
Article Figures & Data
Figures
- Fig 1.
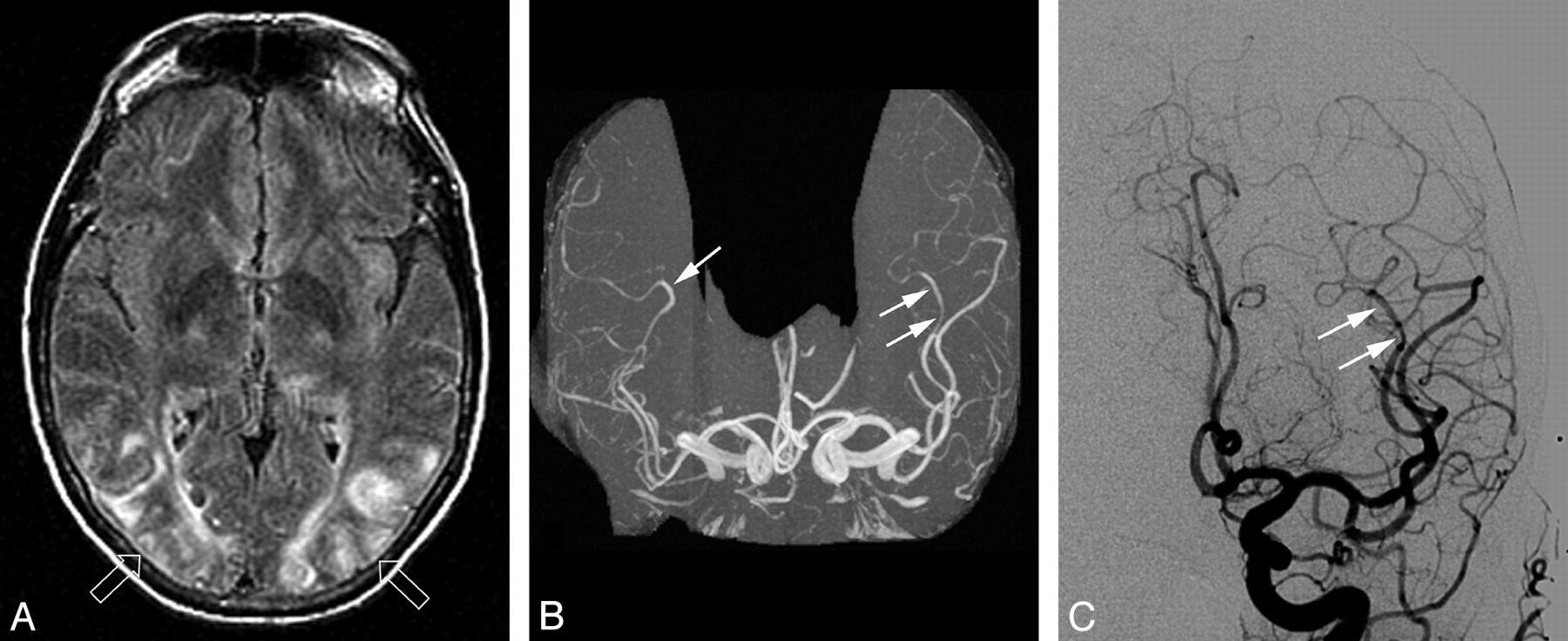
Patient 43 is a 53-year-old woman with a baseline blood pressure of 131/74 mm Hg who was receiving oral and skin patch narcotic pain control for a recently sustained pelvic fracture in a motor vehicle crash. She developed nausea, vomiting, and altered mentation then progressed to generalized seizure with a blood pressure at toxicity of 149/105 mm Hg. A, Axial MR imaging (FLAIR sequence) obtained 1 day after acute toxicity demonstrates vasogenic edema in the occipital region (open arrows) consistent with PRES. Similar areas of vasogenic edema consistent with PRES was present in the frontal and parietal regions (not shown). B, MR angiogram obtained on the same day demonstrates areas of focal vasodilation in the branches of MCA bilaterally with focal vasoconstriction also noted on the left (arrows). C, Frontal view from the left common carotid catheter angiogram obtained the same day demonstrates an identical area of focal vasodilation and vasoconstriction in the branch of the left MCA (arrow). An identical finding was present at angiography in the right MCA consistent with the MRA observation on the right. Similar findings were present on both MRA and CA in the PCA bilaterally (not shown).
- Fig 2.
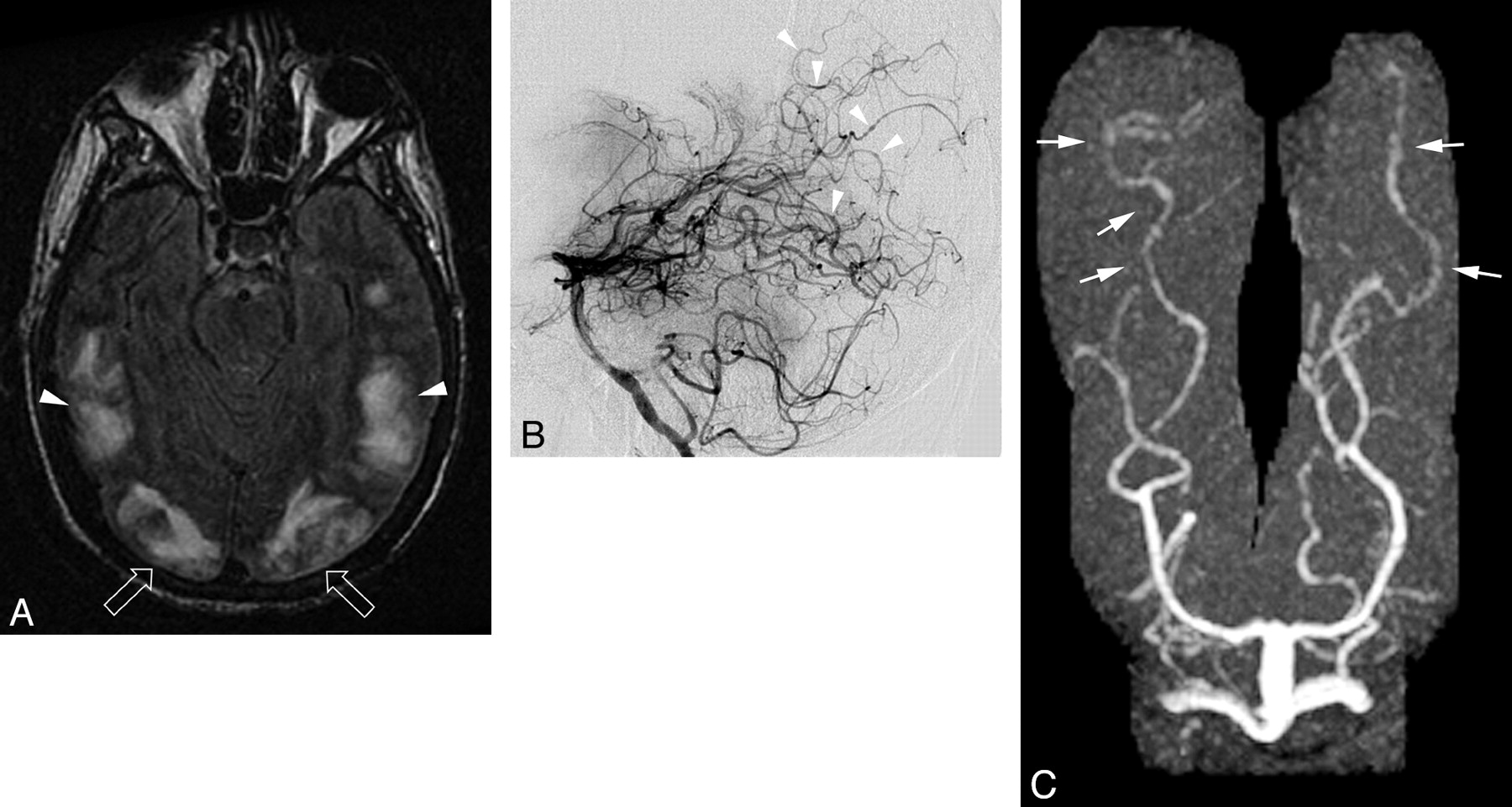
Patient 10 is a 27-year-old man with a history of drug and alcohol abuse with a necrotic pneumonia and empyema growing Pseudomonas and Klebsiella. He developed altered mentation and an asymmetric neurologic examination with blood pressures ranging between 130/77 and 130/100 mm Hg. A, Axial MR imaging (FLAIR sequence) demonstrates extensive vasogenic edema in the occipital lobes (open arrows) and temporooccipital junction (arrowheads) consistent with PRES. Additional extensive areas of vasogenic edema consistent with PRES judged vasogenic edema grade 4 were present in the frontal and parietal lobes (not shown). B, Vertebral catheter angiogram obtained after development of occipital hemorrhage (5 days after initial toxicity) demonstrates areas of vessel narrowing and dilation along with a string-of-bead appearance and areas of focal spasm in parietal and occipital branches of the PCA. Right common carotid catheter angiogram (not shown) also demonstrated extensive vasospasm in branches of the ACA and MCA. C, MR angiogram obtained 5 days after catheter angiogram (10 days after initial toxicity) demonstrates persistent vessel irregularity in the posterior cerebral branches (arrows) with a pattern nearly identical to the appearance of the catheter angiogram. Follow-up MR imaging demonstrated improvement of the extensive vasogenic edema.
- Fig 3.
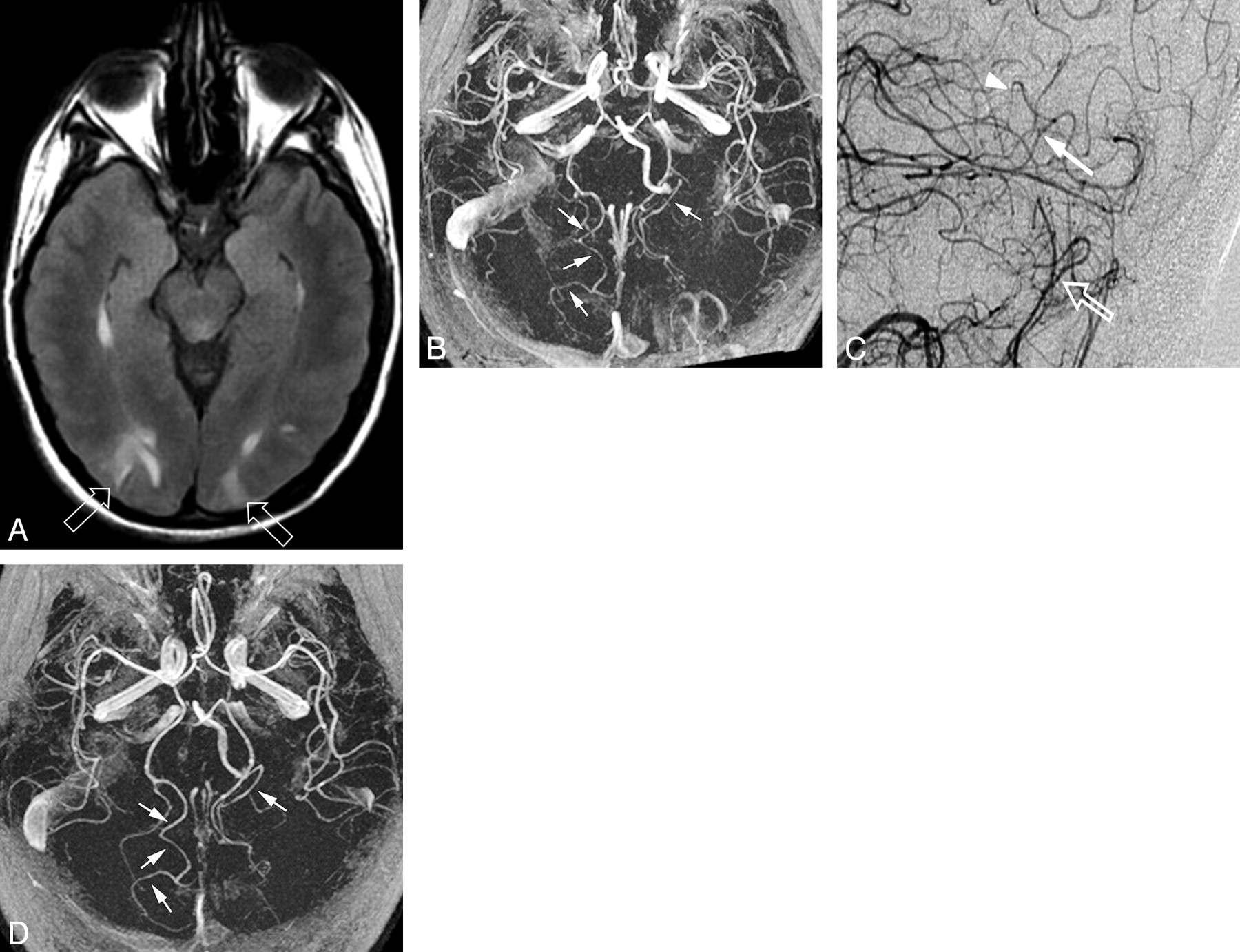
Patient 16 is a 39-year-old woman status post bowel resection and appendectomy for Crohn disease being maintained on antibiotics and steroids with baseline blood pressure of 100/60 mm Hg. Brain imaging was obtained when she developed headache, vertigo, and moderate elevation in blood pressure (145/95 mm Hg). A, Axial MR imaging (FLAIR sequence) results demonstrate vasogenic edema in occipital lobes (open arrows) consistent with PRES. Additional areas of vasogenic edema consistent with PRES were present in the frontal and parietal regions, and abnormality of signal intensity with restricted diffusion was also present in the medial right cerebellar hemisphere (not shown). B, MR angiogram obtained 1 day after toxicity demonstrates marked vessel irregularity in the PCAs bilaterally (arrows), greater on the right than on the left. C, Left vertebral catheter angiogram (selected posterior magnified lateral view) demonstrates a beaded appearance (arrow) and focal vasoconstriction and vasodilation (arrowhead) of right third- and fourth-order branches of the PCA along with a beaded appearance of the branches of the distal medial posterior inferior cerebellar artery on the left (open arrow). D Results of follow-up MR angiogram obtained 3 days after initial study demonstrate normalization of the vessel irregularity and marked improvement in vessel caliber (arrows) consistent with reversal of the vasospasm/arteritis confirmed on conventional angiography. Follow-up MR imaging demonstrated reversal of the PRES pattern.
- Fig 4.
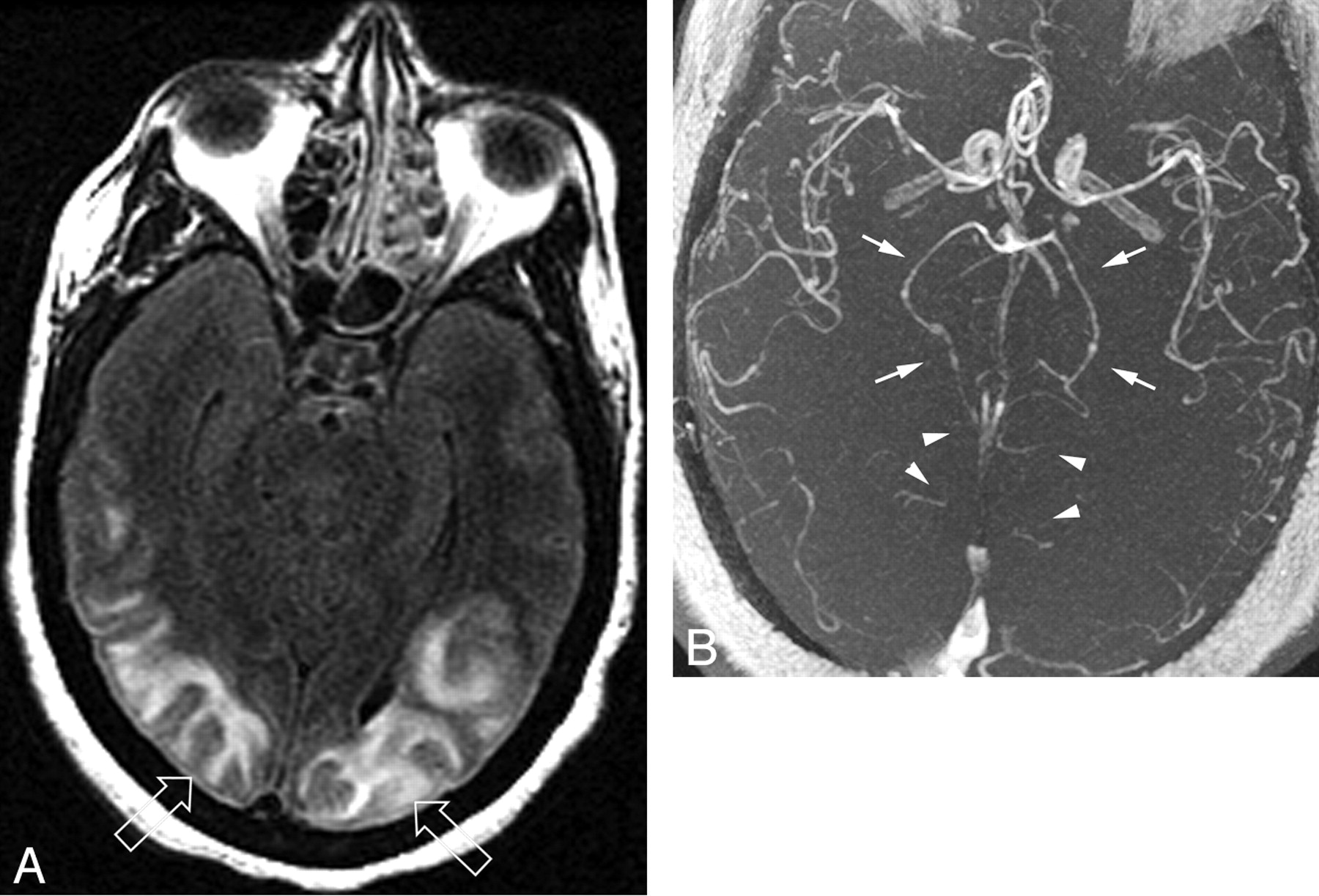
Patient 34 is a 56-year-old woman with long-standing sickle cell disease and a baseline blood pressure of 140/60 mm Hg in a sickle cell crisis with new-onset pneumonia. She developed altered mental status and a seizure with blood pressure at toxicity of 170/110 mm Hg. A, Axial MR imaging (FLAIR sequence) demonstrates typical vasogenic edema in the occipital pole regions bilaterally (open arrows) consistent with PRES and judged edema, grade 3. Occipital lobe rCBV relative to a healthy reference cortex was 63% on the right and 54% on the left. B, Collapsed view of the 3D TOF MRA sequence demonstrates both focal vasospasm (arrows) and pruning of the PCAs bilaterally. Foreshortening of the PCAs and only partial visualization to the midportion of the calcarine arteries are noted bilaterally (arrowheads) and were judged PCA pruning, grade 2. Follow-up MR imaging and MRA (not shown) obtained 1 month after toxicity demonstrated complete resolution of the vasogenic edema in the occipital poles with marked improvement in distal PCA flow bilaterally along with reversal of the pruning and vasospasm.
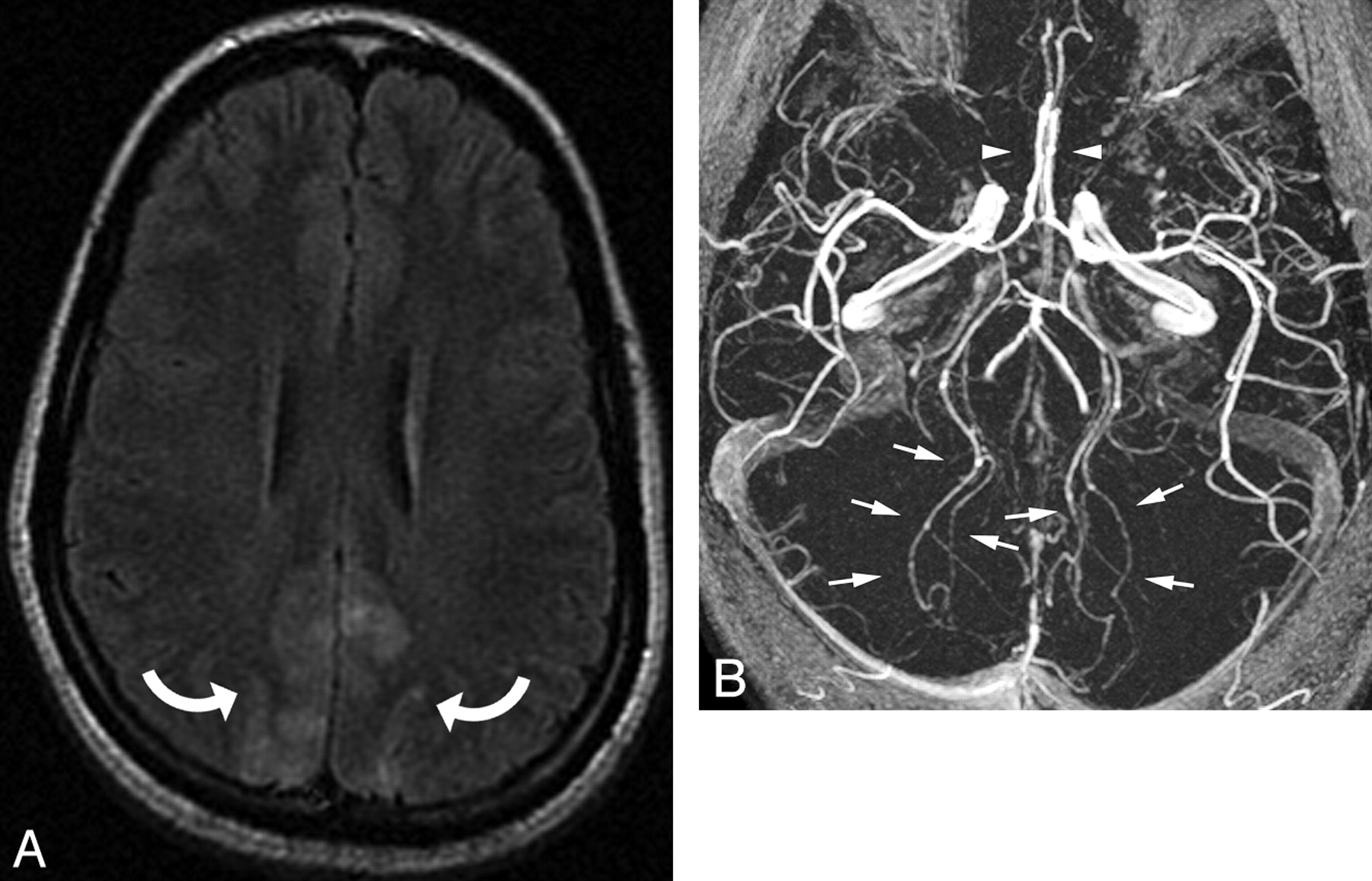
- Fig 5.
Patient 33 is a 23-year-old pregnant woman with baseline blood pressure of 125/75 mm Hg who developed eclampsia. Blood pressure at toxicity was 200/103 mm Hg. A, Axial MR imaging (FLAIR sequence) demonstrates vasogenic edema consistent with PRES in the parietal lobes bilaterally (curved arrows) and was judged edema, grade 1. Vasogenic edema consistent with PRES was also present in the frontal lobes, occipital region, and cerebellum (not shown). B, Collapsed view of the 3D TOF MRA sequence demonstrates PCA spasms bilaterally without PCA foreshortening (arrows) and was judged PCA pruning, grade 1. The ACA spasm present is also partially visible on this collapsed view (arrowheads).
- Fig 6.
Patient 41 is a 34-year-old woman with baseline blood pressure of 104/60 mm Hg who at 33 weeks of pregnancy developed preeclampsia (toxicity blood pressure of 153/102 mm Hg) followed by seizures and status epilepticus. She ultimately required cesarean delivery for seizure control. A, Axial MR imaging (FLAIR sequence) demonstrates typical PRES vasogenic edema in the parietal regions (curved arrows) bilaterally and was judged edema, grade 2. Frontal and occipital involvement was also present bilaterally (not shown). B, rCBV color map demonstrates decreased perfusion in the region of the right parietal lesion (curved arrow). Lesion rCBV was 65% relative to a reference healthy cortex.






Tables
Pruning Grade PCA Distal Visualization* 1 Normal length of the distal calcarine artery to the occipital pole 2 Moderately reduced length of the distal calcarine artery (length halfway between occipital pole and bifurcation with the parieto-occipital artery) 3 Severely reduced length of the calcarine artery (length reduced to the level of the bifurcation with the parieto-occipital artery) Note:—PCA indicates posterior cerebral artery.
* Visualized length of the calcarine artery to the tip of the occipital pole.
Blood Pressure ISS Tx E dE AI Chemo Unk Normotensive 8 2 – 1 – – – Moderate hypertension 1 2 1 1 – – – Severe hypertension 8 5 7 1 5 2 3 Note:—PRES indicates posterior reversible encephalopathy syndrome; ISS, infection, sepsis, and shock; Tx, transplantation; E, eclampsia; dE, delayed eclampsia; AI, autoimmune disease; Chemo, post-cancer chemotherapy; Unk, nonspecific association.
Blood Pressure # pts Overall Features Focal Vessel Features nl P DS # vessels nl Ir (Ir/P) FS (FS/P) Normotensive 10 7 3 – 30 16 12 (6) 2 Moderately hypertensive 5 2 – 3 15 4 4 (2) 7 Severely hypertensive 28 8 2 18 84 13 22 (9) 49 (5) Note:—MRA indicates MR angiography; # pts indicates number of patients; nl, normal; P, pruned; DS, diffuse vasoconstriction; # vessels, number of vessels; Ir, irregularity grade 1; Ir/P, irregular and pruned; FS, focal vasoconstriction/vasodilation grade 2–3; FS/P, focal vasoconstriction/vasodilation and pruned.
- Table 4:
Correlation of MRA pruning grade (PCA-calcarine artery) vs vasogenic edema: 28 patients with severe hypertension (MAP-136)
Vasogenic Edema PCA/Calcarine Artery Pruning Grade Grade 1 Grade 2 Grade 3 Grade 4 0 1 1 Grade 3 3 1 0 Grade 2 6 4 0 Grade 1 12 0 0 Note:—MRA indicates magnetic resonance angiography; PCA, posterior cerebral artery; MAP, mean arterial pressure.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Intra-Arterial Verapamil Treatment in Oral Therapy-Refractory Reversible Cerebral Vasoconstriction Syndrome
- Posterior reversible encephalopathy syndrome as initial manifestation of autoimmune encephalitis
- RCVS2 score and diagnostic approach for reversible cerebral vasoconstriction syndrome
- Preeclampsia: Association With Posterior Reversible Encephalopathy Syndrome and Stroke
- Controversy of posterior reversible encephalopathy syndrome: what have we learnt in the last 20 years?
- Utility and Significance of Gadolinium-Based Contrast Enhancement in Posterior Reversible Encephalopathy Syndrome
- Cerebral perfusion in stroke-like migraine attacks after radiation therapy syndrome
- Cytotoxic Edema in Posterior Reversible Encephalopathy Syndrome: Correlation of MRI Features with Serum Albumin Levels
- Posterior reversible encephalopathy syndrome: the importance of early diagnosis
- Multimodal Imaging of Reversible Cerebral Vasoconstriction Syndrome: A Series of 6 Cases
- Detection of Microhemorrhage in Posterior Reversible Encephalopathy Syndrome Using Susceptibility-Weighted Imaging
- Thunderclap headache
- Serous Retinal Detachment in Hypertensive Posterior Reversible Encephalopathy Syndrome
- The posterior reversible encephalopathy syndrome: what's certain, what's new?
- Type of Edema in Posterior Reversible Encephalopathy Syndrome Depends on Serum Albumin Levels: An MR Imaging Study in 28 Patients
- Licorice-associated reversible cerebral vasoconstriction with PRES
- Reversible cerebral vasoconstriction syndrome
- Hemorrhage in Posterior Reversible Encephalopathy Syndrome: Imaging and Clinical Features
- Catheter Angiography, MR Angiography, and MR Perfusion in Posterior Reversible Encephalopathy Syndrome