
Abstract
BACKGROUND AND PURPOSE: Fluid-attenuated inversion recovery (FLAIR) MR imaging has advantages to detect meningeal lesions. FLAIR MR imaging was used to detect pachymeningeal thickening and thin bilateral subdural effusion/hematomas in patients with spontaneous intracranial hypotension (SIH).
MATERIALS AND METHODS: Eight patients were treated under clinical diagnoses of SIH. Chronologic MR imaging studies, including the FLAIR sequence, were retrospectively reviewed.
RESULTS: Initial MR imaging showed diffuse pachymeningeal thickening as isointense in 6 cases, hypoisointense in 1 case, and isohyperintense in 1 case on the T1-weighted MR images, and hyperintense in all cases on both T2-weighted and FLAIR MR images. Dural (pachymeningeal) hyperintensity on FLAIR MR imaging had the highest contrast to CSF, and was observed as linear in all patients, usually located in the supratentorial convexity and also parallel to the falx, the dura of the posterior fossa convexity, and the tentorium, and improved after treatment. These characteristics of diffuse pachymeningeal hyperintensity on FLAIR MR imaging were similar to diffuse pachymeningeal enhancement (DPME) on T1-weighted imaging with gadolinium. Initial FLAIR imaging clearly showed subdural effusion/hematomas in 6 of 8 patients. The thickness of subdural effusion/hematomas sometimes increased transiently after successful treatment and resolution of clinical symptoms.
CONCLUSION: Diffuse pachymeningeal hyperintensity on FLAIR MR imaging is a similar sign to DPME for the diagnosis of SIH but does not require injection of contrast medium. FLAIR is useful sequence for the detection of subdural effusion/hematomas in patients with SIH.
Spontaneous intracranial hypotension (SIH) syndrome is characterized by low CSF pressure and positional headache caused by leakage of spinal CSF.1,2 MR imaging has revolutionized the identification, diagnosis, management, and understanding of SIH. The characteristic MR signs of SIH include diffuse pachymeningeal (dura mater) enhancement (DPME), bilateral subdural effusion/hematomas, downward displacement of the brain, enlargement of the pituitary gland, prominence of the spinal epidural venous plexus, engorgement of cerebral venous sinuses (“venous distension sign,” etc),3 venous sinus thrombosis,4 and isolated cortical vein thrombosis.5 DPME after gadolinium administration may be the most common and indicative sign1,2 and forms the basis of the proposed “syndrome of orthostatic headache and diffuse pachymeningeal gadolinium enhancement.”6
The cause of DPME remains unclear. Histologic examination of meningeal biopsy specimens consistently demonstrates a thin layer of fibroblasts as well as small, thin-walled, dilated blood vessels without evidence of inflammation on the subdural surface, the so-called dural border cell layer.7 These findings strongly suggest that dural venous dilation following the Monro-Kellie rule is the most likely explanation of DPME associated with SIH, which states that decreased CSF volume caused by CSF leakage requires volume compensation resulting in meningeal venous hyperemia and subsequent pachymeningeal enhancement.8 However, previous studies did not include detailed neuroradiologic evaluations of the pachymeninges in patients with SIH without artificial contrast materials to evaluate the transient and functional changes of the dura mater.9
Bilateral subdural effusion/hematomas are also classic intracranial signs in the diagnosis of SIH, which again may be explained by the Monro-Kellie rule.1,6,8 The incidence of subdural effusion/hematomas associated with SIH is 10% to 50% with use of conventional neuroradiologic techniques.10,11 Subdural effusion/hematomas associated with SIH tend to be thin (typically 2–7 mm), do not cause appreciable mass effect, occur typically over the convexities of the brain, and appear as variable MR signal intensities depending on the fluid protein concentration or presence of blood.1
The fluid-attenuated inversion recovery (FLAIR) pulse sequence cancels the signal intensity from CSF and causes heavy T2 weighting because of the very long TE, resulting in excellent definition of anatomic detail, such as brain surface sulci, and high lesion contrast in areas close to the CSF.12 This method is commonly used to detect meningeal lesions such as subarachnoid hemorrhage and meningitis.13–15 Therefore, FLAIR MR imaging may be the optimum sequence to evaluate the thickened dura associated with SIH and to detect the very thin subdural effusion/hematomas located close to the subarachnoid CSF space.
Our study used FLAIR MR imaging to examine the thickened dura and subdural effusion/hematomas in patients with SIH.
Methods
We retrospectively reviewed the MR images and clinical records of 9 patients treated for clinical diagnoses of SIH at our institution from 2000 to 2006. We obtained informed consent from all patients. One patient was excluded because a FLAIR MR imaging study was not available. Eight consecutive patients (6 women and 2 men; age range, 36–59 years) underwent MR imaging including the FLAIR sequence. All patients manifested positional headache, which worsened shortly after assuming the upright position and improved or disappeared after lying down. The associated symptoms and signs were nausea (n = 3), vomiting (n = 3), tinnitus (n = 3), and sixth cranial nerve palsy (n = 1). Criteria to establish the diagnosis of SIH were similar to those reported previously for SIH and included the following: diffuse headache that worsens within 15 minutes after sitting or standing, evidence of low CSF pressure on MR imaging, and spontaneous resolution of headache or within several days after epidural blood patch.1,3,16 The 6 patients with SIH were treated supportively (strict bed rest) for 2 weeks after admission, and 2 patients improved. The other 4 patients received epidural blood patch on the basis of the findings of 3D CT myelography, radionuclide cisternography, and spinal MR imaging. The most recent 2 patients with SIH received epidural blood patch without strict bed rest. Burr-hole surgery and drainage for subdural hematoma were performed in these 2 patients after epidural blood patch. All patients had an excellent outcome. The cases of these patients were partially reported previously.17
MR imaging was performed with 1.5T and 0.3T systems. Axial, coronal, or sagittal T1-weighted images with and without gadolinium were obtained in all studies (TR, 440–500 ms; TE, 12.9–20 ms). Axial T2-weighted images were routinely obtained in all studies (TR, 3600–4500 ms; TE, 95–120 ms). All patients underwent axial or coronal (or both) FLAIR imaging (TR, 7000–9000 ms; TE, 97–158 ms, inversion time, 1400–2500 ms). A total of 408 sections of FLAIR imaging were used for the study (ratio of axial to coronal sections, 1.2:1). The mean section thickness was 5.5 mm (range, 4–8 mm).
Our study evaluated each patient 3 times—as initial, second, and follow-up studies—to clarify the time course of MR imaging findings. Initial and follow-up studies were performed at the first and last visits to the hospital, respectively. The initial studies were performed from 4 days to 2 months after the onset of headache. All patients had intracranial hypotension and severe positional headache at the initial study. Second studies were performed early after successful treatment (epidural blood patch or strict bed rest). MR imaging was not performed early after successful treatment only in case 2. Therefore, a total of 23 MR imaging studies were available. Second studies were performed 10 days to 2 months (mean, 25.9 days) after the initial studies. Follow-up studies were performed 3 to 5 months after the initial studies (mean, 3.5 months), when all patients had returned to normal daily life without any signs of headache.
Three independent observers reviewed the MR images to assess the signal intensities of the thickened dura and the subdural effusion/hematomas. “Cortical vein sign” was used as the basis to identify subdural effusion/hematomas.18 Signal intensities on T1-weighted MR images were classified as hypointense if equal to or lower than the signal intensity of gray matter, isointense if higher than that of gray matter and lower than that of white matter, and hyperintense if equal to or higher than that of white matter. Signal intensities on T2-weighted and FLAIR MR images were classified as hyperintense if higher than that of brain parenchyma and isointense if almost equal to that of brain parenchyma. The final classifications were determined by consensus of the 3 observers. The presence of DPME on T1-weighted images after injection of contrast agent was evaluated by comparison with the same T1-weighted MR image sections before injection of the agent.
Signal intensities of the thickened dura and bilateral subdural effusion/hematomas were compared on the initial T1-weighted, T2-weighted, and FLAIR MR images of all 8 patients. The distribution of dural abnormality was reviewed as the supratentorial convexity, falx, tentorium, and posterior fossa convexity, and the distribution of subdural effusion/hematoma as the frontal convexity, frontoparietal convexity, and over the supratentorial convexity. The following factors were evaluated on the serial MR images: presence of DPME on T1-weighted images with gadolinium (yes or no), presence of diffuse pachymeningeal hyperintensity on FLAIR imaging (as explained in the results section; yes or no), and thickness of subdural effusion/hematoma (very thin, ≤3 mm; thin, >3–≤6 mm; thick, >6–≤10 mm; very thick, >10 mm). The chronologic changes of these characteristics of the dura and subdural effusion/hematomas were evaluated.
Results
The initial MR images of all patients showed diffuse pachymeningeal thickening, appearing as isointense in 6 patients, hypoisointense in 1 patient, and isohyperintense in 1 patient on the T1-weighted MR images, and hyperintense in all cases on both T2-weighted and FLAIR MR images. The CSF appeared as hypointense, hyperintense, and hypointense in all patients on T1-weighted, T2-weighted, and FLAIR images, respectively. Therefore, the pachymeningeal hyperintensity had the highest contrast to the CSF on the FLAIR images and no contrast on the T2-weighted images (Fig 1). This linear pachymeningeal hyperintensity was diffuse but had uniform thickness and was not uneven, so it was defined as diffuse pachymeningeal hyperintensity on FLAIR imaging. Bilateral subdural effusion/hematomas were observed at the initial study in 6 of the 8 patients, as hypointense in 1 patient, hypoisointense in 3 patients, isointense in 1 patient, and isohyperintense in 1 patient on the T1-weighted MR images, and hyperintense in all patients on both T2-weighted and FLAIR MR images. Subdural effusion/hematoma had the highest contrast to the CSF on FLAIR images and no contrast on T2-weighted images. The dura mater and the extremely thin subdural effusion/hematomas were difficult to distinguish on FLAIR MR images because these structures appeared with similar hyperintensity. The dura mater was considered to appear as linear hyperintensity in the internal skull region and subdural effusion/hematoma as bulge-shaped hyperintensity in the subdural region. The T1-weighted and T1-weighted images with gadolinium were also examined to identify subdural effusion and hematoma.

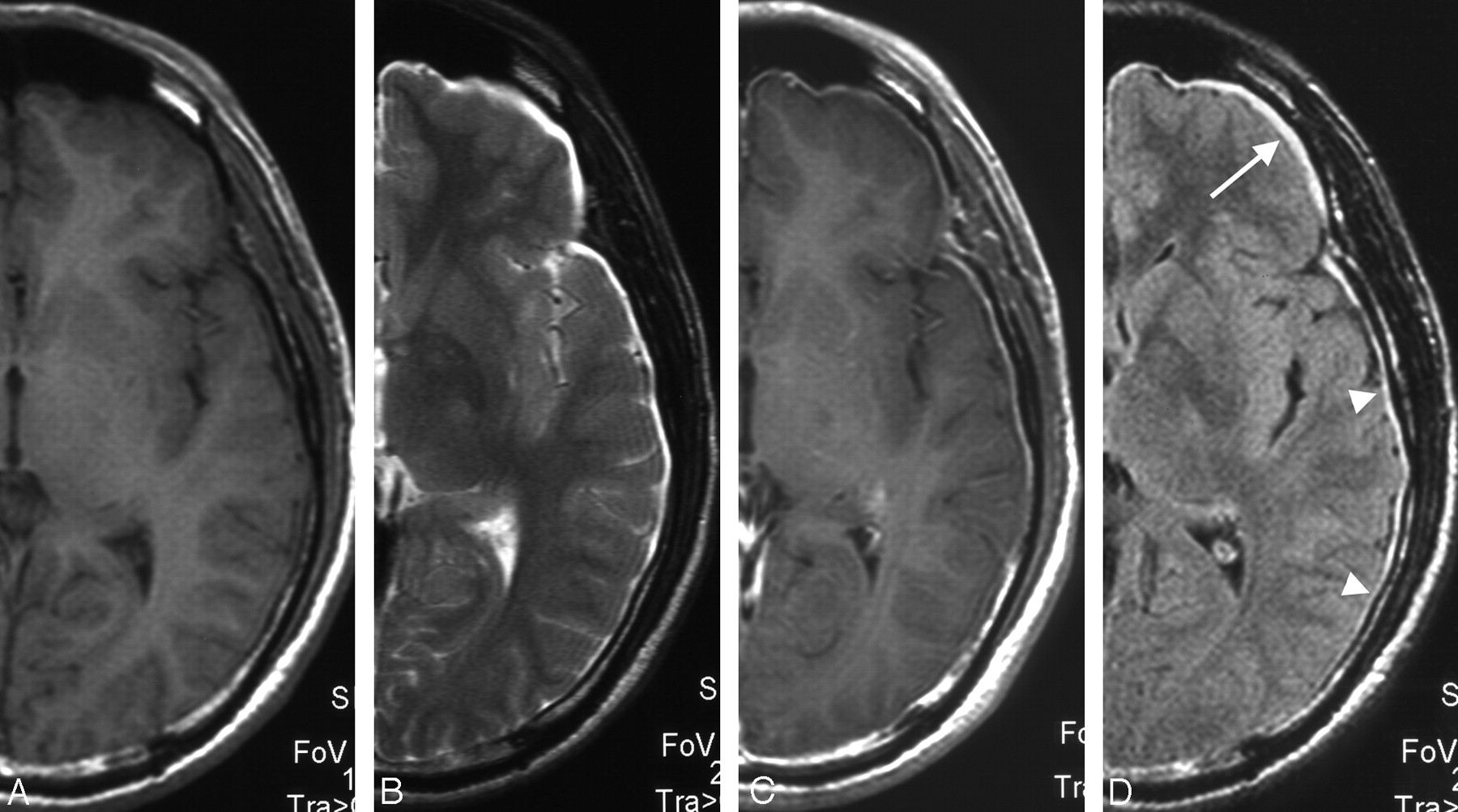
Patient 5. Initial axial, half cut, and magnified MR images of a 39-year-old man with spontaneous intracranial hypotension who presented with a 1-month history of orthostatic headache, nausea, vomiting, and diplopia. Supportive treatment resolved the symptoms. A, T1-weighted image showing diffusely thickened dura mater as isointense. Subdural lesions are unclear. B, T2-weighted image showing that bilateral subdural effusion/hematomas could not be discriminated from CSF. C, T1-weighted image with gadolinium clearly showing diffuse pachymeningeal enhancement. D, FLAIR image showing diffuse pachymeningeal hyperintensity (arrowheads) and very thin bilateral subdural effusion/hematomas in the frontal region (arrow).
The distributions of DPME, diffuse pachymeningeal hyperintensity on FLAIR imaging, and subdural effusion/hematomas were evaluated with use of the initial and second MR imaging studies because thickening of the diffuse pachymeningeal hyperintensity on FLAIR imaging and new subdural effusion/hematomas appeared between the initial and second studies in a few patients. Diffuse pachymeningeal hyperintensity on FLAIR imaging was located at the supratentorial convexity dura in all patients. Diffuse pachymeningeal hyperintensity on FLAIR imaging was also observed parallel to the falx in 7 patients, to the tentorium in 5 patients, and to the dura of the posterior fossa convexity in 5 patients (Table 1, Fig 2). DPME was observed at the supratentorial convexity, falx, dura of the posterior fossa convexity, and tentorium in all patients. Bilateral subdural effusion/hematomas were observed over the supratentorial convexity in 4 patients, frontal convexity in 2 patients, and frontoparietal convexity in 1 patient (Table 1; Figs 1–3).

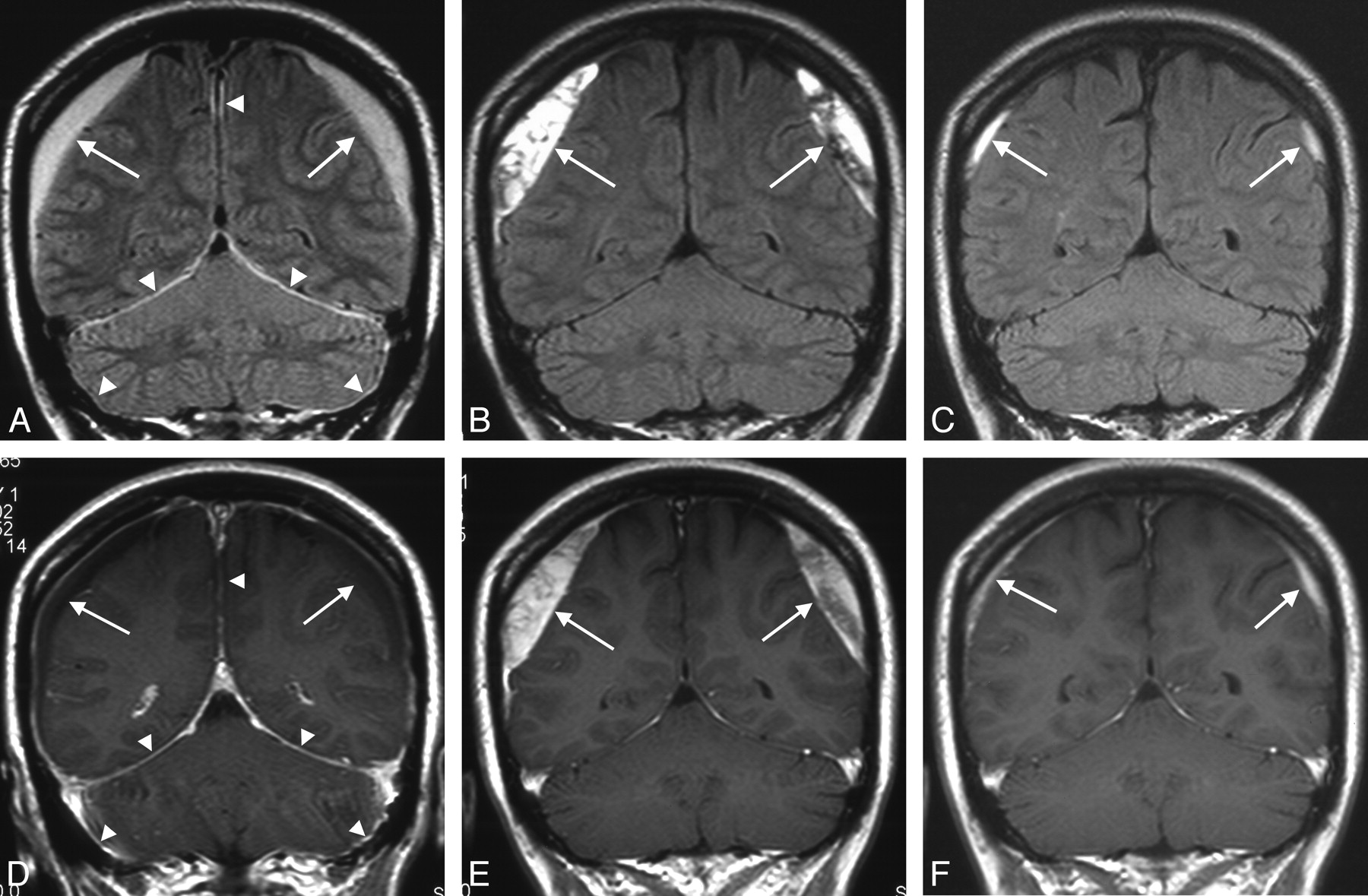
Patient 4. Chronologic FLAIR and T1-weighted MR images of a 37-year-old woman with spontaneous intracranial hypotension. She had a 1-month history of orthostatic headache. Cervical epidural blood patch resolved the symptoms. A, Initial FLAIR image showing diffuse pachymeningeal hyperintensity at the falx, tentorium, and dura of the posterior fossa (arrowheads) and bilateral thick subdural effusion/hematomas (arrows). B, Second FLAIR image performed 1 month after effective blood patch showing disappearance of the diffuse pachymeningeal hyperintensity but thickening of the subdural effusion/hematomas (arrows). C, Follow-up FLAIR image showing remnant subdural effusion/hematomas (arrows). D, Initial T1-weighted image with gadolinium showing DPME at the falx, tentorium, and dura of the posterior fossa (arrowheads) and bilateral thick subdural effusion/hematomas (arrows). E, Second T1-weighted image taken 1 month after completely effective blood patch showing slight remnant of DPME and thickening of the subdural effusion/hematomas (arrows). F, Follow-up T1-weighted image showing remnant subdural effusion/hematomas (arrows).

Patient 8. Chronologic FLAIR and T1-weighted MR images of a 47-year-old woman with spontaneous intracranial hypotension. She had a 1-week history of orthostatic headache. Lumbar epidural blood patch resolved the symptoms. A, Initial FLAIR image showing diffuse pachymeningeal hyperintensity (arrowheads). B, Second FLAIR image taken 1 week after completely effective blood patch showing thickened diffuse pachymeningeal hyperintensity (arrowheads) and partial subdural effusion/hematomas (arrows). C, Follow-up FLAIR image showing disappearance of the diffuse pachymeningeal hyperintensity and subdural effusion/hematomas. D, Initial T1-weighted image with gadolinium showing DPME (arrowheads). E, Second T1-weighted image taken 1 week after effective blood patch showing disappearance of DPME (arrowheads) and partial subdural effusion/hematomas (arrows). F, Follow-up T1-weighted image showing disappearance of the DPME and subdural effusion/hematomas.
Distribution of diffuse pachymeningeal hyperintensity on FLAIR imaging and/or bilateral subdural effusion/hematomas in patients with spontaneous intracranial hypotension
The initial MR imaging studies of all patients showed DPME and diffuse pachymeningeal hyperintensity on FLAIR imaging, but these signs had improved or disappeared at the second or follow-up study (Table 2). In particular, diffuse pachymeningeal hyperintensity on FLAIR imaging had disappeared on the follow-up MR images in all patients. Subdural effusion/hematomas were detected in 6 of 8 patients at the initial study, 6 of 7 at the second study, and 2 of 8 at the follow-up study. Subdural effusion/hematomas were observed in 7 of 8 patients in all studies. Subdural effusion/hematoma thickness had increased, or de novo subdural effusion/hematomas had developed at the second study despite successful treatment in patients 1, 3, 4, and 8 (Figs 2, 3). The other patients showed no change during this period. Subdural effusion/hematomas had improved or disappeared at the second or follow-up study in all patients.
Summary of changes in MR imaging appearance in patients with spontaneous intracranial hypotension
Discussion
Our study attempted to evaluate pachymeningeal thickening and detect thin bilateral subdural effusion/hematomas in patients with SIH by using FLAIR MR imaging without contrast agent. The main observations were as follows:
Diffuse thickening of the dura mater appeared as linear hyperintensity on FLAIR imaging, with high contrast to the CSF, in all patients with SIH. This finding was defined as diffuse pachymeningeal hyperintensity on FLAIR imaging.
Diffuse pachymeningeal hyperintensity on FLAIR imaging was usually located in the supratentorial convexity and also occurred parallel to the falx, the dura of the posterior fossa convexity, and the tentorium and had disappeared by the final MR imaging study after successful treatment. These features are similar to those of DPME detected by T1-weighted MR imaging with gadolinium.
Subdural effusion/hematomas were frequently observed, though sometimes were very thin, on FLAIR images.
Subdural effusion/hematomas sometimes showed transient increase in thickness, but both DPME and diffuse pachymeningeal hyperintensity on FLAIR imaging improved or disappeared early after successful treatment in these patients.
Diffuse pachymeningeal hyperintensity on FLAIR imaging was detected at the initial study in all our patients (Tables 1 and 2). Diffuse pachymeningeal hyperintensity on FLAIR imaging was usually located in the supratentorial convexity but also occurred parallel to the falx, the dura of the posterior fossa convexity, and the tentorium (Table 1; Fig 2). The appearance and disappearance of diffuse pachymeningeal hyperintensity on FLAIR imaging almost paralleled those of DPME (Table 2; Figs 2 and 3). In the initial stage, both diffuse pachymeningeal thickening and subdural effusion/hematomas appeared as hyperintense on FLAIR images and could not be discriminated, but diffuse pachymeningeal hyperintensity on FLAIR imaging disappeared more rapidly than subdural effusion/hematomas after treatment. This characteristic is also similar to DPME. Review of FLAIR MR images of previously reported patients with SIH found that diffuse pachymeningeal hyperintensity on FLAIR imaging was present but not actually described as such.11,19
DPME, diffuse pachymeningeal hyperintensity on FLAIR imaging, and subdural effusion/hematomas may have close pathologic relationships in the pachymeninges of patients with SIH. The pachymeninges consist of the outer or periosteal dura mater and the inner or meningeal dura. Deep in the dura mater, overlying the arachnoid, the fibroblasts become more elongated and form a layer of “dural border cells,” which consists of loose fibroblasts and extracellular spaces of various sizes but lacks extracellular collagen and contains small blood vessels. This layer of dural border cells is a structurally relatively weak zone at the dura-arachnoid interface. In general, subdural collections of fluid tend to form in this layer.18,20 The decrease in CSF volume associated with SIH results in compensatory vasodilation in the dural border cell layer,7 resulting in thickening of the pachymeninges. Compensatory minimum high-protein fluid collection may then occur in this layer and develop into subdural effusion and subdural hematoma. Therefore, diffuse pachymeningeal thickening and hyperintensity on FLAIR imaging may be signs of the first pachymeningeal event in the sequence leading to subdural effusion and, subsequently, subdural hematomas. Subdural effusion/hematomas originated in and converged to form linear pachymeningeal thickening appearing as diffuse pachymeningeal hyperintensity on FLAIR imaging in the cases of our patients 3 and 8, respectively (Fig 3).
Our observation of the chronologic changes of subdural effusion/hematomas on FLAIR MR imaging found that the thickness of subdural effusion/hematomas at the supratentorial convexity increased in 4 patients between the initial and second studies despite successful treatment. However, such paradoxic increase of subdural effusion/hematoma thickness may not indicate treatment failure because the increase was transient and had improved in all patients at follow-up study. Such transient increase of intracranial subdural effusion/hematomas after treatment has previously been reported in a case very similar to our patient 4 (Fig 2).21 The thickness of the subdural effusion/hematomas had increased for 1 to 2 months after epidural blood patch, but DPME (or diffuse pachymeningeal hyperintensity on FLAIR imaging) had improved. Follow-up MR imaging showed the subdural effusion/hematomas had improved without intervention. The reason for this transient thickening of subdural effusion/hematomas after treatment remains unclear. The balance phenomenon acting during the weak self-expanding potential of subdural effusion/hematomas and volume restoration of CSF is a potential candidate. An additional large MR imaging series is required to clarify the relationship among DPME, diffuse pachymeningeal hyperintensity on FLAIR imaging, and subdural effusion/hematomas in patients with SIH.
Bilateral subdural effusions/hematomas are one of the main neuroimaging signs of SIH, but conventional neuroradiologic modalities such as CT and T1-weighted or T2-weighted MR imaging generally achieve low rates of detection. Subdural effusion/hematomas associated with SIH are frequently thin, so the rate of detection may depend on the sensitivity of the technique. MR imaging is generally superior to CT for the imaging of subdural fluid collection, both for estimating the size and detecting small collections.22 However, subdural effusion may be occasionally difficult to detect because both the lesion and CSF have similar signal intensities on both conventional T1-weighted and T2-weighted images.18 Subdural fluid collection associated with SIH may occur as effusion in the early stage and may be very thin. Therefore, subdural effusion/hematomas associated with SIH, especially in the early stage, may be difficult to detect by conventional T1-weighted and T2-weighted sequences.
FLAIR MR imaging can detect an increase in protein concentration in the CSF with high sensitivity depending on the effective TE, show anatomic detail such as brain surface sulci, and provides high lesion contrast in areas close to the CSF.12 The detectable protein concentration threshold may be 125 mg/dL in the conditions used in this study.23 Furthermore, FLAIR MR imaging is generally superior for the detection of brain surface lesions. The high tissue contrast between gray and white matter on T2-weighted MR imaging may also obscure small hyperintense lesions at or on the surface of the brain. By suppressing the signal intensity from the CSF and the tissue contrast between gray and white matter, the FLAIR sequence considerably improves the visualization of small lesions at the periphery of the cerebral hemispheres, such as subdural hematomas.24 In our study, FLAIR MR imaging provided higher contrast between subdural effusion/hematomas and CSF than T1-weighted or T2-weighted MR imaging. FLAIR MR imaging detected bilateral subdural effusion/hematomas in 6 of the 8 patients with SIH, a considerably higher rate than that found by conventional MR imaging sequences.
Our study suggests that diffuse pachymeningeal hyperintensity on FLAIR imaging may provide similar clinical indications to the finding of DPME in patients with SIH. However, diffuse pachymeningeal hyperintensity on FLAIR imaging was not exactly equivalent to DPME during the time course of the study. The second MR imaging studies, which were performed early after successful treatment, suggested that diffuse pachymeningeal hyperintensity on FLAIR imaging disappeared more rapidly than that of DPME (Table 2). This difference might be related to the relative sensitivities of the 2 techniques or possibly to the relative rates of response to the normalization of intracranial pressure after treatment. Unfortunately, this study included only a few patients, so we could not investigate the sensitivity of diffuse hyperintensity on FLAIR imaging. Our overall impression is that diffuse pachymeningeal hyperintensity on FLAIR imaging is slightly less sensitive than that of DPME. However, FLAIR MR imaging does not require the injection of gadolinium contrast agent, so it is preferable in patients with contraindications such as allergy, asthma, pregnancy, etc.
The weaknesses of our study were the variations in the clinical course and data collection due to the retrospective nature of the study. In particular, the treatment concept and protocol were modified during the study period. We emphasized strict bed rest before epidural blood patch for the initial treatment of SIH at the beginning of the study. However, epidural blood patch was given priority later.25 This study involved retro-spective collection of MR images. However, the second MR study in patient 2 did not match the definition of “early after successful treatment.” Also, permission for injection of contrast material was refused at the second MR study by patient 3. In fact, the findings of the second MR studies were varied. However, our findings do indicate a relationship between diffuse pachymeningeal hyperintensity on FLAIR imaging and subdural effusion/hematomas, and the relative sensitivity of diffuse pachymeningeal hyperintensity on FLAIR imaging compared with DPME based on the MR studies including the second MR studies. A larger prospective study is required to establish the pathologic meaning and true sensitivity of diffuse pachymeningeal hyperintensity on FLAIR imaging.
FLAIR MR imaging in patients with SIH detected linear thickening of the dura as hyperintensity (diffuse pachymeningeal hyperintensity on FLAIR imaging) in all 8 patients in our series, with similar chronologic characteristics to those of DPME detected by T1-weighted MR imaging with gadolinium. FLAIR MR imaging also detected bilateral subdural effusion/hematomas in 6 of the 8 patients with SIH. FLAIR MR imaging has the potential to provide a simple, noninvasive method for the diagnosis of SIH.
Footnotes
This study was partly supported by grants from the Ministry of Education, Science, Sports, and Culture.
References
- Received October 12, 2007.
- Accepted after revision January 17, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- MRI Findings after Recent Image-Guided Lumbar Puncture: The Rate of Dural Enhancement and Subdural Collections
- Delayed diagnosis of bilateral subdural effusions complicating intracranial hypotension in a patient presenting with post lumbar puncture headache
- Postoperative Intraspinal Subdural Collections after Pediatric Posterior Fossa Tumor Resection: Incidence, Imaging, and Clinical Features
- Dural Hyperintensity on Fluid-Attenuated Inversion Recovery in Spontaneous Intracranial Hypotension
- Reply: