
Abstract
BACKGROUND AND PURPOSE: Patients infected with human immunodeficiency virus (HIV) are susceptible to cognitive deterioration. This study investigated the utility of magnetization transfer (MT) imaging for quantification of brain tissue alterations associated with cognitive deficits in patients with HIV.
MATERIALS AND METHODS: MT ratios (MTR) were derived for whole brain and for regions of interest (ROIs) in the basal ganglia and white matter in 11 HIV and 12 control subjects. Relationships with severity of cognitive impairment and specific neuropsychological deficits were also evaluated.
RESULTS: MTR values for normalized whole brain histogram peak height, whole brain histogram mean, and all examined ROIs were reduced in the HIV subjects. Normalized histogram peak height and mean for whole brain, as well as means for the corpus callosum, basal ganglia, and frontal white matter (FWM), were significantly correlated with severity of cognitive impairment. MTR values for white matter regions (corpus callosum, FWM, and centrum semiovale) were correlated with specific cognitive deficits.
CONCLUSION: Quantitative MTR measurements, determined for the whole brain and for vulnerable ROIs, are sensitive to neuropathologic changes associated with cognitive impairment in HIV-infected patients.
Human immunodeficiency virus (HIV)-associated cognitive impairment involves behavioral, motor, and neuropsychological deficits that may eventually progress to dementia.1 Cognitive deficits are secondary to brain injury in response to proinflammatory cytokines, chemokines, and neurotoxic HIV viral proteins (eg, gp120).2,3 Microscopic pathologies include inflammatory infiltrates, myelin pallor, dendritic simplification, and neuronal loss.4,5 Injury is prominent in the basal ganglia and deep white matter, and the pattern of cognitive deficits is consistent with subcortical dementia.1,4,6 Conventional MR imaging findings in patients with HIV, however, have limited prognostic significance for histopathologic and clinical neuropsychological outcome.7
Magnetization transfer (MT) imaging is a noninvasive quantitative MR imaging strategy that has been used to detect subtle or occult alterations in normal-appearing brain tissue in neurologic disorders. The MT effect results from macromolecular proteins and lipids in myelin membranes,8,9 which are undetectable on conventional T1- and T2-weighted brain images because their signal intensity decays rapidly. MT selectively saturates the macromolecular-bound protons to strategically probe tissue integrity at the microstructural level.10 The MT ratio (MTR) is computed on the basis of the difference of 2 serial images; 1 with MT saturation and 1 without. MT can be used to quantify pathologic changes in macromolecules due to tissue injury and destruction. This noninvasive strategy has been used to identify injury in various neurologic pathologies, including HIV encephalitis.11–16
An advantage of MT is the possibility of acquiring measurements of the brain at different levels of analysis. This strategy can be used to derive quantitative MTR measurements for the whole brain as well as for localized regions of interest (ROIs). In patients with HIV, the whole brain histogram MTR, a putative measure of remaining normal tissue, is reduced17,18 and is significantly correlated with severity of cognitive impairment and psychomotor losses.18 However, MT measurements for localized regions and the relationship of these measurements to specific cognitive deficits have not been systematically investigated in patients with HIV, to our knowledge. MT measurements, acquired in vulnerable subcortical brain regions, may be more sensitive to subtle localized tissue damage and may better correlate with cognitive deficits in patients with HIV. The purpose of this study was to derive MT measurements in the basal ganglia and deep white matter to evaluate relationships with the deficits characteristic of HIV-associated cognitive deterioration. In addition, several whole brain MT indices were assessed.
Materials and Methods
Participants
Eleven HIV-seropositive subjects (mean age, 49.4 ± 7.27; 9 men and 2 women) participating in an investigation of the natural history of neurologic impairment in advanced HIV infection19 were included. Control subjects included 12 seronegative volunteers without a history of neurologic illness (mean age, 43.0 ± 10.36; 10 men and 2 women). Demographic variables were compared in the 2 groups, and no significant difference was found, though the HIV subjects (47.0 ± 7.27) were older on average than control participants (43.0 ± 10.36). There were also no significant differences between the groups in years of education (15.5 ± 2.4 versus 15.5 ± 2.7).
Study exclusion criteria were chronic neurologic disorders, current or past opportunistic central nervous system (CNS) infection, psychosis at study entry, schizophrenia, history of head injury, or chronic neurologic disorders. All HIV subjects were receiving antiretroviral therapy. Clinical assessments of the HIV subjects included the macroneurologic examination created by the AIDS Clinical Trials Group and the motor portion of the Unified Parkinson's Disease Rating Scale, used to assess extrapyramidal signs. The neuropsychological examination evaluated working memory; verbal memory; visual memory; constructional ability; and psychomotor, motor speed, and frontal/executive systems on the basis of composites of individual subtests included in the battery. The severity of cognitive impairment was determined on the basis of criteria defined by the Memorial Sloan-Kettering (MSK) rating scale,20 operationalized for uniform staging across multiple research sites.21,22 The operationalized MSK scoring takes into account the presence of CNS abnormalities on examination; the results of the neuropsychological testing; and the degree of impairment in work, self-care, and mobility status reported by the patient. A reported deficit in at least 1 of the 8 instrumental activities of daily living is required to meet the minimal functional criterion for MSK staging. The derivation of the cognitive domain measures and the operational definitions of the severity of cognitive impairment ratings have been described in more detail in prior reports.21,22 MSK scores for the HIV subjects ranged from 0.5 to 2 versus 0–0.5 for healthy controls. CD4 counts for the HIV subjects ranged from 24 to 427; plasma viral load ranged from undetectable to 154,938 copies/mL. The investigation was conducted with approval from the institutional review board.
MR Imaging and Image Processing
MT imaging was performed with a fast gradient-echo sequence by using a low flip angle (20°) and a TR of 1000 ms to achieve minimal T1-weighting. Twenty-four contiguous 7-mm axial sections covering the entire brain were used for the MT scans. In-plane resolution was 0.9375 × 0.9375 mm2. The sequence was run twice, once preceded by an off-resonant saturation pulse (MS) and once without the saturation pulse (M0). The frequency offset of the saturation pulse was 1200 Hz, and its duration was 16 ms. Identical prescanning settings (center frequency, shim parameters, transmit gain, and receiver gain) were maintained between the 2 acquisitions. Other conventional imaging acquisitions included T2- and proton attenuation–weighted spin-echo sequences. Quantitative image analysis was performed off-line. The whole brain histogram analysis was performed by using customized image processing software written in Matlab (Mathworks, Natick, Mass). Maps of the MTR were obtained by using the relation,  where MS and M0 are the signal intensities in a given voxel obtained with and without the MT saturation pulse. The background noise, skull, extracranial tissues, and CSF were segmented out. The MTR histogram (Fig 1A) was produced to obtain the normalized peak height, peak site, and mean MTR. The peak height of the histogram was divided by the number of voxels of brain parenchyma to normalize head size variation and atrophy. MTR measurements for the ROIs were determined by using an Advanced Workstation (GE Healthcare, Milwaukee, Wis). The ROIs were placed by a radiologist who was blinded to the clinical and cognitive status of the subjects. MT color maps were computed by using the previously mentioned relation with the color spectrum indicating the range of MTR values. Mean MTR was determined by averaging the MTR of pixels in the ROI. Uniform-sized (33 ± 3 mm2) ROIs were positioned on the MT raw images. The MTR color maps were used to constrain ROI placement. Partial volume artifact, shown as a rim (Fig 2) surrounding ventricular CSF (in green), was avoided. The centrum semiovale was identified 1 section above the ceiling of the bilateral ventricles by using the MTR color map to rule out possible CSF contamination. The mean MTR was acquired for ROIs in the corpus callosum (genu and splenium), FWM, centrum semiovale, caudate, putamen, and thalamus (Fig 2A). Routine visual inspection of the images indicated the atrophic changes, some punctate focal hyperintensities, and diffuse subtle hyperintensities on T2- and proton attenuation–weighted MR imaging that have been described in previous MR imaging studies of patients infected with HIV.7 ROIs were not specifically placed on focal lesions. For the studied regions, the intraoperator reproducibility determined for 10 healthy controls ranged from 0.85 to 0.99 (intraclass correlation coefficients).
where MS and M0 are the signal intensities in a given voxel obtained with and without the MT saturation pulse. The background noise, skull, extracranial tissues, and CSF were segmented out. The MTR histogram (Fig 1A) was produced to obtain the normalized peak height, peak site, and mean MTR. The peak height of the histogram was divided by the number of voxels of brain parenchyma to normalize head size variation and atrophy. MTR measurements for the ROIs were determined by using an Advanced Workstation (GE Healthcare, Milwaukee, Wis). The ROIs were placed by a radiologist who was blinded to the clinical and cognitive status of the subjects. MT color maps were computed by using the previously mentioned relation with the color spectrum indicating the range of MTR values. Mean MTR was determined by averaging the MTR of pixels in the ROI. Uniform-sized (33 ± 3 mm2) ROIs were positioned on the MT raw images. The MTR color maps were used to constrain ROI placement. Partial volume artifact, shown as a rim (Fig 2) surrounding ventricular CSF (in green), was avoided. The centrum semiovale was identified 1 section above the ceiling of the bilateral ventricles by using the MTR color map to rule out possible CSF contamination. The mean MTR was acquired for ROIs in the corpus callosum (genu and splenium), FWM, centrum semiovale, caudate, putamen, and thalamus (Fig 2A). Routine visual inspection of the images indicated the atrophic changes, some punctate focal hyperintensities, and diffuse subtle hyperintensities on T2- and proton attenuation–weighted MR imaging that have been described in previous MR imaging studies of patients infected with HIV.7 ROIs were not specifically placed on focal lesions. For the studied regions, the intraoperator reproducibility determined for 10 healthy controls ranged from 0.85 to 0.99 (intraclass correlation coefficients).

A, In MTR histograms, the normalized whole brain peak for patients with HIV is lower and shifted to the left, demonstrating significantly reduced MTR value compared with that of control subjects. AU indicates arbitrary unit; asterisk, P < .05. B, Whole brain mean MTR and peak site for HIV and control subjects. Asterisk indicates P < .05; double asterisks, P < .01.

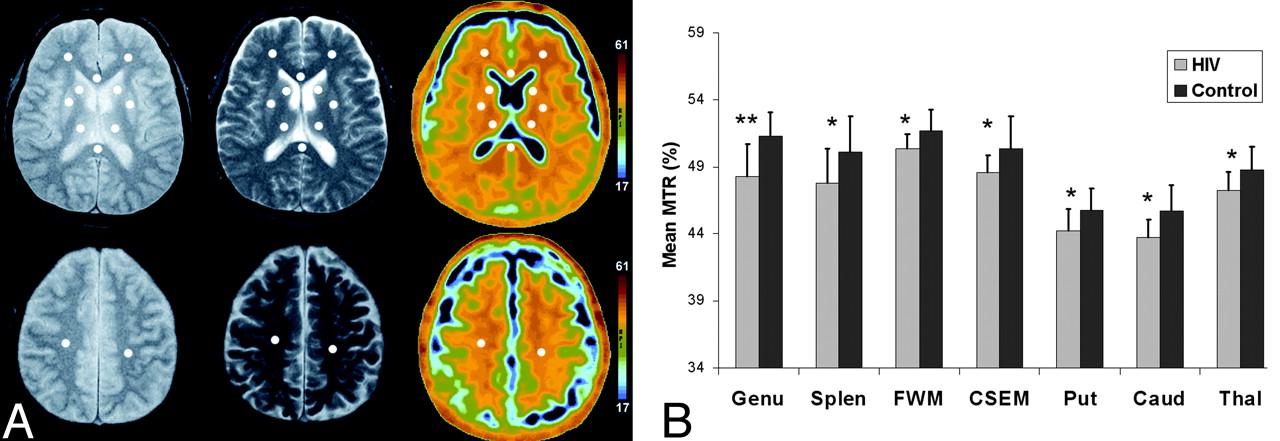
A, ROIs. From left to right, MT without saturation, MT with saturation, and MTR color maps. B, Group comparisons of the HIV and controls for the studied ROIs. Splen indicates splenium; CSEM, centrum semiovale; Put, putamen; Caud, caudate; Thal, thalamus; asterisk, P < .05; double asterisks, P < .01.
Statistical Analysis
Primary dependent measures included the MTR measures calculated for the whole brain and for specific ROIs. The quantitative MR measurements were compared in HIV and control subjects and examined for patterns of relationship to the severity of cognitive impairment and deficits in specific cognitive functions. Statistical methods included analysis of variance, independent t test, summary statistics, Pearson correlation coefficients (for ratio-scaled variables), and Spearman correlation coefficients (for ordinal-scaled clinical ratings). All statistical tests were 2-tailed and were executed in SPSS by using a significance level of .05 (SPSS, release 12.0; Chicago, Ill). Multiplicity was corrected by using the false discovery rate (FDR) controlling procedure.23
Results
We calculated 3 whole brain MTR parameters: histogram mean, normalized peak height, and peak site. Each of these whole brain measurements was compared in the groups by using analysis of variance with age entered as a covariate. There were significant differences between the groups for the histogram mean (F(1,20) = 6.82; P = .017) and the normalized peak height (F(1,20) = 5.89; P = .025). The ROI measurements for white matter (centrum semiovale, genu, splenium, and FWM) and gray matter (basal ganglia, including the caudate and putamen) were evaluated simultaneously by using repeated measures analysis of variance with age entered as a covariate. Significant main effects for the group were obtained for both white matter (F(1,20) = 6.13; P = .02) and for gray matter (F(1,20) = 4.33; P = .05). Further analyses examined differences between the groups for individual regions. For white matter, this analysis indicated significantly lower MTR values in the patients with HIV for the genu (t(21) = −3.43; P = .003), splenium (t(21) = −2.19; P = .04), FWM (t(21) = −2.42; P = .025), and centrum semiovale (t(21) = −2.22; P = .037). For gray matter regions, the MTR measurements were significantly reduced in the HIV subjects in the putamen (t(21) = −2.28; P = .033), caudate (t(21) = −2.77; P = .011), and thalamus (t(21) = −2.40; P = .026). The whole brain and localized MTR results are presented in Figs 1 and 2B.
MTR Correlations with Severity of Cognitive Impairment MSK Rating Scale Criteria
For the whole brain MTR, the histogram mean (ρ = −0.64; P = .003) and normalized histogram peak height (ρ = −0.57; P = .011) (Fig 3A) were significantly correlated with the ordinal scaled MSK severity of cognitive impairment ratings (Table). For the localized MTR measurements, significant correlations with the dementia rating (ordinal-scaled MSK) were identified for the genu (ρ = −0.61, P = .002), splenium (ρ = −0.53, P = .009), FWM (ρ = −0.46; P = .03) (Fig 3B), putamen (ρ = −0.51; P = .027), and thalamus (ρ = −0.51; P = .026) (Fig 3C).

Scatterplots of significant correlations between MTR measurements and cognitive status measures, including the MSK ordinal-scale dementia rating (A–C) and continuous cognitive function variables (D–F).
Correlations of MTR measurements and cognitive status measures
MTR Correlations with Cognitive Deficits
Evaluation of relationships between the localized MTR measurements and specific cognitive deficits (Table) indicated significant correlations between reduced MTR in white matter and visual memory (genu: r = 0.48, P = .03; splenium: r = 0.48, P = .03; centrum semiovale: r = 0.46, P = .04) (Fig 3D), visuoconstruction (genu: r = 0.49, P = .03; centrum semiovale: r = 0.54, P = .01; FWM: r = 0.56, P = .01) (Fig 3E), and motor speed (splenium: r = 0.54; P = .02) (Fig 3F). There were no significant relationships between the studied cognitive deficits and MTR measurements for whole brain or for gray matter regions (Table).
MTR Correlations with Markers of Systemic Disease
MTR measurements for the splenium were significantly correlated with higher levels of plasma HIV ribonucleic acid (RNA) (r = −0.71; P = .015). No other significant relationships were identified, however, between the whole brain or localized MTR measures and either CD4+ count or the plasma level of HIV RNA (copies/milliliter) in the patients with HIV.
Discussion
This study evaluated MTR measures for detecting HIV-induced brain damage and correlations with cognitive deficits. The principal advantage of whole brain measurements is to summarize aggregate injury owing to diffuse and/or heterogeneous pathologic processes. Of the 3 whole brain parameters examined, both the histogram mean and normalized peak height were significantly reduced in patients with HIV, and these measures were significantly correlated with the severity of cognitive impairment. These findings are consistent with evidence of reduced whole brain peak height measured in the normal-appearing brain parenchyma of patients with HIV17 and of reduced average mean MTR across multiple discrete white matter regions.15 MT studies of other CNS disorders also support the utility of MT for detecting brain changes associated with clinical and neuropsychological outcome.13,14,24,25 For example, global disease burden, as detected by whole brain MTR, is correlated with cognitive function in multiple sclerosis (MS).26,27 A previous study in cognitively impaired HIV subjects indicates a relationship between whole brain MT measures and overall cognitive decline in HIV-infected subjects.18 Through examining additional whole brain parameters, this study provides further support for the prognostic significance of MT with respect to cognitive status.
Quantitative MTR also makes possible the noninvasive study of discrete brain regions and lesions. Localized brain measurements are important in behavioral neurology studies because alterations occurring in specific regions are associated with characteristic neurologic deficits.28 Changes measured in vulnerable brain regions may be more sensitive to early brain injury and more closely related to subtle signs of deterioration in specific cognitive functions. MT studies in other CNS pathologies have also identified alterations in localized regions and relationships with cognitive outcome. MT studies have demonstrated abnormalities in otherwise normal-appearing brain regions in subjects with MS.13,29,30 Localized MTR alterations have been associated with cognitive status in subjects with mild cognitive impairment and with Alzheimer disease.16,25 Information concerning the sensitivity of MT to localized brain alterations in patients with HIV is very limited, and available information was acquired before widespread use of highly active antiretroviral therapy (HAART).15,31 This investigation evaluated localized MT measurements in regions in which injury has been identified by postmortem studies of HIV encephalopathy, the pathologic correlate of dementia.5,32 MTR values were significantly reduced in HIV subjects in all brain regions studied, including the basal ganglia (putamen, caudate, and thalamus) and white matter (genu, splenium, FWM, and centrum semiovale). These findings support the sensitivity of MT to localized neuropathologic changes in HIV-infected subjects.
The localized MT measurements were also significantly correlated with cognitive status. MTR values for the corpus callosum (genu and splenium), FWM, and the basal ganglia (putamen and thalamus) were significantly correlated with severity of cognitive impairment, as determined by a clinical dementia scale.20 Relationships with specific cognitive deficits, determined by neuropsychological testing, were generally more pronounced for white matter regions. Most notably, reduced MTR measurements in the corpus callosum were significantly correlated with motor speed (splenium), visual memory (splenium), and visuoconstruction (genu). Alterations in the corpus callosum have also been identified in HIV-infected subjects with diffusion tensor imaging,33–35 and these changes correlate with the severity of cognitive impairment and motor function.34,35 Structural studies indicate thinning of the corpus callosum in patients with HIV.36 It has been suggested that the vulnerability of the corpus callosum to injury in HIV dementia has not been adequately recognized, and this brain region may be an HIV predilection site.37 Moreover, only MTR measurements for the splenium of the corpus callosum were significantly correlated with higher levels of plasma HIV RNA. Taken together, these findings suggest that quantitative MR imaging measurements acquired in the corpus callosum may be informative in studies of HIV-associated cognitive impairment.
The localized MTR measurements also indicated significant alterations in the basal ganglia, including the caudate, thalamus, and putamen. Moreover, MTR measurements for the thalamus and putamen were significantly correlated with the severity of cognitive impairment. The basal ganglia have been implicated in cognitive deterioration in HIV-infected patients by histopathologic findings at autopsy.1 MR spectroscopic and positron-emission tomography (PET) studies have found abnormal hypermetabolism in basal ganglia regions in patients with HIV dementia.38,39 Measurements of the basal ganglia acquired with diffusion-tensor imaging demonstrate significant relationships with cognitive and clinical parameters in HIV-infected patients.40 MTR may have considerable practical significance for studying changes in these subcortical gray matter regions. MT affords higher spatial resolution and is easier to implement and less labor-intensive than techniques such as MR spectroscopy and PET. A comparative study of 5 different quantitative MR imaging measures, including total water content, myelin water content, mean T2 relaxation time, T1 relaxation time, and MTR, identified MTR as the most reliable and sensitive for detecting abnormalities in tissue.41
Findings from this investigation indicate that MT is a promising method for summarizing both aggregate and localized neuropathologic changes associated with cognitive deficits in HIV-infected patients. Measurements acquired with MTR, both for whole brain and for selected ROIs, distinguished HIV from control subjects and were significantly correlated with severity of cognitive impairment. MTR measurements in studied white matter regions were correlated with specific cognitive deficits. Findings from this investigation provide further evidence implicating white matter injury in HIV-associated cognitive deterioration. Multifocal-distributed neural networks interconnected by white matter pathways are critical to intact higher order cognitive function.42 The corpus callosum plays a role in visuomotor integration and may interact in important ways with subcortical structures, notably basal ganglia, in response initiation.43 Injury involving the corpus callosum and/or basal ganglia may be reflected in slowed response initiation and longer reaction times on tasks involving hemispheric transfer or integration between regions.
Many neuroradiologic studies, particularly in MS, have found that MT detects subtle changes that are not identified on conventional MR imaging.11–16 However, the technique has not yet been adapted for clinical settings in the management of patients with HIV. Potential clinical applications of MT include early detection of neurologic involvement and response to treatment. In MS, for example, MT measurements have been used to evaluate drug effectiveness44 and have been recommended as objective end points in large-scale MS trials.45 It is possible, pending further study, that MT could be used to detect response to specific antiretrovirals. These measurements may be more sensitive to subtle or short-term changes in status than measures based on clinical evaluation (eg, cognitive symptoms). The patients with HIV in this investigation were all cognitively impaired and were on antiretroviral regimens. Further studies are necessary to determine the potential of localized MTR measurements for detecting neuropathologic changes in asymptomatic stages of infection, for studying the impact of neuroprotective interventions, and for monitoring neurologic progression across the course of HIV infection.
Conclusion
MTR measurements are sensitive to the neuropathologic substrate in patients with HIV. In this investigation, aggregate changes measured with whole brain MTR, as well as localized MTR measurements, demonstrated significant correlations with clinical ratings of overall cognitive function. Specific neuropsychological deficits were more highly correlated with localized MT measurements.
Acknowledgments
We are grateful for the assistance of Linda Pierchala and Linda Reisberg.
Footnotes
This work was supported by NIH grants K23 MH66705 (A.R.) and NS36519 (L.E.), and the National Institute of Mental Health (grants MH66705 and MH63039) and the National Institute of Neurologic Disorders and Stroke (grants NS36519 and NS049465).
Paper previously presented in part at: Annual Meeting of the International Society for Magnetic Resonance in Medicine, May 6–12, 2006; Seattle, Wash.
References
- Received February 21, 2007.
- Accepted after revision April 30, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.