
Abstract
BACKGROUND AND PURPOSE: Optic nerve tortuosity is one of several nonmalignant abnormalities documented on MR imaging in patients with neurofibromatosis type 1 and may be related to the development of optic pathway gliomas. This study seeks an operational definition for optic nerve tortuosity.
MATERIALS AND METHODS: A focus group of 3 pediatric neuroradiologists reviewed 20 MR images of the brain and orbits of patients suspected to have optic nerve tortuosity in the absence of optic pathway glioma and found 6 radiographic factors that occurred frequently. Subsequently, 28 MR images were assessed for the presence of optic nerve tortuosity, using a global assessment question that reflects a neuroradiologist's confidence in the presence of optic nerve tortuosity, and for the presence of the 6 radiographic factors, to identify a combination of these factors that best predicted a diagnosis of optic nerve tortuosity.
RESULTS: We found perfect inter-rater agreement between 3 readers on the presence/absence of tortuosity in 75% of cases. Lack of congruity of the optic nerves, in more than 1 coronal section and dilation of the subarachnoid space surrounding the optic nerves, when found together are sensitive (89%) and specific (93%) for a diagnosis of tortuosity on the global scale. The absence of these 2 factors, along with absence of deviation of the optic nerve within the axial plane, provides a reliable test to exclude tortuosity.
CONCLUSION: Lack of congruity of the optic nerves in more than 1 coronal section and dilation of the subarachnoid space surrounding the optic nerves together provide an operational radiographic definition of optic nerve tortuosity.
Neurofibromatosis type 1 (NF-1) is a common neurocutaneous disorder that affects approximately 1 in 3000 people worldwide.1 Two of 7 clinical diagnostic criteria, as developed by the National Institutes of Health consensus conference, must be met to make the diagnosis of NF-1 in the absence of genetic documentation of disease.2 One of these 7 criteria is the presence of an optic pathway glioma (Fig 1). Optic pathway gliomas are the most common central nervous system (CNS) neoplasm in patients with NF-1 and because of their location, vision loss often occurs. CT of asymptomatic patients with NF-1 has shown the prevalence of optic pathway glioma to be 15%–19% at 4 years of age.3–5 Approximately 47% of patients with a known optic pathway glioma will develop vision loss.6

Optic glioma.
A, Sagittal spin-echo image (TR, 643 ms; TE, 12 ms) shows markedly enlarged optic nerve (arrow).
B, Axial fast spin-echo (TR, 6000 ms; TE, 84 ms) image shows bilateral enlargement, along with tortuosity of intraorbital optic nerves (arrow).
Optic nerve tortuosity is one of several nonmalignant abnormalities documented on MR imaging in patients with NF-1.7–10 The course of the optic nerve exhibits abnormal curvature, but the optic nerve itself is not thickened and does not enhance with gadolinium administration and therefore does not meet diagnostic criteria for optic pathway glioma.11 Previous studies have reported the incidence of optic nerve tortuosity in patients with NF-1 to be between 12% and 31%.5,11
It is unknown whether optic nerve tortuosity is a precursor to the development of optic pathway gliomas. However, before this question can be answered directly, optic nerve tortuosity must be objectively defined. This study seeks a case definition of optic nerve tortuosity by relating a global assessment question that reflects a neuroradiologist's confidence in the presence of optic nerve tortuosity to individual radiographic findings that may predict the presence of optic nerve tortuosity. A consistent relationship between the global assessment and individual radiographic findings yields an objective case definition of optic nerve tortuosity.
Materials and Methods
We identified 20 MR images of the brain and orbit between the years 2000 and 2005 that were suspected, based on formal reading, to have tortuosity of the optic nerves in the absence of optic pathway glioma. A focus group, involving 3 pediatric neuroradiologists at a tertiary care pediatric hospital that serves as a national referral site for children with NF-1, reviewed these MR images. Open-ended questions were posed to encourage the participants to describe individual images and to establish patterns seen across multiple images in an attempt to identify a group of radiographic findings that may define a patient with optic nerve tortuosity.
Using the findings of the focus group, an instrument was designed, based on previously validated methods used in assessment of chronic pain, to facilitate evaluation of individual MR images for the presence of optic nerve tortuosity (Appendix).12,13 This instrument contained a single global assessment question to determine whether on formal reading the radiologist would document the presence of tortuosity. Answers to the global assessment were recorded on a 5-point Likert scale.14 The central item on the scale, “Toss-up,” was described as complete uncertainty in regard to the presence of tortuosity, with absolute certainty reserved for either pole of the scale. In addition, the instrument contained an assessment of the presence or absence of the findings identified by the focus group to occur regularly in cases of optic nerve tortuosity. Using this instrument, 3 neuroradiologists, blinded to identifying information, evaluated the 20 MR images of the brain and orbits previously suspected to have optic nerve tortuosity. In addition, 8 normal MR images were included to assess the readers’ ability to exclude images with normal optic nerves. We anticipated that 28 cases, read by 3 radiologists, would provide 84 individual assessments for tortuosity and thus an adequate sample size to establish sufficient confidence intervals around the final outcomes.
Descriptive statistics were used to quantify agreement among the neuroradiologists for the global assessment of tortuosity and for the presence/absence of the radiographic findings thought to be significant in the diagnosis of optic nerve tortuosity. Perfect inter-rater agreement occurred when all 3 radiologists agreed on the presence of an individual item.15 Majority inter-rater agreement signified that 2 of 3 agreed on an item. A total score was calculated for each case by indicating the number of radiographic factors that an individual reader determined to be present on an individual case (Appendix). A mean total score was calculated for each case and represented the average number of radiographic factors identified by 3 readers on a single case. Four cases had incomplete image sets, precluding calculation of a mean total score.
Two hypotheses were tested. First, we hypothesized that cases defined as “definitely tortuous” or “probably tortuous” on the global assessment would have a higher mean total score, signifying a greater number of the 6 radiographic factors present, than cases defined as “toss-up,” “probably not tortuous,” and “definitely not tortuous.” Second, we hypothesized that a subset of the 6 radiographic findings would accurately predict a diagnosis of “definitely tortuous” or “probably tortuous” on the global assessment. Using multivariable logistic regression, receiver operating characteristic (ROC) curves were created for all possible combinations of the 6 radiographic factors. The concordance statistic (C statistic) was calculated for each ROC curve, and the sensitivity and specificity of each possible combination used as a test for the diagnosis of tortuosity was calculated.16(p63-5) Results were then stratified by combinations of factors, being either all present or all absent. Stratum specific likelihood ratios were then used to calculate the odds that a given result would appear in a patient with optic nerve tortuosity, as opposed to a patient without optic nerve tortuosity.17 Thus, the combination of factors with the highest likelihood ratio is the test that best rules in a diagnosis of optic nerve tortuosity. Likewise, the combination of factors with the lowest likelihood ratio (less than 1) is the test that best rules out tortuosity. The likelihood of making the correct diagnosis regarding the presence of tortuosity after application of a given set of factors (post-test odds of disease) was calculated by multiplying the likelihood ratio by the pretest odds of disease.
This investigation was performed under the approval of the institutional review boards of Children's Hospital of Pennsylvania and the University of Pennsylvania. All calculations were performed on Stata, version 9.0 (Stata, College Station, Tex).
Results
Six radiographic findings were determined by the participants of the focus group to occur with regularity (Fig 2) and to be relevant to a final diagnosis of optic nerve tortuosity. All 6 items were included on the global assessment instrument (Appendix).

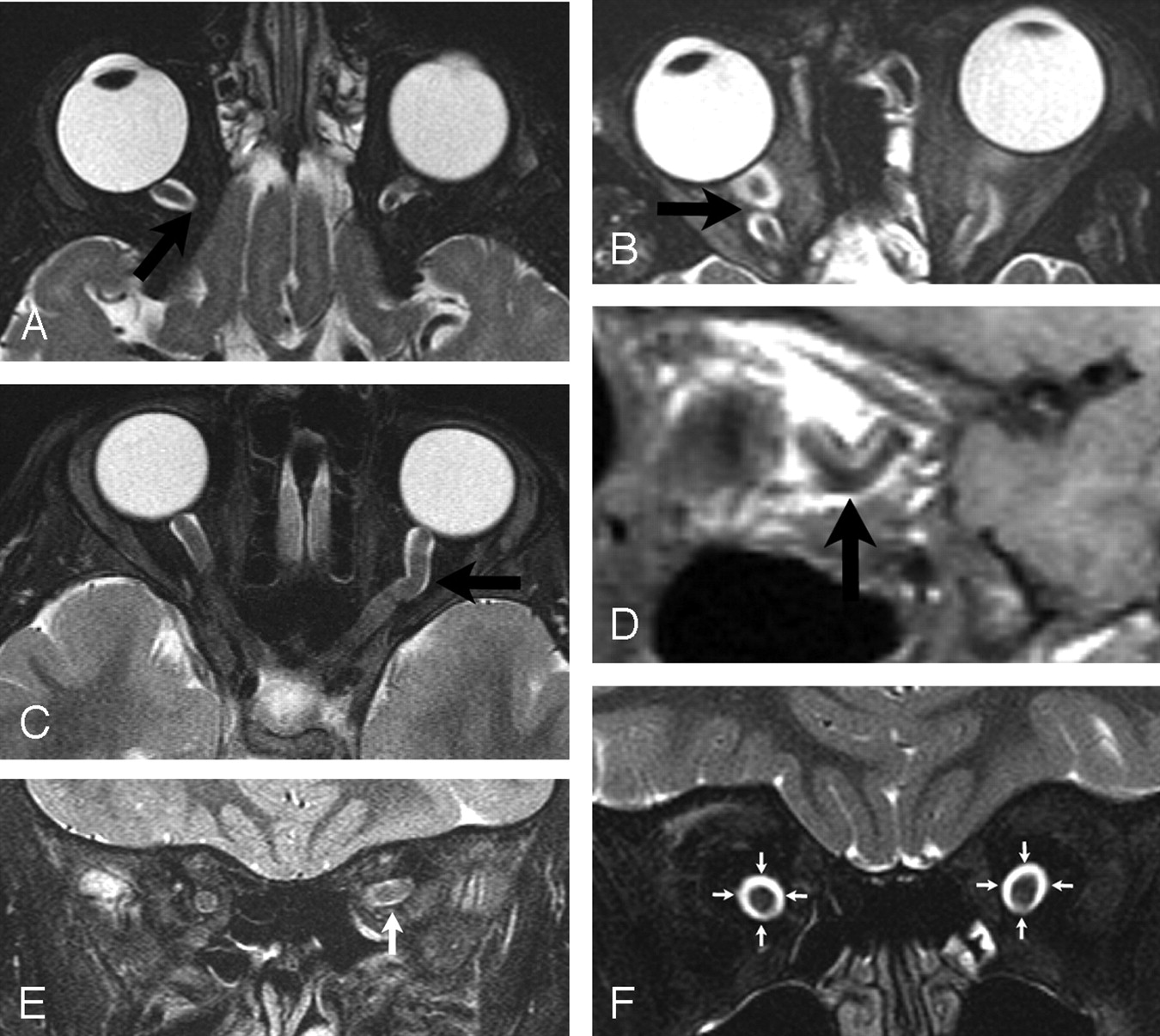
Tortuosity of optic nerves
A, Axial fast spin-echo T2-weighted image showing factor 1: interruption of the optic nerve out of the axial plane (tip of arrow) without return.
B, Axial fast spin-echo T2-weighted image showing factor 2: interruption of the optic nerve out of the axial plane (tip of arrow) with return of the nerve into the axial plane.
C, Axial fast spin-echo T2-weighted image showing factor 3: deviation of the optic nerve within the axial plane (arrow).
D, Sagittal T1-weighted image showing factor 4: increased curvature (tip of arrow) in the sagittal plane.
E, Coronal fast spin-echo T2-weighted image showing factor 5: lack of congruity of the optic nerves (arrow) in the coronal plane.
F, Coronal fast spin-echo T2-weighted image showing factor 6: dilation of the subarachnoid space (encircled by arrows) surrounding anterior portion of optic nerves.

Using the single global assessment question from the created instrument, perfect agreement among the readers on a 5-point Likert scale regarding the presence/absence of optic nerve tortuosity occurred in 14 cases (50%; Table 1). Perfect agreement among radiologists occurred only in the categories “definitely tortuous” and “definitely not tortuous.” Readers were never unanimous on the 3 central items that suggested neutrality or uncertainty. Majority agreement occurred in 23 cases (82%), again with most cases (19) occurring at the poles of the Likert scale, where readers were “definite” about the presence/absence of tortuosity. When the 5-point Likert scale was dichotomized into the more clinically relevant outcome measure of tortuous (“definitely tortuous” + “probably tortuous”) versus not tortuous (“definitely not tortuous,” “probably not tortuous,” and “toss-up”), the readers perfectly agree in 75% of the cases. In 4 cases, all 3 readers recorded different readings on the Likert scale, indicating complete disagreement.
5 item global assessment results by case number for 3 readers
Of the radiographic findings suspected to be components of optic nerve tortuosity, 4 (factors 1, 3, 4, and 5) had at least 70% 3-reader perfect agreement for the presence/absence of the radiographic finding (Table 2). Increased curvature in the sagittal plane (4) was the radiographic finding most commonly diagnosed (44 times) by the evaluators, followed by factors 3 (40 times), 6 (38 times), 5 (34 times), 2 (33 times), and 1 (24 times).
Individual predictors of tortuosity
Four cases had incomplete image sets, which precluded calculation of a mean total score. For the 24 cases with a complete set of images, mean total scores ranged between 0 and 5 (Table 2). All cases defined as tortuous (“definitely tortuous” + “probably tortuous”; 9 cases) on the global assessment had a mean total score of 4 or greater. All remaining cases had a mean total score of less than 4. Thus, a cutoff value of 4 for the mean total score (4 of 6 possible radiographic items found to be present in a given case) was both 100% sensitive and 100% specific for a diagnosis of tortuosity on the global assessment in this case series. Of the 20 original cases suspected to have tortuosity, 7 were defined as tortuous (“definitely tortuous” + “probably tortuous”) by the radiologists.
Univariate analysis of the presence of the 6 radiographic factors revealed that dilation of the subarachnoid space surrounding the optic nerve (6, odds ratio [OR] = 29) and lack of congruity of optic nerves on multiple coronal sections (5, OR = 24) most commonly corresponded with a diagnosis of tortuosity on the global assessment scale (Table 3). Evaluation of all possible combinations of the 6 radiographic factors demonstrated that factors 5 (lack of congruity of the optic nerves across multiple coronal sections) and 6 (dilation of the subarachnoid space surrounding the optic nerve) occurring together are the most sensitive and specific test for detection of an outcome of tortuosity on the global assessment scale (Table 4). Presence of this pair provides the best diagnostic test for ruling in tortuosity (LR+ = 13.3, Table 5). The best test to exclude a diagnosis of optic nerve tortuosity includes additional assessment for radiographic factor 3. When radiographic factors 3, 5, and 6 are all absent, optic nerve tortuosity is excluded in this dataset (LR− = 0, Table 5). The predictive nature of these items is unchanged when tortuosity is defined to include rather than exclude the “toss-up” item on the Likert scale.
Univariate analysis of radiographic factors for predicting a diagnosis of tortuosity
Radiographic factor combinations that predict a diagnosis of tortuosity
Likelihood ratios of key radiographic factor combinations
Discussion
The presence of 2 distinct radiographic factors (ie, factor 5, lack of congruity of optic nerves on multiple coronal sections, and factor 6, dilation of the subarachnoid space surrounding the optic nerve) corresponds with a diagnosis of optic nerve tortuosity, thus providing a consensus definition for tortuosity that can be reliably applied by radiologists across institutions. Consensus methods exist (Delphi, nominal group method) that rely on the subjective opinions of experts to create definitions for controversial subjects.18,19 Our use of a global assessment instrument provides a more quantitative approach and uses well established methods to reach a consensus definition for optic nerve tortuosity. We applied this tool to identify optic nerve tortuosity in our case series (9 of 28 cases) and to correlate it with specific radiographic findings.13,12,20 Thus, the use of the global assessment instrument allows a systematic, quantitative, data-driven approach to determine an objective definition for an important radiographic entity that, before this report, had only been subjectively described. This definition should reduce interobserver variability in the diagnosis of optic nerve tortuosity, allowing future assessment of this entity and its relationship to the development of optic pathway gliomas.
In this study, presence of any 4 of the 6 radiographic factors predicts a diagnosis of tortuosity and less than 4 predicts the absence of optic nerve tortuosity. Evaluation for all 6 factors, however, is cumbersome, because it requires multiple MR imaging sequences that may not be routinely performed at many institutions. In fact, 4 of our 28 cases (14%) were not complete for evaluation; coronal sequences were the most commonly omitted. Alternatively, lack of congruity of the optic nerves on coronal sequences and the presence of dilation of the subarachnoid space (factors 5 and 6) occurring together is extremely sensitive for a diagnosis of optic nerve tortuosity. The likelihood ratio of 13.3 suggests that when these 2 factors are present, the posttest odds of tortuosity are over 13 times higher than the pretest odds of tortuosity with this test result. Thus, if the pretest risk of tortuosity is approximately 20%, as suggested by the literature, and factors 5 and 6 are present, the posttest risk of optic nerve tortuosity is 77%. Therefore, presence of factors 5 and 6 provides increased confidence in the diagnosis of optic nerve tortuosity.
However, because there is concern that tortuosity may presage tumor growth and vision loss, a screening test should be extremely reliable when it excludes optic nerve tortuosity. Absence of factor 3 (deviation of the optic nerve within the axial plane) in the context of the absence of factors 5 and 6 provides increased confidence in ruling out optic nerve tortuosity. In this series, no cases that had absence of these 3 factors were diagnosed with tortuosity (LR− = 0). As a result, we recommend that factors 3, 5, and 6 be assessed in all MR imaging scans obtained to rule out optic nerve tortuosity.
Although factors 3, 5, and 6 (present and absent) provide the ideal screening test for optic nerve tortuosity, coronal sections, necessary for identification of factor 5, were the most commonly omitted sequence in our study and may not be routinely performed in children with NF-1. Therefore, we recommend that all MR imaging series for evaluation of optic nerve tortuosity include coronal sections in addition to axial and sagittal sections and that evaluation include T2-weighted sequences with 2–3-mm cuts through the orbit.
An additional concern is the limited agreement among neuroradiologists regarding the presence of dilation of the subarachnoid space surrounding the optic nerve. We hypothesize that tortuosity of an optic nerve causes strain on the arachnoid layer of the meninges surrounding the optic nerve, thus creating the potential for enlargement of the subarachnoid space. Our 3 neuroradiologists demonstrated only 64% inter-rater agreement for this entity, raising concern that less experienced radiologists might be even less reliable in their determination of the presence of this entity. However, the presence of dilation of the subarachnoid space surrounding the optic nerve remains valid in the prediction of tortuosity despite poor inter-rater agreement, which suggests that any attempt to improve agreement on this item will only increase its predictive ability. Based on this, further efforts to quantitatively define dilation of the subarachnoid space in children with NF-1 are necessary.
Conclusion
Children with optic nerve tortuosity may be at increased risk of developing tumors of the optic pathway. Thus, it is imperative to determine a case definition of optic nerve tortuosity if future evaluation of its relationship to tumor development and vision loss is to occur. In this study, we use an objective, quantitative instrument to demonstrate that dilation of the subarachnoid space surrounding the optic nerve and lack of congruity of the optic nerves across multiple coronal planes provides a reliable case definition of optic nerve tortuosity and identifies a population of patients with NF-1 who should be followed with additional imaging. Coronal images are critical to the diagnosis of tortuosity and should routinely be obtained.
Footnotes
The authors report no conflict of interest regarding the content of this report.
References
- Received May 22, 2006.
- Accepted after revision July 24, 2006.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}