
Abstract
BACKGROUND AND PURPOSE: Internal carotid artery (ICA) aneurysms may present with cranial nerve dysfunction. Therapeutic ICA occlusion, when tolerated, is an effective treatment resulting in improvement or cure of symptoms in most patients. When ICA occlusion is not tolerated, selective endovascular aneurysm occlusion can be considered. We compare recovery of cranial nerve dysfunction in patients treated with selective coil occlusion and with therapeutic ICA occlusion.
MATERIALS AND METHODS: In 16 patients with 17 large or giant (11–45 mm) unruptured ICA aneurysms presenting with dysfunction of cranial nerves (CN) II, III, IV, or VI, selective coil occlusion was performed. From a cohort of 39 patients with ICA aneurysms treated with ICA occlusion and long-term follow-up, we selected 31 patients with aneurysms presenting with cranial nerve dysfunction. Clinical recovery at follow-up from oculomotor dysfunction and visual symptoms was compared for both treatment modalities.
RESULTS: Of 17 aneurysms treated with selective coiling, symptoms of cranial nerve dysfunction resolved in 3, improved in 10, and remained unchanged in 4. In 9 of 17 patients, additional coiling during follow-up was required. Of 31 aneurysms treated with carotid artery occlusion, cranial nerve dysfunction resolved in 19, improved in 9, and remained unchanged in 3. These differences were not significant. There were no complications of treatment.
CONCLUSION: Recovery of ICA aneurysm-induced cranial nerve dysfunction occurs in most patients, both after ICA occlusion and after selective coiling. In patients who cannot tolerate ICA occlusion, selective aneurysmal occlusion with coils is a valuable alternative.
Large and giant aneurysms of the cavernous, ophthalmic, and hypophyseal segments of the internal carotid artery (ICA) frequently present with symptoms of mass effect on the cranial nerves. Compression of the oculomotor nerve (CN III), trochlear nerve (CN IV), or abducens nerve (CN VI) results in ophthalmoplegia and is frequently associated with cavernous sinus aneurysms. Compression of the optic nerve (CN II) results in decreased visual acuity and visual field deficits and is mostly associated with carotid ophthalmic or hypophyseal aneurysms. In general, treatment in unruptured but symptomatic intradural located hypophyseal and ophthalmic aneurysms is indicated to prevent rupture and to alleviate symptoms of mass effect. Treatment of unruptured symptomatic cavernous sinus aneurysms may be indicated to improve cranial nerve function or to discontinue progression of dysfunction.
In patients who can tolerate therapeutic ICA occlusion, this therapy is effective in excluding the aneurysm from the circulation. Symptoms of mass effect resolve or improve in most patients. In addition, endovascular balloon occlusion of the ICA is simple to perform, safe, and inexpensive.1–8 When ICA occlusion is not tolerated, alternative treatments are selective aneurysm occlusion with coils or liquid embolic agent9,10 and bypass surgery preceding occlusion.11 The effect on cranial nerve dysfunction of selective occlusion with coils of ICA aneurysms in general and large and giant aneurysms specifically is poorly understood.12–18 In this study, we assess the clinical evolution of aneurysm-induced cranial nerve dysfunction after selective coil occlusion in 16 patients with 17 unruptured large and giant ICA aneurysms and compare the results with historical data of patients with similar aneurysms and symptoms treated with ICA occlusion.
Patients and Methods
General
At our institution, patients with unruptured large or giant ICA aneurysms presenting with cranial nerve dysfunction are preferably treated with endovascular ICA balloon occlusion. Only in patients who cannot tolerate permanent ICA occlusion, selective coiling or bypass surgery is offered.
Assessment of Cranial Nerve Dysfunction
Oculomotor dysfunction was defined as paresis of CN III, IV, or VI or a combination with diplopia in single or multiple gazes with or without ptosis and pupillary dysfunction.
Optic nerve dysfunction was defined as decreased visual acuity with visual field deficits as assessed with perimetric or confrontation testing.
The criteria for complete recovery of oculomotor dysfunction were no diplopia in all direction of gazes, complete resolution of ptosis, and partial or complete recovery of pupillary reaction. Partial recovery of oculomotor dysfunction was defined as residual diplopia in upward, downward, lateral, or medial gaze with or without normal primary gaze, residual ptosis, and pupillary dysfunction.
The criteria for complete recovery of optic nerve dysfunction were restoration of normal visual acuity and visual field. Residual visual field deficits indicated partial recovery.
Aneurysms Treated With Selective Coiling
Between January 1995 and March 2007, a total of 16 patients with 17 large or giant unruptured ICA aneurysms presenting with dysfunction of CN II, III, IV, or VI were treated with selective occlusion of the aneurysm with coils. There were 14 of 16 patients who did not tolerate ICA test occlusion and 2 patients who had bilateral giant ICA aneurysms. One patient had 1 ophthalmic and 1 cavernous sinus aneurysm both presenting with mass effect and both treated with selective coiling (Fig 1). One patient had bilateral cavernous sinus aneurysms, of which the 1 symptomatic aneurysm was coiled. There were 2 men and 14 women with a mean age of 60.0 years (median age, 57 years; range, 38–81 years). The location of the aneurysm was the carotid cavernous sinus in 7, carotid hypophyseal in 4, and carotid ophthalmic in 6. The size of the aneurysm was a mean of 25.6 mm (median, 25 mm; range, 11–45 mm). Of 17 aneurysms, 9 contained an intraluminal thrombus. All 7 cavernous sinus aneurysms presented with ophthalmoplegia or isolated CN III palsy in 1 patient with associated CN II dysfunction. All ophthalmic aneurysms presented with CN II dysfunction in 1 patient with associated CN III palsy. Of 4 hypophyseal aneurysms, 3 presented with CN II dysfunction and 1 with ipsilateral ophthalmoplegia and contralateral partial CN III palsy (Fig 2).

A 48-year-old woman presenting in 1994 with visual field deficit from a right giant carotid ophthalmic aneurysm and acute left ophthalmoplegia from a left-sided carotid cavernous sinus aneurysm. A, Right ophthalmic aneurysm completely occluded with coils (see coil mesh in C and D). B, Left cavernous sinus aneurysm with intraluminal thrombus. Note additional small middle cerebral artery aneurysm. C, Angiogram 7 days after B shows enlargement of the aneurysm by resolution of intraluminal thrombus. D, Loose coil packing after embolization. Follow-up angiograms 6 to 72 months later showed progressive aneurysmal thrombosis with complete occlusion. E and F, MR imaging after 3 weeks (E) and 18 months (F). At 18 months, the aneurysm is almost completely obliterated. Visual field deficit remained unchanged, and ophthalmoplegia improved to isolated abducens palsy.

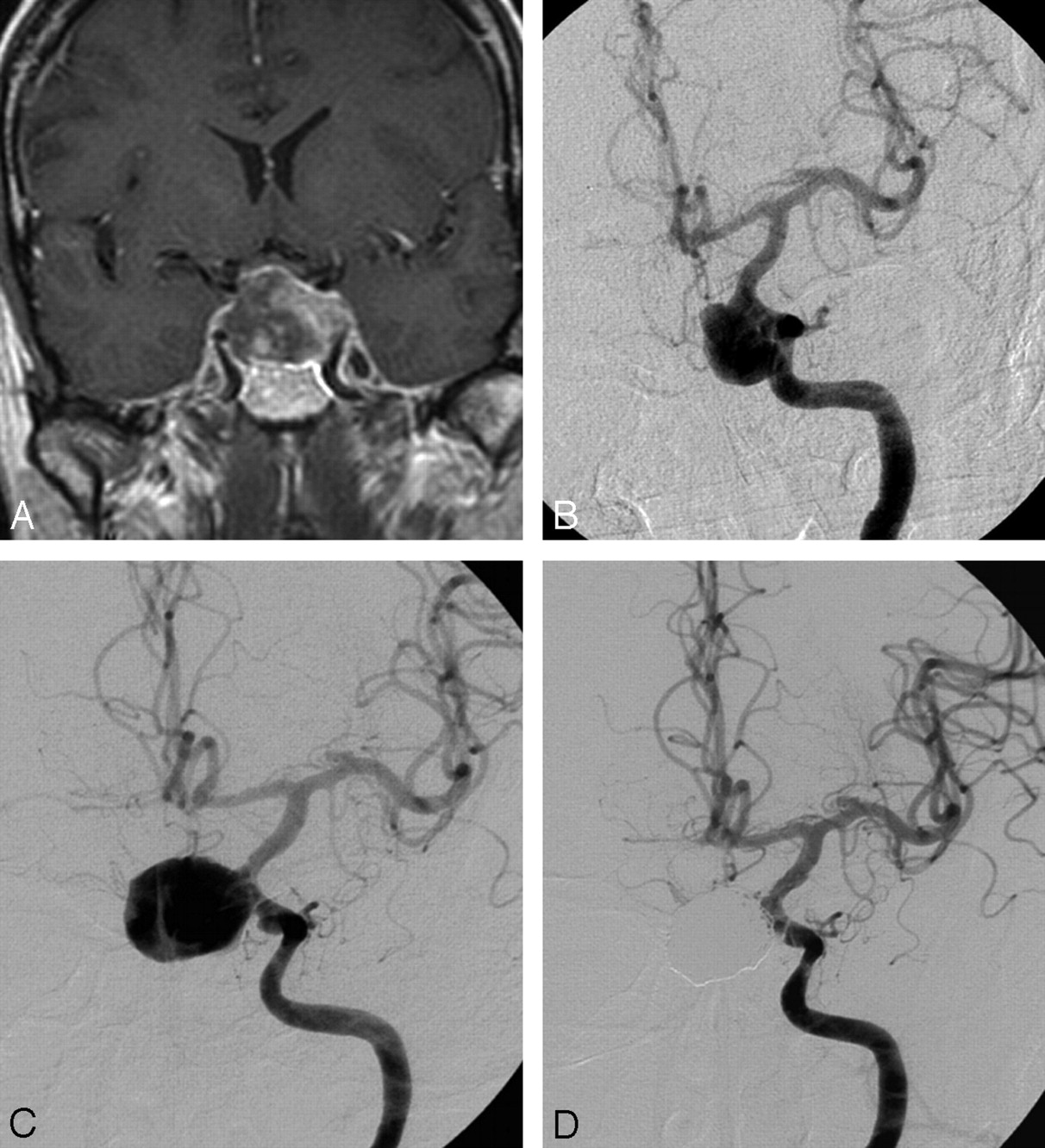
A 52-year-old man presenting with acute ipsilateral ophthalmoplegia and contralateral CN III palsy with intact vision. A and B, Contrast-enhanced MR imaging (A) and angiography (B) shows giant left carotid hypophyseal aneurysm with intraluminal thrombus. Angiographic test occlusion was not tolerated. C, Angiogram 2 days after B shows enlargement of the aneurysmal lumen due to resolution of thrombus. D, Complete occlusion after stent-assisted coiling. One year later, right ophthalmoplegia was resolved. Residual upper gaze diplopia and 1- to 2-mm residual ptosis on the left side.
Five aneurysms were coiled with balloon assistance and 3 after stent placement in primary or additional coiling (Enterprise; Cordis Neurovascular, Miami Lakes, Fla). Coiling was performed with 50-cm long straight coils (Detach 18; Cook, Copenhagen, Denmark) or Guglielmi detachable 18 helical coils (Boston Scientific, Fremont, Calif).
Aneurysms Treated With ICA Occlusion
The protocol for therapeutic ICA occlusion has been described previously.3,6 In short, during balloon test occlusion in the awake patient, angiography of the contralateral ICA or vertebral artery, or both, was performed. Apart from clinical tolerance, synchronous opacification of the cerebral veins in the examined and occluded vascular territory indicated tolerance to permanent occlusion. After tolerance was determined, the ICA was permanently occluded with detachable balloons (Goldvalve #16 balloon; Nycomed, Paris, France or Balt, Montmorency, France). Imaging follow-up consisted of serial MR imaging to evaluate thrombosis and shrinkage of the aneurysm with time.
From a previously published cohort of 39 patients with ICA aneurysms treated with ICA occlusion and long-term clinical and imaging follow-up,4,5 we selected 31 patients with unruptured large and giant aneurysms symptomatic by cranial nerve dysfunction and located in the cavernous sinus (n = 26), and hypophyseal (n = 4) or ophthalmic (n = 1) segment. There were 4 men and 27 women with a mean age of 57.3 years (median age, 55 years; range, 26–78 years). Of 26 patients with cavernous sinus aneurysms, the presenting symptom was ophthalmoplegia in 23 (with additional trigeminal neuralgia in 1) and isolated CN VI palsy in 3. Of 4 patients with hypophyseal aneurysms, 3 presented with CN II dysfunction and 1 with ophthalmoplegia and trigeminal neuralgia. The 1 patient with an ophthalmic aneurysm presented with CN II dysfunction.
Follow-up Assessment
For patients treated with selective coiling, follow-up angiograms were scheduled at 6 months, and additional imaging follow-up (angiography, MR imaging, or MR angiography) was tailored as deemed necessary. When reopening of the aneurysm was apparent at follow-up, additional coiling was performed. For patients treated with ICA occlusion, follow-up imaging consisted of MR imaging at 3 months and at various intervals thereafter.
Recovery from cranial nerve dysfunction was assessed at various intervals during follow-up in the outpatient clinic by neurosurgeons, neurologists, or ophthalmologists. Evolution of aneurysmal size during follow-up after treatment was assessed for patients with serial MR imaging follow-up.
Statistical Analysis
The number of patients with resolved or reduced symptoms of cranial nerve dysfunction for both treatment modalities was compared with patients with unchanged symptoms with the Fisher exact test. The same was done for aneurysms with visual field deficit or oculomotor function as the major presenting symptom.
Results
Aneurysms Treated With Selective Coiling
Initial aneurysmal occlusion after coiling was complete or near complete in all 17 aneurysms. During angiographic follow-up in all patients at a mean of 29.8 months (median, 19 months; range, 6–102 months), 9 aneurysms reopened and were additionally coiled, and 4 of those were coiled for a third time. Final aneurysmal occlusion at last angiographic follow-up was complete or near complete in 16 aneurysms and incomplete in 1 aneurysm. There were no procedural complications leading to permanent morbidity or mortality, neither from primary nor from additional coiling. There were 7 of 16 patients (with 8 aneurysms) who had initial MR imaging and serial MR imaging follow-up, with intervals ranging from 6 to 36 months. Aneurysmal size was unchanged in 6, increased from 19 to 24 mm in 1 (Fig 3), and decreased from 35 to10 mm in 1.

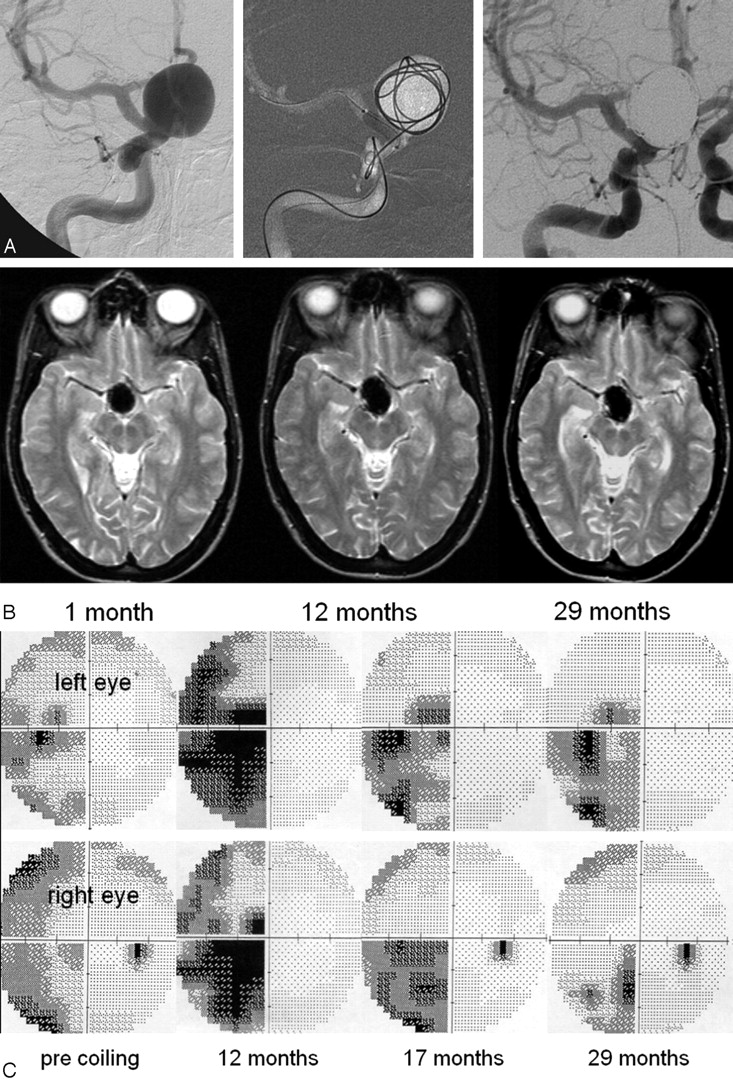
A 38-year-old woman presenting with progressive visual field deficit. A, Giant carotid hypophyseal aneurysm compressing the chiasm treated with balloon-assisted coiling. Angiographic test occlusion was not tolerated. B, MR imaging at 3 intervals after coiling. At 12 months, the aneurysm has increased in size from 24 to 31 mm. Size is stable during an interval of 12 to 24 months. C, Perimetric results before coiling and different intervals thereafter. Incomplete hemianopsia before coiling. At 12 months, increased aneurysmal size caused progressive hemianopsia that gradually decreased at 17 and 29 months. Final result was classified as unchanged.
Clinical follow-up was available in all patients at a mean of 35.3 months (median, 24 months; range, 6–108 months). At last clinical follow-up, on a per aneurysm basis, symptoms of cranial nerve dysfunction resolved in 3, improved in 10, and remained unchanged in 4 aneurysms. Of 9 aneurysms with visual field deficit as the major presenting symptom, this was reduced in 5 and remained unchanged in 4. Of 8 aneurysms with oculomotor dysfunction as the major presenting symptom, this resolved in 3 and was reduced in 5. All 5 patients with incomplete recovery had remaining diplopia in upward or medial gaze, not in primary gaze. Ptosis resolved in all patients.
Aneurysms Treated With Internal Carotid Artery Occlusion
There were no early or late complications of therapeutic ICA occlusion.4–6 At last clinical and MR imaging follow-up at a mean of 31 months (median, 19 months; range, 6–107 months), symptoms of mass effect in 31 patients were resolved in 19, improved in 8, and remained unchanged in 3. Of 4 patients with visual field deficit as the major presenting symptom, this deficit improved in all 4. Of 27 patients with oculomotor dysfunction as the major presenting symptom, this dysfunction resolved in 19, improved in 5, and remained unchanged in 3. All 5 patients with incomplete recovery had remaining diplopia in upward or medial gaze only, not in primary gaze. Ptosis resolved in all patients. In 2 patients with associated trigeminal neuralgia, this resolved in both. For most patients with clinical improvement or resolution, this was obvious in the first year after ICA occlusion. At last MR imaging follow-up at a mean of 31 months, 22 of 31 aneurysms were obliterated completely, 2 aneurysms decreased to 25% of their original diameter; 2 aneurysms, to 50% of their original diameter; and 5 aneurysms, to 75%.
Comparison of Recovery of Cranial Nerve Function in Patients Treated With Selective Coiling Versus ICA Occlusion
Of 17 aneurysms treated with selective coiling, symptoms of cranial nerve dysfunction resolved in 3, improved in 10, and remained unchanged in 4. Of 31 aneurysms treated with carotid artery occlusion, cranial nerve dysfunction resolved in 19, improved in 9, and remained unchanged in 3. These differences were not significant.
Results of recovery of visual field deficit and oculomotor symptoms for both treatment modalities are summarized in the Table. There was no significant difference in improvement or resolution of both types of presenting symptoms, though improvement of visual field deficits occurred more often after ICA occlusion. Complete normalization of visual field did not occur with both treatment modalities.
Recovery of ICA aneurysm-induced oculomotor dysfunction, visual symptoms, and all symptoms after selective coil occlusion in and after ICA occlusion
Discussion
In our study, we found that recovery of cranial nerve dysfunction induced by large or giant unruptured ICA aneurysms occurs in most patients, both after ICA occlusion and after selective coiling. In only 7 of 48 aneurysms, symptoms of cranial nerve deficits remained unchanged after therapy, and aggravation of symptoms did not occur. In our limited patient groups, we were unable to demonstrate a significant difference in alleviation of mass effect between the 2 treatment modalities. This may be explained by the diversity of factors involved in the recovery process: duration of symptoms before treatment; acute or gradual onset of symptoms; degree of cranial nerve dysfunction (complete vs partial); and presence of microvascular risk factors such as hypertension, diabetes, and advanced age. In our patients, the presence and magnitude of these possible factors were not always known. Both coiling and ICA occlusion were safe; complications did not occur. Also, with additional coiling in 9 of 17 aneurysms, there were no complications. The safety of coiling of large and giant aneurysms is supported by previous studies.19–21 In general, in patients with unruptured large or giant ICA aneurysms symptomatic by mass effect, therapy is indicated to reduce symptoms of mass effect and to eliminate the risk for rupture in aneurysms with an intradural location. Both ICA occlusion and selective coiling provide sufficient protection against rupture, with a high chance of improvement of symptoms of mass effect. ICA occlusion is, in our opinion, the treatment of choice because it is effective, safe, definitive, simple to perform, and inexpensive. In patients who cannot tolerate permanent ICA occlusion, alternative treatment should be considered. These alternatives consist of selective occlusion with coils or a liquid embolic agent (Onyx; ev3, Irvine, Calif) or bypass surgery preceding ICA occlusion. The first alternative, selective occlusion with coils, is technically more challenging than ICA occlusion, especially when balloon- or stent-assisted treatment is necessary.22,23 With stent-assisted treatment, prolonged antiplatelet medication is necessary. With currently available easy-to-place stents, feasibility and safety of the stent-assisted technique are enhanced. Imaging follow-up is mandatory because reopening with time occurs in a substantial proportion of patients with large and giant aneurysms, and additional coiling is frequently needed. Recently, filling the aneurysmal lumen with Onyx has been proposed as an alternative treatment.9,10 With this treatment, the neck of the aneurysm is sealed with a balloon in the carotid artery during Onyx injection. In a multicenter study by Molyneux,9 procedure- or device-related permanent neurologic morbidity at final follow-up was present in 8 (8.3%) of 97 patients, with 2 procedural deaths. In large and giant aneurysms, procedural time was lengthy (up to 6 hours). Delayed occlusion of the carotid artery occurred in 9 (9%) of 100 patients. At 12-month follow-up of 53 patients, 38 (72%) large and giant aneurysms were completely occluded. Retreatment was performed in 9 of 79 large and giant aneurysms. Sixteen patients had oculomotor palsies at presentation. At 12-month follow-up, the oculomotor palsy had improved or resolved in 14 patients, remained unchanged in 1 patient, and had worsened in 1. Fourteen patients had optic nerve compression before treatment. At 12-month follow-up, the nerve compression had improved in 6 patients, remained unchanged in 7, and worsened in 1. In our opinion, the high complication rate and high rate of delayed carotid artery occlusion do not justify this treatment in patients with unruptured aneurysms who cannot tolerate carotid artery occlusion. The third alternative to primary carotid artery occlusion is bypass surgery preceding permanent occlusion. High-flow bypass surgery with the excimer laser-assisted anastomosis technique has the advantage of not involving temporary occlusion of the donor or recipient vessel with inherent risks of inducing ischemia. In a study by Brilstra et al,11 short-term outcomes of this technique were evaluated in 77 patients. Of these 77 patients, 10 (13%) had operative complications resulting in dependency in 7 and death in 3. The authors concluded that, in view of this high risk for complications, this technique should be reserved for patients with intradural large or giant aneurysms with a high chance of rupture who cannot tolerate carotid artery occlusion.
Conclusion
For patients with unruptured large or giant carotid artery aneurysms presenting with cranial nerve dysfunction, therapeutic carotid artery occlusion, when tolerated, is the treatment of choice. Clinical results are excellent and complications are exceptional. In patients who cannot tolerate carotid artery occlusion or who have bilateral aneurysms, selective coiling, with or without balloon or stent assistance, is the best alternative with comparable clinical results. Onyx treatment is not justified in view of the high complication rate and high rate of delayed carotid artery occlusion. Bypass surgery should only be considered in patients with intradurally located aneurysms with a high chance of rupture.
References
- Received December 2, 2007.
- Accepted after revision December 20, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Volume variation may be a relevant metric in the study of aneurysm pulsatility: a study using ECG-gated 4D-CTA (PULSAN)
- WEB in Partially Thrombosed Intracranial Aneurysms: A Word of Caution
- Therapeutic Internal Carotid Artery Occlusion for Large and Giant Aneurysms: A Single Center Cohort of 146 Patients
- Intracranial Aneurysms: Wall Motion Analysis for Prediction of Rupture
- The Maze-Making and Solving Technique for Coil Embolization of Large and Giant Aneurysms
- Parent Artery Occlusion in Large, Giant, or Fusiform Aneurysms of the Carotid Siphon: Clinical and Imaging Results
- Flow Diversion Versus Conventional Treatment for Carotid Cavernous Aneurysms
- The 'one and a half round microcatheterization technique' for stent-assisted coil embolization of intracranial aneurysm: technical case series
- Unruptured Carotid Artery Aneurysms Presenting with Symptoms of Mass Effect: Outcome after Selective Coiling, Parent Vessel Occlusion, and Flow Diversion
- Resolution of Mass Effect and Compression Symptoms following Endoluminal Flow Diversion for the Treatment of Intracranial Aneurysms
- Flow Diverters for Unruptured Internal Carotid Artery Aneurysms: Dangerous and Not Yet an Alternative for Conventional Endovascular Techniques
- Endovascular Treatment of Cavernous Sinus Aneurysms
- Partially Thrombosed Intracranial Aneurysms Presenting with Mass Effect: Long-Term Clinical and Imaging Follow-Up after Endovascular Treatment
- Balloon test occlusion and endosurgical parent artery sacrifice for the evaluation and management of complex intracranial aneurysmal disease
- Endovascular Treatment of Large and Giant Aneurysms