
Abstract
BACKGROUND AND PURPOSE: Diffusion-weighted imaging (DWI) is a novel method of studying the brain that creates tissue contrast secondary to water diffusion. Central nervous system (CNS) vasculitis is a rare inflammatory disease that continues to be difficult to diagnose and evaluate with MR imaging. DWI with apparent diffusion coefficient (ADC) analysis may demonstrate abnormalities within the brain that would otherwise be undetected by conventional imaging, thus aiding in the diagnosis and evaluation of patients with CNS vasculitis.
MATERIALS AND METHODS: A retrospective analysis was performed of patients who were diagnosed with CNS vasculitis and had undergone DWI. A total of 15 patients who had DWI with b = 1000 were analyzed. Regions of interest were drawn in the anterior, central, and posterior regions of white matter (WM) at 3 levels. Regions of interest were also drawn bilaterally in the caudate heads, putamina, thalami, posterior internal capsules, and the cerebellar WM. ADC values were measured and compared with 15 healthy controls who were matched for age, sex, and MR imaging scanner.
RESULTS: There was a significant increase in the ADC values (P < .00625) for the anterior WM, central WM, thalami, and posterior internal capsules in patients with CNS vasculitis.
CONCLUSION: Diffuse increase in water diffusion was present in the normal-appearing brain in patients with CNS vasculitis, and these abnormalities were not demonstrated by conventional MR imaging sequences. The detection and quantification of ADC abnormalities may provide useful diagnostic information for patients with CNS vasculitis.
Central nervous system (CNS) vasculitis is a rare inflammatory disease that affects the arteries and the veins of the brain.1, 2 MR imaging often demonstrates brain lesions in patients with CNS vasculitis.3–7 However, there are numerous examples of conventional MR imaging not demonstrating lesions in patients with proved vasculitis.5, 6 The limited sensitivity of conventional MR imaging to CNS vasculitis changes is demonstrated by cases in which angiographic abnormalities are present despite normal findings on MR imaging examination.4, 5, 7, 8
Diffusion-weighted imaging (DWI) provides a novel method of investigating the brain, which relies on the molecular diffusion of water for tissue contrast.9 Apparent diffusion coefficient (ADC) analysis allows a quantitative measurement of changes within the brain. Brain analysis using ADCs has been found to demonstrate abnormalities that are not detectable by conventional MR imaging for multiple sclerosis, tuberous sclerosis, Behcet's disease, neurofibromatosis type 1 (NF1), and the aging brain.10–14 The detection of abnormalities in the brain by DWI, not otherwise visualized by MR imaging, may help to determine the extent of abnormalities in patients with CNS vasculitis.
We evaluated the normal-appearing brain as demonstrated by conventional MR imaging with DWI using ADC analysis to enhance our understanding of the extent and type of changes present in patients with CNS vasculitis. We hypothesized that there would be diffuse abnormalities present within the brain, resulting in increased diffusion and thus increased ADC values.
Materials and Methods
The medical records were searched by computer for patients with the diagnosis of cerebral vasculitis from 1998 to 2005. Since 1998, brain MR imaging has been routinely performed with a DWI sequence. Only cases of inflammatory vasculitis were included. The cases considered to represent vasculitis had to have a clinical diagnosis of vasculitis and 1 of the following: 1) pathologic evidence, 2) classic vasculitis pattern on an angiogram, or 3) clinical course and a response to therapy consistent with vasculitis.3, 15 The diagnosis of vasculitis was based on clinical history and pathology evidence in 6, clinical history and vasculitis pattern on angiograms in 8, and clinical course with response to therapy in 1. The diagnosis was primary CNS vasculitis in 12 patients and vasculitis secondary to sarcoid in 2 patients.
There were 15 patients who met our entry criteria (4 men, 11 women; mean, 51.9 years of age; range, 39–74 years of age). Symptoms in patients had been present from 2 days to 20 days. Eleven patients were imaged within 10 days of the onset of symptoms. The others were imaged after approximately 13, 20, and 45 days of symptoms.
Fourteen subjects underwent scanning with 1.5T; and 1, with 3T MR imaging systems. The MR imaging studies are summarized as follows: 9 studies on Signa (GE Healthcare, Milwaukee, Wis), 1 study on Magnetom Vision (Siemens, Erlangen, Germany), 2 studies on Symphony (Siemens), 2 studies on Avanto (Siemens), and 1 study on Trio (Siemens). Fluid-attenuated inversion recovery (FLAIR) and DWI with b = 1000 were performed in all patients.
There was a total of 8 cases that were considered to have vasculitis but were not included in the data analysis. One case had corrupt diffusion source data; 1 case was saved on a storage disk that could no longer be accessed; 1 patient had only MR imaging performed outside our institution, the results of which could not be obtained; and 5 of the vasculitis patients had only follow-up imaging at our institution. Additionally, 3 more patients were excluded as result of not having a true inflammatory vasculitis and/or having a complicated history. One patient was scanned after surgery and radiation therapy for an astrocytoma, and there were 2 patients with Susac Syndrome (a clinical triad of encephalopathy, hearing loss, and retinal arteriolar occlusions).
Four-vessel angiography was performed using a digital subtraction technique in all patients. The angiograms were reviewed in a blinded fashion by a neuroradiologist, and the reports were also reviewed. The blinded reviews of the angiograms were all in agreement with the original interpretation.
The control subjects were matched for age, sex, and MR imaging scanner. There were 4 male and 11 female controls with a mean of 50.2 years of age (range, 36–67 years of age). Each control MR imaging was interpreted as having normal findings on brain examination. The indications for examinations of the control subjects included the following: asymmetric sensorineural hearing loss, headaches, anterior communicating artery aneurysm, bilateral upper extremity numbness, paresthesias and facial weakness, acoustic neuroma excision, benign positional vertigo, cerebellar signs and left facial droop, optic disk edema and periphlebitis, peripheral visual field loss, and hemifacial spasm.
The primary analysis of the brain consisted of evaluation of the cerebral WM. Smaller regions of interest were drawn for sampling than those in previous studies secondary to our concern for avoiding partial volume averaging with adjacent CSF, gray matter, or lesions. Regions of interest were drawn bilaterally in the anterior, central, and posterior regions of WM at each of 3 consecutive levels, with the most caudal level at the superior aspect of the lateral ventricles. These regions corresponded to frontal, frontal-parietal, and parietal WM. Regions of interest were also drawn bilaterally in the caudate heads, putamina, thalami, posterior internal capsules, and the cerebellar WM (Fig 1). The regions of interest were drawn to avoid areas of FLAIR and DWI lesions. Similar region-of-interest locations were drawn in patients as well as controls. There was a total of 15 regions of interest for which ADC measurements could not be obtained secondary to lesion locations that did not allow for placement of the region of interest in the patients with CNS vasculitis. The average size of the region of interest in the patients with CNS vasculitis was 44.4 mm3.

A, Regions of interest 1, 2, and 3 represent measurements made in the anterior, central, and posterior WM in the corona radiata and centrum semiovale. B, The region of interest positions are represented by 4 for the caudate heads, 5 for the putamina, 6 for the posterior internal capsules, and 7 for the thalami. C, Region of interest 8 is positioned in the cerebellar WM.
The right-sided and left-sided ADC measurements for the 3 levels at which the WM was measured were averaged together for 1 value to represent each WM region—anterior, central, or posterior WM. Similarly, the right-sided and left-sided ADC measurements from the caudate heads, putamina, thalami, posterior internal capsules, and the cerebellar WM were averaged together to obtain 1 measurement for each region.
The ADC analysis was performed by using 2-point ADC calculations.16 Images with b = 0 s/mm2 and b = 1000 s/mm2 were used. ADC maps were generated on an ADW 4.0 workstation (GE Healthcare).
The t test was used to compare the average ADCs for each region-of-interest point measured (anterior WM, central WM, posterior WM, caudate heads, putamina, thalami, posterior internal capsules, and the cerebellar WM) in the vasculitis subjects with those of healthy controls. A Bonferroni correction was used, making a P value of < .00625 significant.
Results
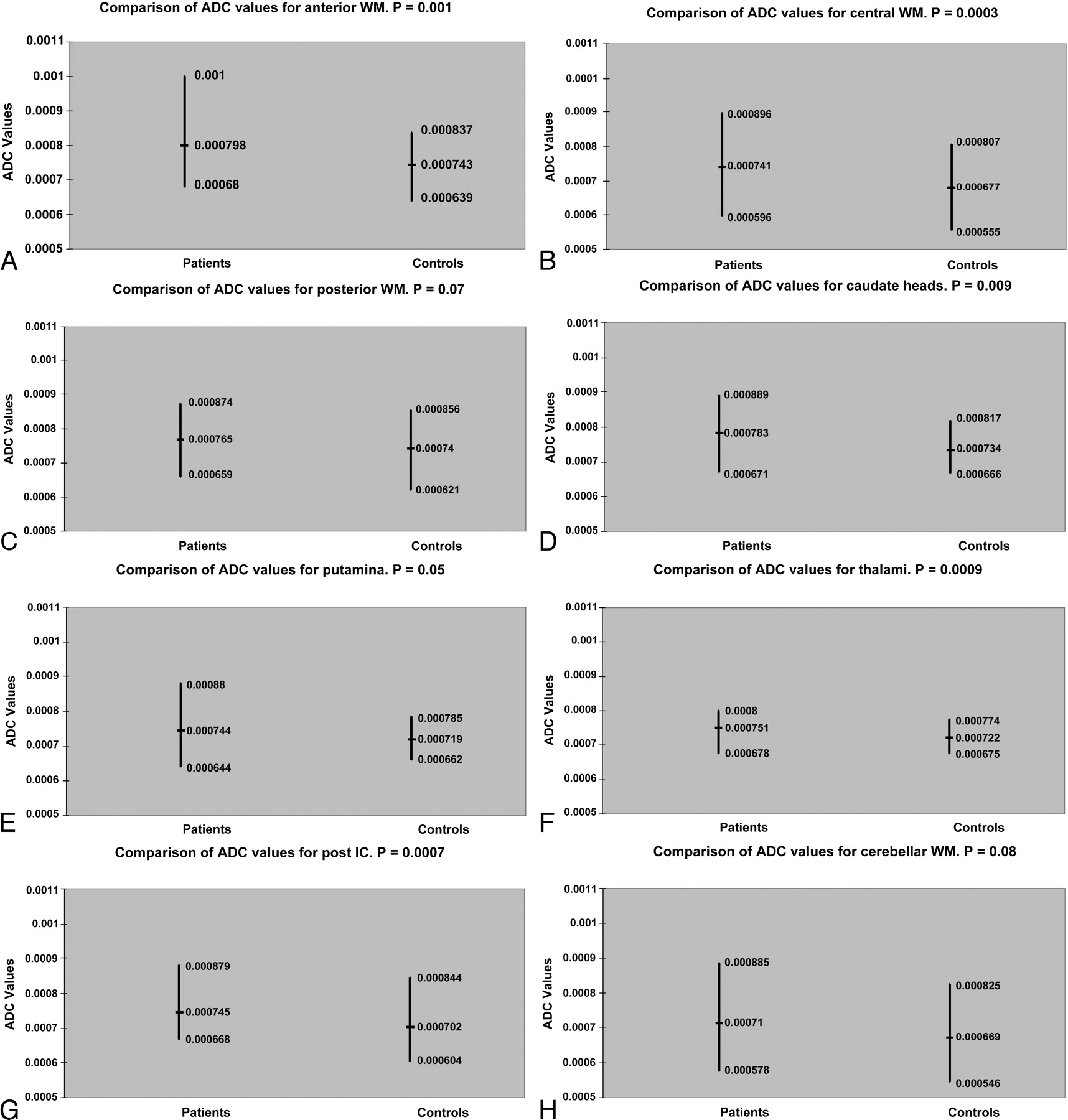
The ADC values in the normal-appearing brain of the patients are summarized in the Table. There was a significant increase in the ADC values (P < .00625) for the anterior WM, central WM, thalami, and posterior internal capsules (Fig 2). In patients 4 and 5, DWI and FLAIR showed no abnormal findings. Both patients overall demonstrated mild-to-moderate elevation of ADCs compared with the average values of the controls. There were 9 patients with lesions seen on DWI and 12 patients with lesions seen on FLAIR. Only 2 patients demonstrated more lesions on DWI than on FLAIR. There was a total of 75 DWI lesions and 150 FLAIR lesions.

Comparison of the ADC values (square millimeters per second) between the patients with vasculitis and the healthy controls for anterior WM (WM, A), central WM (B), posterior WM (C), caudate heads (D), putamina (E), thalami (F), posterior internal capsules (post IC, G), and cerebellar WM (H). There is a significant increase in the ADC values (P < .00625) for the anterior WM, central WM, thalami, and post IC in the patients with vasculitis. The horizontal lines indicate the mean ADC values in each group.
ADC in the nonlesional brain of patients
Discussion
Diagnosing CNS vasculitis continues to be a clinical and radiographic challenge. It has been shown previously that MR imaging findings in CNS vasculitis can be negative when abnormalities are present at cerebral angiography.4–7 Conventional MR imaging findings may even be negative in cases of pathologically proved vasculitis.17 Also, angiography and biopsy findings can be negative in patients who have CNS vasculitis.1, 3, 4, 7, 17–19 This demonstrates the need for a noninvasive test that can detect abnormalities that may be missed by conventional MR imaging, and even angiography and biopsy. This noninvasive test could potentially be beneficial for both diagnostic and prognostic purposes.
DWI uses a contrast mechanism—water diffusivity—that is unique and quantifiable.9 This uniqueness of the contrast mechanism allows DWI to demonstrate brain changes that routine MR imaging misses. ADCs increase when water motion increases. However, increased diffusion is a nonspecific finding that can be the result of several mechanisms. DWI with ADC analysis has demonstrated the ability to detect subtle changes throughout the brain. Increased ADC values for normal-appearing brain have been found in multiple sclerosis, tuberous sclerosis, Behcet disease, NF1, and the aging brain.10–14 Applying ADC analysis to evaluate the brain in patients with CNS vasculitis may reveal otherwise undetectable changes.
Our results demonstrate that diffuse changes do occur in the normal-appearing brain in patients with CNS vasculitis. The ADCs were increased throughout the WM of the corona radiata and centrum semiovale, the thalami, and the posterior internal capsules. The ADC analysis of the brain helped to elucidate the extent of abnormalities that occur in CNS vasculitis. This study demonstrated the ability of ADC measurements to detect brain changes that have not been previously noted.
The ADC analysis of the normal-appearing brain may be potentially useful in the diagnostic work-up of patients with suspected CNS vasculitis, given that conventional MR imaging findings may be negative in patients with CNS vasculitis.4–7 For example, normal MR imaging findings but an abnormality of normal-appearing brain in a patient with suspected CNS vasculitis may be strong evidence for pursuing a more invasive diagnostic test such as brain biopsy. This question needs further evaluation. Even of greater interest would be the possibility that a noninvasive test could help make the diagnosis of CNS vasculitis, and a brain biopsy could be avoided. However, it would be surprising if ADC analysis of the normal-appearing brain in patients suspected of having CNS vasculitis could fulfill that role, given the nonspecific meaning of increased ADCs.
We can only hypothesize the meaning of diffuse abnormalities detected by ADC analysis. We would conjuncture that they potentially represent diffuse vasogenic edema, brain destruction (axonal loss), wallerian degeneration, or vascular changes directly due to the vasculitic process. In patients with CNS vasculitis, diffuse pathologic changes in the brain parenchyma include loss of nerve cells, abnormal nerve cells, perivascular lakes of eosinophilic material, and foci of vacuolation.20 Changes have been found widespread throughout the white and gray matter.20 At autopsy, diffuse changes of edema, reactive astrocytosis, ischemic change, and hemorrhage have been found.21 The changes in the posterior internal capsules and the thalami in particular could be due to wallerian degeneration secondary to the WM tracts of which they consist (the posterior internal capsules) or the numerous WM connections within them (the thalami).
CNS vasculitis is a relatively rare disorder, and this resulted in the number of cases in our series being small. However, given the rarity of the disease, we believe the number of patients in our series is respectable. Not all of our cases are from the same MR imaging scanner, and this may result in an unanticipated bias that we may not have corrected even though we matched our healthy controls by the MR imaging scanner used in the patients with vasculitis. We did use the same b value for all diffusion studies (b = 1000). Most of our cases were not pathologically proved, but it has been shown that biopsy can be negative in patients who have CNS vasculitis.17, 19 We were limited in biopsy material available to confirm the diagnosis of CNS vasculitis secondary to the clinical methodologies used at our institution to make the diagnosis of vasculitis.
Conclusion
We detected changes by ADC analysis of the normal-appearing brain in patients with CNS vasculitis. Further analysis of patients with CNS vasculitis is needed to determine if this information can be used to predict patient diagnosis, acute clinical outcome, or long-term disability.
References
- Received April 24, 2006.
- Accepted after revision October 5, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.