
Abstract
SUMMARY: Opitz syndrome is a rare autosomal recessive disorder of cholesterol metabolism associated with mental retardation and multiple congenital malformations. It is also uncommonly associated with congenital glaucoma. We describe the orbital findings on CT in this rare case of a patient with Opitz syndrome who presented with congenital glaucoma, with a review of the literature. The CT findings of congenital glaucoma, which have not been described before in the literature, are also discussed. It is important for the radiologist to be aware of this rare association. It is also important to be aware of the findings of congenital glaucoma on CT because patients with Opitz syndrome and other syndromes associated with learning difficulties may not present with typical clinical features of glaucoma. A high index of suspicion will lead to a correct diagnosis and earlier intervention.
Opitz syndrome is a rare autosomal recessive disorder caused by a defect of cholesterol metabolism. It is associated with mental retardation and multiple congenital malformations. Multiple midline neurologic abnormalities have been described in the literature. There have been rare reports of congenital glaucoma in association with Opitz syndrome. To the best of our knowledge, radiologic findings on CT of congenital glaucoma have not been described before in the literature. We describe the association as well as radiologic findings on CT of congenital glaucoma.
Case Report
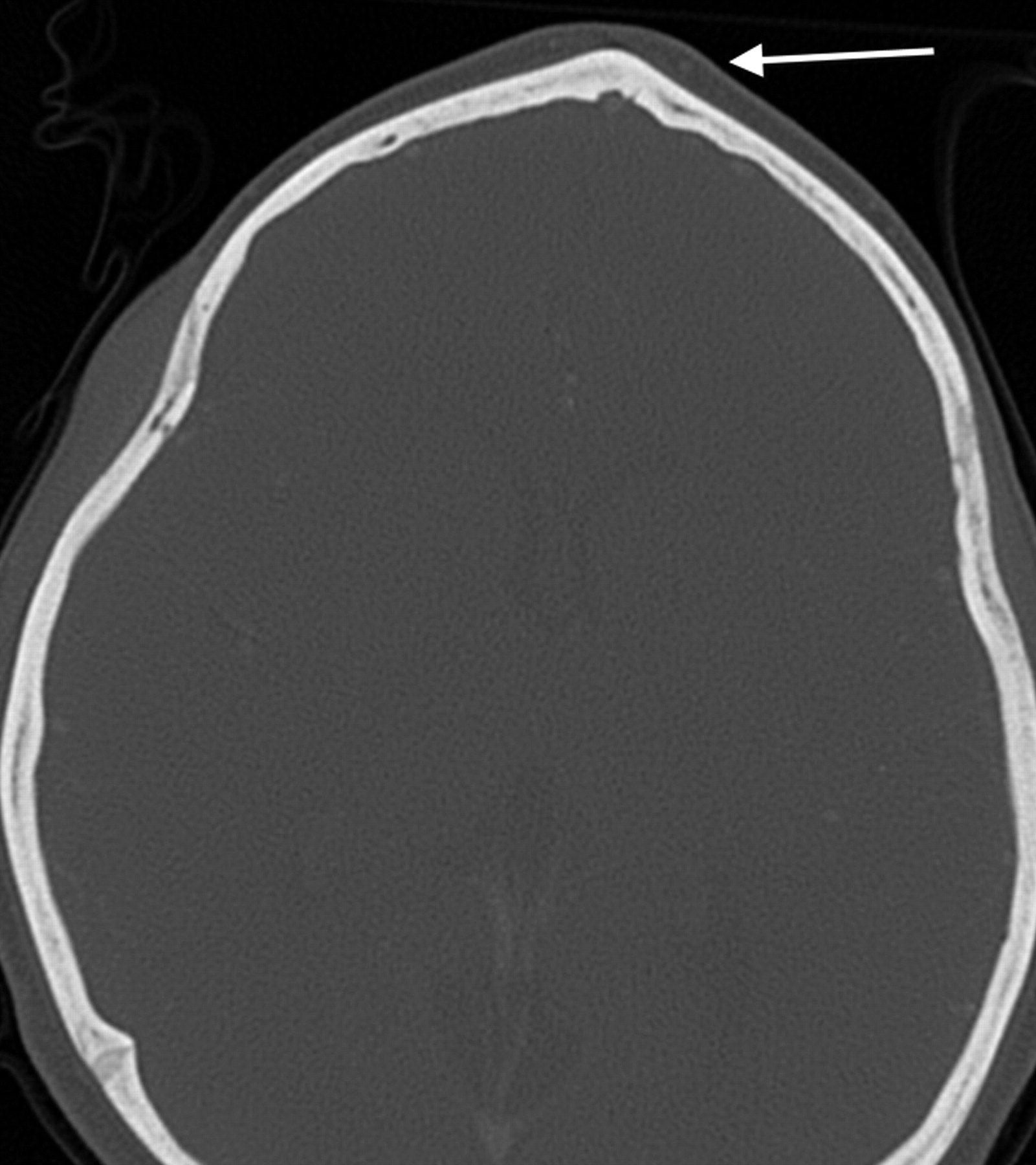
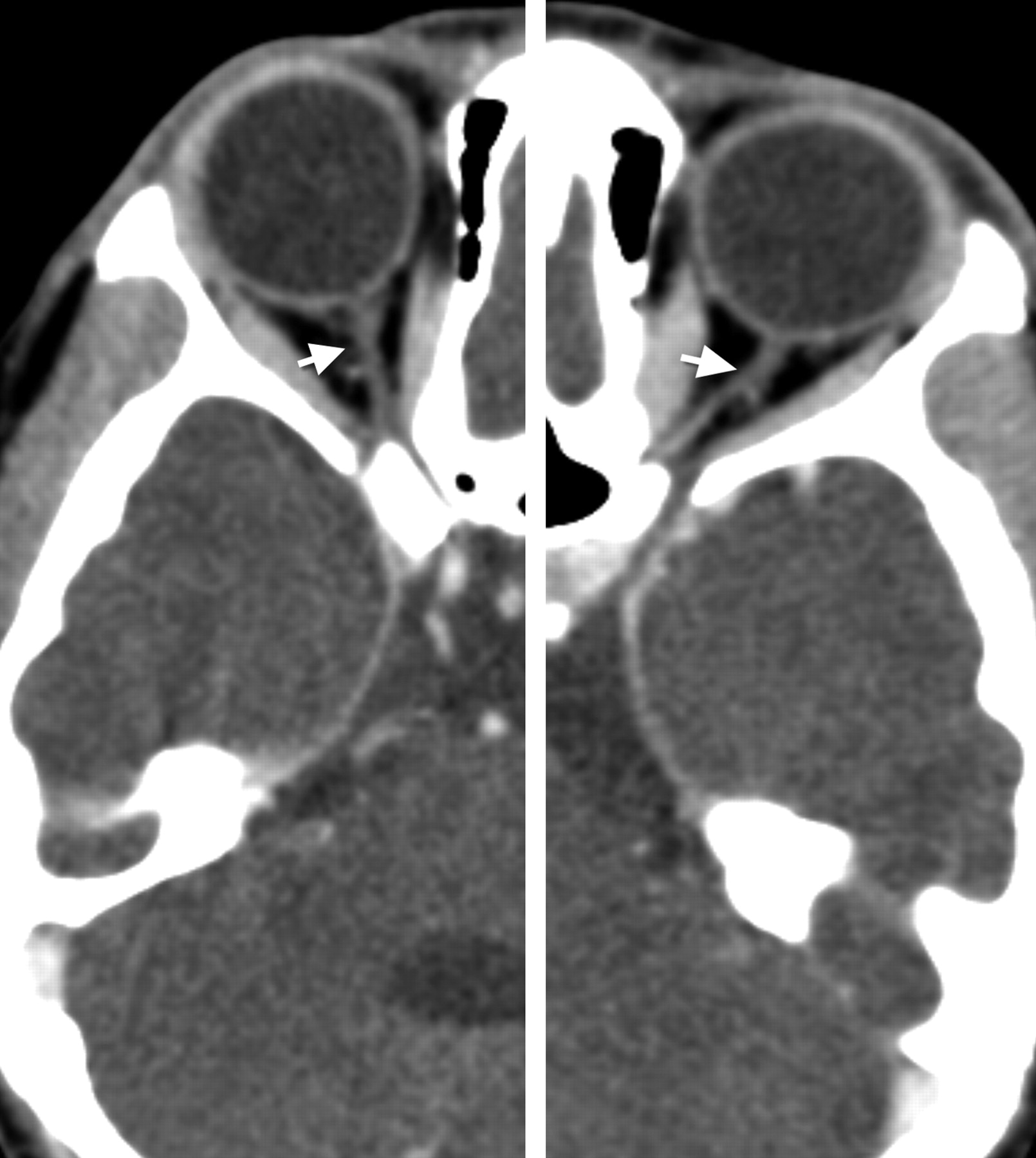
A 12-year-old female patient with Opitz syndrome came to the emergency department with a history of increasing prominence of right eye. She had profound mental retardation; cleft palate; nasal, forehead, finger, and foot deformities; and micrognathia. On previous barium swallow study, her epiglottis was described as short and stubby. A CT study was obtained to exclude a retro-orbital mass and showed a markedly enlarged anterior chamber of the right eye, which measured 6.7 mm in the anteroposterior dimension compared with 4.0 mm on the left side, which is also enlarged (Figs 1 and 2). Trigonocephaly was noted (Fig 3). Bilateral optic nerve atrophy (Fig 4) was also noted. On ophthalmologic examination, she was found to have large cornea with a pressure of more than 40 bilaterally, worse on the right side. She subsequently was given a topical beta-blocker, systemic carbonic anhydrase inhibitor, and brimonidine. One week later, she had trabeculotomy and trabeculectomy of her right eye and, a few weeks later, trabeculotomy and trabeculectomy of her left eye.

Axial CT image through the orbits after administration of intravenous (IV) contrast medium, which demonstrates a markedly enlarged anterior chamber of the right globe (arrow) and mildly enlarged anterior chamber of the left globe (arrowhead).

Sagittal reconstructed CT images through the orbit after IV contrast medium, which demonstrates a markedly enlarged anterior chamber of the right globe (arrow) and a mildly enlarged anterior chamber of the left globe (arrowhead).

Axial CT image through the frontal bone in bony windows demonstrating trigonocephaly (arrow).

Axial CT images through the optic nerve after IV contrast medium showing bilateral optic nerve atrophy (arrows).
Discussion
Opitz syndrome is a rare autosomal disorder caused by a defect in cholesterol metabolism. It is a heterogeneous disorder ranging from lethality to minor abnormalities. The abnormalities involve multiple systems including mental retardation; structural brain abnormalities; craniofacial abnormalities; and abnormalities of the heart, bowel, liver, lung, extremities, and genitalia. The ophthalmologic findings described have included blepharoptosis, congenital cataracts, optic atrophy, nystagmus, blepharoptosis, epicanthal folds, convergent strabismus, downslanting small palpebral fissures, mild exophthalmos, retinal pigment epithelial defects, pale disks, nystagmus, microcornea, aniridia, congenital cataracts, postlenticular membrane, Duane retraction syndrome, absence of lacrimal punctaopsoclonus-like eye movements, lack of visual-following responses and opticokinetic reflexes, corneal enlargement, abnormal iris insertion, bilateral optic pits, sclerocornea, and optic nerve demyelination.1 Congenital glaucoma is uncommonly seen with Opitz syndrome.2,3 Glaucoma can also be associated with other congenital disorders including Sturge-Weber syndrome, neurofibromatosis, Lowe syndrome, Pierre Robin syndrome/sequence, Marfan syndrome, homocystinuria, aniridia, Axenfeld anomaly, and Reiger syndrome.4 Secondary causes of infantile glaucoma causing similar appearance include maternal rubella, syphilis, retinopathy of prematurity, infantile xanthogranuloma, trauma, and retinoblastoma.5
The dimensions of the globe are relatively constant, varying within a millimeter or so with the average sagittal diameter measuring approximately 24.15 mm (outer) and 22.12 mm (inner). In boys, the diameter is approximately 0.5 mm more than that in girls. At birth, the sagittal diameter of the eyes varies from 16 to 17 mm and then increases to an average value of 22.5 to 23 mm at the age of 3 years. It further increases by approximately 1 mm between the ages of 3 and 13 years and then stays stable. The overall incidence of congenital glaucoma is 1:5000 to 1:10,000 live births. It is more common in boys (60%–70%) and is bilateral in 64% of 88% of patients.4 In congenital glaucoma, developmental abnormalities cause obstruction to the flow of the aqueous humor from the anterior chamber, resulting in increased intraocular pressure. The different theories to explain obstruction include the Barkan membrane covering the trabecular meshwork, congenital absence of the Schlemm canal, and an embryonic anterior chamber angle.4 In young children, this results in enlargement, stretching, and thinning of the coats of the eye, as the eyes are of sufficient plasticity. This is especially marked in the anterior chamber, resulting in a deep anterior chamber. The appearance is said to resemble the eyes of an ox (buphthalmos). In the adult, a similar degree of raised pressure will only cause stretching in the region of the lamina cribrosa.5 The normal mean anterior chamber depth is approximately 3 mm, which varies with the measuring method and the age and sex of the patient.6,7 In congenital glaucoma, the mean anterior chamber depth is 6.3 mm.5 In our patient, the sagittal diameter of the globe on the right side measured 27 mm, with the anterior chamber measuring 6.7 mm. Therefore, it has been predominantly an enlargement of the anterior chamber. These eyes may develop subluxated lens. Complications include atrophy of the optic nerve, which was noted on our study. The optic nerve should measure approximately 3 to 4 mm in the orbit.6 On our patient, it measured approximately 2 mm. It is also important to note that the primary closed-angle glaucoma is associated with a narrow anterior chamber.8 The condition tends to stabilize in early youth, possibly because of a stretching process opening up the trabeculae of the angle of the anterior chamber. In the absence of effective treatment, the end result is almost invariably blindness.5
On the axial sections, it is important to measure the depth of the anterior chamber at the equator because a globe rotated superiorly or inferiorly may give an erroneous measurement. The best way to assess the anterior chamber is on sagittal images, which on CT examination can be easily reconstructed from the raw data of most of the modern multidetector CT studies. A significant difference in the size of the 2 globes or an absolute measurement of more than 5 mm may also be considered abnormal.9 An enlarged anterior chamber can also be seen in other causes of glaucoma, including posttrauma. Hampton10 has compiled a comprehensive classification of pseudodevelopmental glaucoma with its differentiating features. It has also been reported in cases of posterior scleral rupture.9 However, the diagnosis may be suspected by the clinical history of trauma as well as other signs of globe trauma including loss of volume, significant change in globe contour, or vitreous hemorrhage.11 Subluxation of the lens may also cause an enlarged anterior chamber, but the lens is usually rotated and the diagnosis is obvious clinically. Other differential diagnoses would include megalocornea, high congenital myopia, congenital staphyloma, and also congenital hereditary dystrophies of the cornea. Megalocornea may appear similar with enlarged anterior chamber but is because of a primary overgrowth rather than secondary to distension and, as such, does not have raised intraocular pressure or optic nerve atrophy.5 The other differential diagnoses listed above are usually clinically obvious.
Conclusion
It is important for the radiologist to be aware of the association of Opitz syndrome with congenital glaucoma. It is also important to be aware of the findings of congenital glaucoma on CT because patients with Opitz and other syndromes associated with learning difficulties may not present with typical clinical complaints of glaucoma. An enlarged anterior chamber sign in the absence of trauma may be a sign of congenital glaucoma, particularly in the presence of optic nerve atrophy, and additional clinical assessment to evaluate for raised intraocular pressure would be required. A high index of suspicion will lead to a correct diagnosis and earlier intervention.
References
- Received November 14, 2007.
- Accepted after revision December 16, 2007.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}