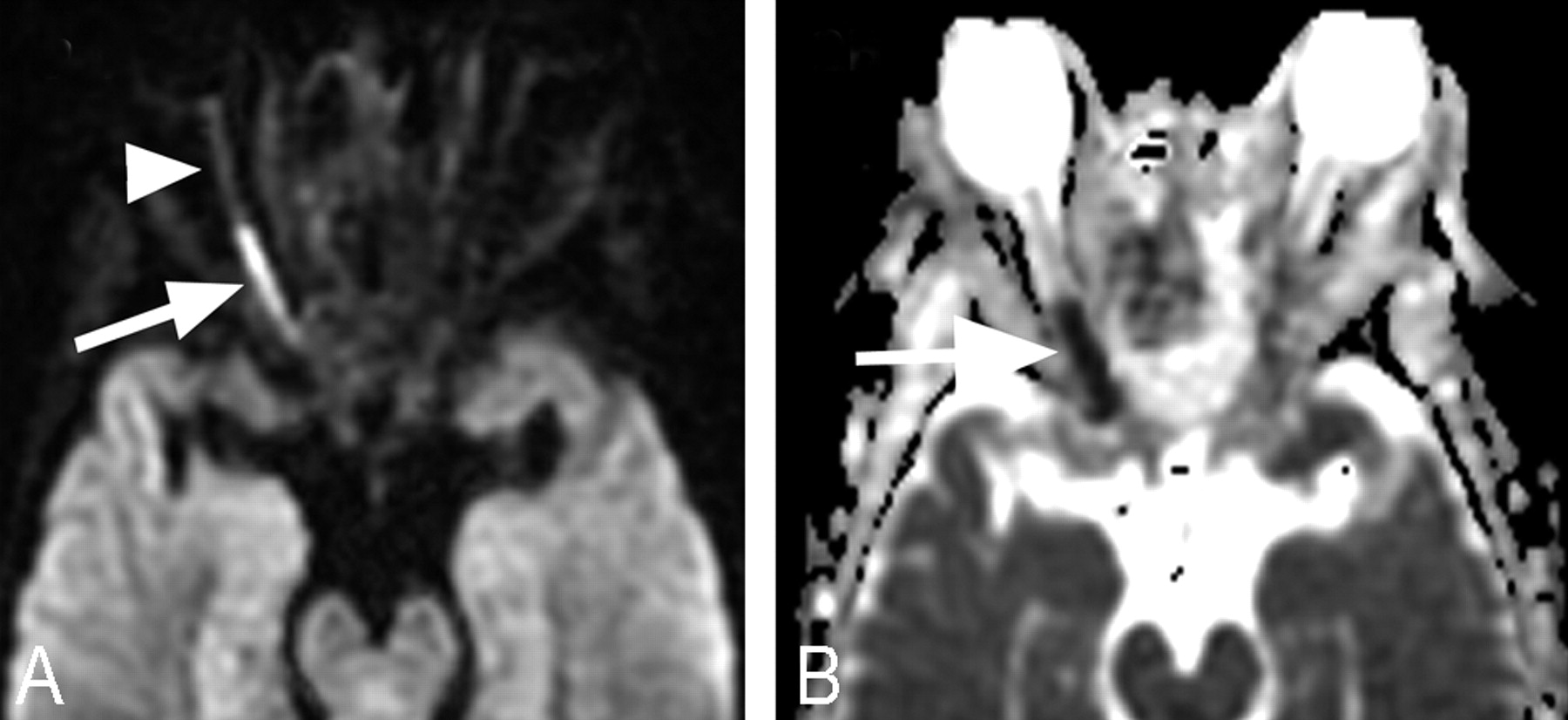
By day 30, the patient developed orbital apex syndrome and vision loss in the left eye. Repeat MR imaging, performed on day 31, showed extension of the inflammatory changes to the left side involving the left sphenoid sinus, left orbit, and left infratemporal fossa. The right optic nerve showed markedly restricted diffusion on DWI and was hypointense on the apparent diffusion coefficient (ADC) map (Fig 2). There was no abnormal signal intensity in the right optic nerve on other MR images.

MR imaging performed 15 days after vision loss in the right eye. A, DWI demonstrates marked diffusion restriction in the posterior right optic nerve (arrow). Note that there is no obvious signal-intensity change of the retrobulbar portion of right optic nerve (arrowhead). B, ADC map shows a hypointense posterior right optic nerve (arrow).
On hospital day 33, the poor prognosis was discussed with the patient's family, and she was transferred to the hospice care, where she ultimately died.
Discussion
Our patient experienced complete right-sided vision loss as a result of rhinocerebral mucormycosis. The MR imaging performed 6 days after the onset of vision loss in the right eye revealed subtle high signal intensity in the right optic nerve on DWI. This signal-intensity abnormality became more obvious on the MR imaging performed 15 days after the onset of vision loss in the right eye. T2-weighted, FLAIR, and T1-weighted postcontrast sequences did not show any recognizable signal-intensity abnormality in the optic nerves. This finding suggests that the abnormal signal intensity due to restricted diffusion may be the earliest abnormality on MR imaging after optic nerve infarction and that this abnormal signal intensity becomes better visualized with time.
The pattern of abnormal signal intensity in the optic nerve suggests the involvement primarily of the posterior intraorbital segment of the nerve (Fig 2). This pattern, in the presence of normal finding on FLAIR and postcontrast MR images, is suggestive of ischemic optic nerve infarction, possibly due to vascular invasion by Mucor organisms.
The symptom of sudden-onset blindness in rhino-orbitocerebral mucormycosis has been correlated histologically with central retinal artery occlusion,1 ophthalmic artery necrosis,2 optic nerve infarction and necrosis,1,2 or direct optic nerve infection by mucormycosis.2 The main contribution of CT or MR imaging to the diagnosis of mucormycosis is its clear demonstration of the relationship between nasal, sinus, and orbital disease along with tissue necrosis, a relationship so typical of mucormycosis that this diagnosis should be considered whenever combined nasal, sinus, and orbital diseases are encountered.3 The addition of DWI increases the imaging diagnosis of ischemic optic neuropathy, as shown in this patient.
On searching the literature, we found only 2 case reports on diffusion characteristics of acute ischemic optic neuropathy.4,5 The restricted diffusion in optic nerves has been shown in patients with perioperative hypotensive posterior ischemic optic neuropathy4 and nonarteritic posterior ischemic optic neuropathy.5 The time period between the onset of visual loss and the demonstration of restricted diffusion in these cases was approximately 4 days4 and 12 days.5 This is very similar to our patient in whom subtle findings of restricted diffusion were first evident 6 days after onset of vision loss.
We conclude from this case that DWI sequences play an important role in demonstrating optic nerve infarction, especially when regular MR imaging sequences show normal optic nerves. Restricted diffusion on MR imaging may be the earliest abnormality detectable in acute ischemic optic neuropathy due to rhinocerebral mucormycosis.
- Received March 29, 2006.
- Accepted after revision April 10, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- MRI signs helpful in the differentiation of patients with anterior ischaemic optic neuropathy and optic neuritis
- Rhino-orbital-cerebral mucormycosis
- Hyperintense Optic Nerve Heads on Diffusion-Weighted Imaging: A Potential Imaging Sign of Papilledema
- Diffusion Changes in the Vitreous Humor of the Eye during Aging
- The "Black Turbinate" Sign: An Early MR Imaging Finding of Nasal Mucormycosis