
Abstract
BACKGROUND AND PURPOSE: Endoscopic endonasal surgery let us observe that woodworkers’ nasal adenocarcinomas originate in the olfactory cleft. Our aim was the identification of CT imaging features that corroborate the olfactory cleft as the site of origin for woodworkers’ adenocarcinoma.
MATERIALS AND METHODS: We designed a retrospective study to compare CT scans of 27 unilateral olfactory cleft adenocarcinomas with 30 cases of nasosinusal polyposis (NSP) and 33 healthy sinus controls. Enlargement of the olfactory cleft, lateralization of the ethmoidal turbinate wall, and contralateral bulging of the nasal septum were measured on coronal scans passing through crista galli and posterior half of both ocular globes. Comparisons have been performed by using analysis of variance and the Bonferroni procedure.
RESULTS: The nasal septum was significantly bulging across the midline in adenocarcinoma (4.6 ± 3 mm; range, −0.1–13.7 mm) compared with NSP (0.7 ± 1 mm; range, −2.1–2.3 mm) or healthy sinus controls (0.5 ± 1 mm; range, −1.2–2 mm) (P < .001). The olfactory cleft was significantly wider in adenocarcinoma (15.1 ± 4.5 mm; range, 8.6–25.7 mm) than in NSP (3.6 ± 0.4 mm; range, 2.8–4.6 mm) or healthy sinus controls (3.3 ± 0.7 mm; range, 1.4–4.6 mm). The ethmoidal labyrinth width was significantly smaller on the pathologic side in adenocarcinoma (7.2 ± 2.7 mm; range, 3.2–14.2 mm) than in the control groups (P < .001). Whereas the angle between the conchal lamina and vertical midline was close to zero degrees in NSP (0.03 ± 2.25°; range, −5°–3°) and healthy sinus controls (0.45 ± 2.13°, range, −5°–5°), it reached 39.76 ± 13.83° (P < .001) in adenocarcinoma.
CONCLUSIONS: Radiologists should suspect nasal adenocarcinoma on sinus CT scans showing a unilateral expanding opacity of the olfactory cavity.
Neoplastic diseases of the nose and paranasal sinuses require thorough assessment of location and extension to plan appropriate treatment. Adenocarcinoma is known to be associated with exposure to wood dust and usually develops in woodworkers.1 Woodworkers’ adenocarcinoma is classically described as originating in the ethmoid sinuses and is resected by a transfacial or craniofacial approach.2
During the last decade some authors have shown that malignant tumors could also be resected by using endonasal endoscopic surgical techniques.3, 4 Our experience in this field started in 2000, and since 2004, we have suspected that woodworkers’ adenocarcinoma could originate in the olfactory cleft in most cases. A prospective study in 20 consecutive patients undergoing endonasal endoscopic resection between 2004 and 2006 has confirmed the origin of woodworkers’ adenocarcinoma in the olfactory cleft.5
Moreover endoscopic resection revealed that woodworkers’ adenocarcinomas grow out of the olfactory cleft into the nasal cavity like polyp neoplasms with well-defined bodies and that for a long time, even after becoming large, many of them do not invade, but just displace and push out the surrounding structures (ie, the nasal septum and the turbinate wall of the ethmoidal labyrinth).6
The aim of this study using CT was an attempt to detect imaging features (ie, enlargement of the olfactory cleft, lateralization of the ethmoidal turbinate wall, and contralateral bulging of the nasal septum) that suggest the olfactory cleft as the site of origin for woodworkers’ adenocarcinoma.
Materials and Methods
We designed a retrospective study to compare the CT scans of 27 consecutive woodworkers having undergone surgery under endoscopic control on unilateral olfactory cleft adenocarcinomas between January 2004 and June 2007 with the CT scans of 30 patients having undergone surgery for nasosinusal polyposis (NSP) and 33 controls with healthy sinuses.
Patients
Adenocarcinoma Group.
Adenocarcinoma diagnosis was based on preoperative biopsies. Preoperative radiologic evaluation has been based on CT scans and MR images. Patients were selected for endoscopic surgery with multidisciplinary agreement involving surgeons, radiotherapists, medical oncologists, and radiologists. Contraindications to endoscopic surgery were intracranial (2 patients), intraorbital (0 patients), or facial skin invasion (1 patient). For the sake of this study, the exceptional patients having bilateral or contralateral extension of the tumor were excluded (3 patients). The study group was composed only of men between 54 and 79 years of age (mean, 68 years). They all had been woodworkers (ie, had been exposed to wood dust during their occupational life for at least 12 cumulated months; French legal mention for Occupational Diseases7).
Control Groups.
Using the last digit of each number in a table of random numbers, we collected the CT scans of 30 patients (21 men; mean age, 51 years; range, 24–77 years) among 189 patients who had undergone surgery for NSP without respiratory epithelial adenomatoid harmatoma (REAH) on pathologic examination in our department between 2003 and 2005. NSP is a chronic inflammatory disease of the ethmoidal sinus mucosa leading to a protrusion of benign edematous polyps from the meatus into the nasal cavity8; REAH is a benign tumor originating in the olfactory cleft, which may coexist in the setting of inflammatory polyps and may enlarge the olfactory cleft width on CT, which is characterized by a glandularlike structural proliferation lined by ciliated respiratory epithelium.9
We also randomly collected 33 CT scans with normal findings of healthy patients (19 women; mean age, 36 years; range, 18–62 years) from the data base of the radiology department of our institution.
Anatomic Terminology
The olfactory cleft (Fig 1) is a narrow chamber opening anteriorly and inferiorly into the nasal fossa, closed laterally by the turbinate wall of the ethmoidal labyrinth6 and medially by the corresponding nasal septum; closed superiorly, from anterior to posterior, by the nasal and frontal bones, the cribriform plate, and the anterior process of the sphenoid roof; and closed posteriorly by the anterior wall of the sphenoid sinus.

Anatomic terminology.
The turbinate wall of the ethmoidal labyrinth6 is made of the conchal lamina and the attached middle and superior (and inconstantly the supreme) turbinates; it separates the olfactory cleft from the ethmoidal labyrinth.
Because the cribriform plate lies more caudal than the ethmoidal roof, the turbinate wall of the ethmoidal labyrinth is attached to the ethmoidal roof due to the lateral lamella of the intracranial olfactory groove.
CT Assessment
Measurements were performed by using a PACS Workstation (AGFA-Gevaert, Health Care, Mortsel, Belgium) from reformatted coronal images with a bone window (level, 200 HU; width, 200 HU).
One coronal scan passing through the crista galli and the posterior half of both ocular globes was selected. In the control groups, 1 side was selected as the “pathologic side” by using a random table of numbers (even numbers for selecting the right side). We measured the following parameters:
OC, width between the midline and the septal bulging or deviation (Fig 2).
CD, width of the olfactory cleft on the pathologic side (Fig 2).
ECL, angle between the midline xy and the conchal lamina (Fig 3).
DE, width of the ethmoidal labyrinth on the pathological side (Fig 2).
AE, naso ethmoidal cavity total width (Fig 2).

Measurement of widths on a coronal scan passing through the crista galli and the posterior half of both ocular globes. The midline is defined by the xy line joining the bases of the crista galli and the vomer bone on the nasal floor. A perpendicular line zt is drawn tangent to the inferior limits of both ocular globes, cutting xy in O and the nasal septum line in C. The OC segment is equal to zero when the nasal septum is straight on the midline and is measured as positive when the C point is displaced opposite to the pathologic side and as negative in reverse conditions. The AE segment on the zt line measures the nasoethmoidal cavity total width and is decomposed into the following subsegments: AB for the width of the healthy ethmoidal labyrinth, BC for the width of the healthy olfactory cleft, CD for the width of the olfactory cleft on the pathologic side (in patients, the CD segment measures the median opacity without recognizable bony lamella, located between the nasal septum and the squeezed ethmoidal labyrinth on the pathologic side), and DE for the width of the ethmoidal labyrinth on the pathologic side (in patients, the DE segment measures the lateral opacity squeezed onto the orbital wall, in which ethmoidal bony lamellas are still recognizable).

Measurement of the ECL angle between the midline xy and the conchal lamina. The conchal lamina is the upper part of the ethmoidal turbinate wall (Fig 1). A line lm is drawn tangent and parallel to the conchal lamina on the pathologic side to measure the ECL angle. In patients, the line lm also represents the border between the median opacity without recognizable bony lamella and the lateral opacity squeezed onto the orbital wall in which ethmoidal bony lamellas are still recognizable.
Statistical Analysis
Descriptive statistics are presented as means, SDs, and ranges. We used analysis of variance and the Bonferroni procedure for correction of multiple testing to compare radiologic features between adenocarcinoma, polyposis, and healthy groups. The level of type I error used to determine statistical significance in the analysis was 5%. Statistical analysis was performed by using SAS System for Windows, Version 9.01 (SAS Institute, Cary, NC).
Results
Descriptive results are summarized in the Table.
Descriptive results*
The OC distance measured a significant deviation of the nasal septum toward the contralateral side of the tumor in the adenocarcinoma group, compared with the polyposis or healthy groups (P < .001) (Fig 4A). The olfactory cleft (CD width) was significantly wider in patients with adenocarcinoma than in patients with NSP or healthy controls (P < .001) (Fig 4B). The ethmoidal labyrinth width (DE) on the pathologic side was significantly smaller in the adenocarcinoma group than in the 2 control groups (P < .001) (Fig 4C). The nasoethmoidal cavity total width (AE) was not different in the 3 groups. Whereas the ECL angle between the midline xy and the conchal lamina was close to zero degrees in both the NSP and healthy control groups, it was measured at 39.76 ± 13.83° (P < .001) in the adenocarcinoma group (Fig 4D).

CT scan demonstrates significant enlargement of the olfactory cleft in the adenocarcinoma (ADC) group compared with NSP and healthy sinus controls (HSC) (P < .05). A, OC, bulging of the nasal septum across the midline. B, CD, width of the pathologic olfactory cleft. C, DE, width of the ethmoidal labyrinth on the pathologic side. D, ECL, angle between the midline xy and the conchal lamina. NS indicates not statistically significant.
Discussion
To our knowledge, there is no specific CT description of woodworkers’ adenocarcinomas in the literature. The CT appearances of malignant tumors of the sinonasal region are characterized by their nonhomogeneous structure: They may destroy the bony margins and infiltrate neighboring regions; they may enhance following the administration of contrast. CT and MR imaging, either singly or in combination, give a range of information about attenuation, signal intensity, contrast enhancement, and mass effect that helps distinguish benign from malignant disease and tumor from secondary mucosal inflammation. MR imaging is particularly useful in this setting because nearly 95% of all sinonasal tumors are of intermediate signal intensity on the T2-weighted sequence, allowing them to be differentiated from the high signal intensity of polyps, mucosal inflammation, and retained secretions. Thick mucinous secretions may be intermediate in signal intensity on the T2 sequence but demonstrate increased signal intensity on the T1 sequence due to the high protein content. Contrast-enhanced CT may, in many cases, suggest the diagnosis of malignancy but does not approach the specificity of MR imaging, especially in the differentiation of large polypoid masses from tumors.
Both CT and MR imaging give precise anatomic detail regarding tumor location and extension, which are critical in the determination of operability or in planning radiation therapy. However, it is often difficult to determine the actual site of origin of tumors in the sinonasal region. Our CT study of woodworkers’ adenocarcinomas describes new clues for the diagnostic work-up of these lesions.
On the basis of our endoscopic observation that woodworkers’ adenocarcinomas originate in the olfactory cleft (Fig 5),5 we retrospectively reviewed all these patients’ CT scans and found that the origin and location of woodworkers’ adenocarcinomas can also be suggested on CT scans. Adenocarcinomas appear as slow-growing tumors causing gradual expansion of the olfactory cavity by pushing onto the nasal septum and the ethmoidal turbinate wall, squeezing the olfactory cleft onto the lateral wall in the healthy nasal cavity and the ethmoidal labyrinth onto the orbital wall in the tumor nasal fossa. Endoscopic surgical dissections have shown that the nasal septum perichondrium-periosteum is an effective barrier preventing invasion of the contralateral nasal fossa; the ethmoidal turbinate wall offers the same protection against invasion of the ethmoidal labyrinth. These 2 characteristics have lead to the surgical concept of endoscopic exenteration of the olfactory cleft as the treatment of choice for removing woodworkers’ adenocarcinomas.5, 10

Endoscopic surgical view of a woodworkers’ adenocarcinoma originating in left olfactory cleft. IT indicates inferior turbinate; MT, middle turbinate; NS, nasal septum; T, tumor into the olfactory cleft.
This new knowledge about the origin and growing behavior of nasal adenocarcinoma improves the imaging diagnosis. The radiologist should now suspect the diagnosis of nasal adenocarcinoma on the sinus CT scan of woodworkers on the basis of unilateral opacity of the olfactory cleft with signs of gradual expansion of the olfactory cavity (ie, bulging of the nasal septum and lateralization of the ethmoidal turbinate wall). These characteristic features have been observed in each of our 27 cases of adenocarcinoma. This highly suggests that the remodelling of the olfactory cleft can be considered the result of a tumor originating in the olfactory cleft rather than a process originating more inferiorly in the nasal cavity and growing superiorly into the olfactory cleft secondarily. This remodelling of the olfactory cleft was not observed in our 2 control groups.
We have not checked for intra- and interobserver variability in our measurements. This lack can be considered a limitation of our study because this variability could affect the level of measurement of parameters (OC, CD, DE, AE, ECL) in each group. However, the data presented in the Table show large differences between adenocarcinoma and control groups, which are probably not very sensitive to intra- and interobserver variability.
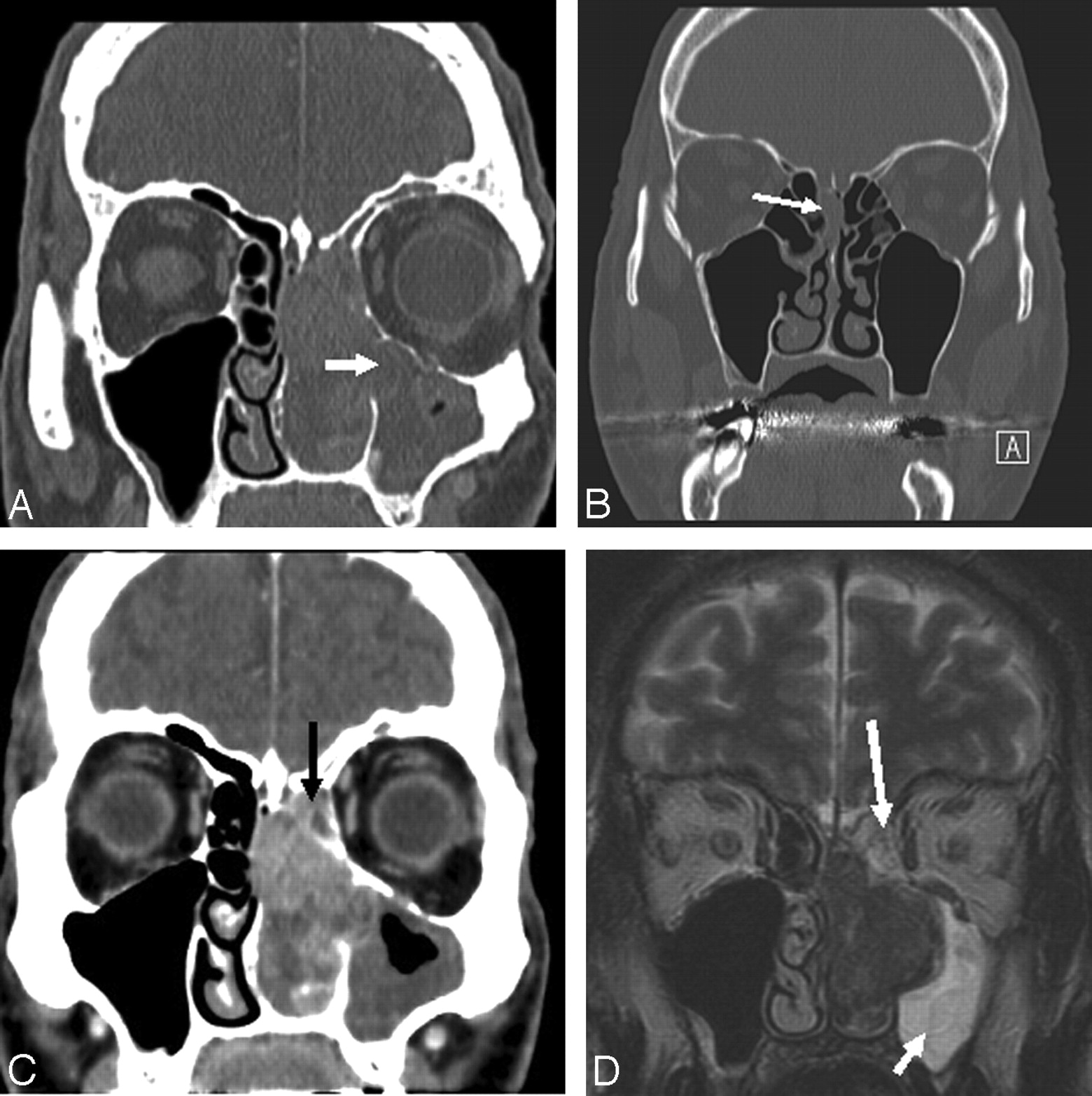
The squeezed ethmoidal labyrinth is usually opaque, but this corresponds to mucus retention in the ethmoidal cells. When one looks closely, the bony conchal lamina, which is the upper portion of the ethmoidal turbinate wall, and the bony partitions of the ethmoidal cells remain visible despite their more-or-less severe squeezing onto the orbital wall; sometimes the inferior part of the ethmoidal labyrinth is reduced to a thin opaque layer with the tumor penetrating into the maxillary sinus through the fontanelle area or bulging onto the medial orbital wall (Fig 6A). Most interesting in large tumors, the upper part of the ethmoidal labyrinth, which lies above the line tangent to the cribriform plate and below the ethmoidal roof (Fig 1), remains, most of the time, uncrushed because the slow-growing tumor originating in the olfactory cleft (below the cribriform plate) sequestrates a small triangle of ethmoidal cells under the ethmoidal roof (which lies more cranially) by lateralizing (not invading) the conchal lamina. All these features are confirmed and better illustrated on MR imaging (Fig 6C, -D), which is also the imaging technique of choice in the evaluation of intracranial and intraorbital extension.

More examples of woodworkers’ adenocarcinomas. A, The inferior part of the ethmoidal labyrinth is reduced to a thin opaque layer with the tumor penetrating into the maxillary sinus through the fontanelle area (arrow). B, CT scan of an anosmic woodworker, which led to the early diagnosis of a small adenocarcinoma of the right olfactory cleft (arrow). The right olfactory cleft is opacified with a slight bulging of the corresponding nasal septum to the left and of the conchal lamina to the right. Note that there is still a small space filled with air under the cribriform plate and between the conchal lamina and the septum in the left olfactory cleft. C, The slow-growing tumor originating in the olfactory cleft (below the cribriform plate) sequestrates a small triangle (arrow) of ethmoidal cells under the ethmoidal roof (which lies more cranially) by lateralizing (not invading) the conchal lamina. D, MR image confirms the origin in the olfactory cleft with retention in the squeezed ethmoidal labyrinth (long arrow) (note the triangle of ethmoidal cells under the ethmoidal roof) and maxillary sinus (short arrow).
The radiologist should, however, consider a few differential diagnoses, especially in patients who are not woodworkers. Esthesioneuroma is also a unilateral tumor originating in the olfactory cleft. This rare tumor initially expands slowly and unilaterally, allowing the bone to remodel around it. Tumoral calcification is often seen. More aggressive behavior can occur with gross intracranial extension through the cribriform plate, which is better identified on MR imaging.11, 12 REAH is a pathologic entity individualized by Wenig and Heffner in 1995,13 presenting as a benign tumor also originating and expanding in the olfactory cleft. With the methods of measurement used in the present study, it has been shown that REAH can be suspected preoperatively on CT enlargement of the olfactory clefts.9 REAH may coexist in the setting of inflammatory nasosinusal polyps and may enlarge bilaterally the olfactory clefts or can also develop primarily, unilaterally, or bilaterally, favoring secretion retention in the ethmoid and other paranasal sinuses. Clinically, it might present as a differential diagnosis of nasosinusal polyposis or neoplastic lesions like an inverted papilloma or adenocarcinoma. REAH must be suspected on CT enlargement of the olfactory clefts,9 but the final diagnosis belongs to the pathologist.
Finally, another advantage of knowing that woodworkers’ adenocarcinomas originate in the olfactory cleft is early diagnosis of small tumors. In 2 cases in our series of 27 adenocarcinomas, the clinical presentation was limited to loss of the sense of smell. The sinus CT revealed, in both woodworkers, a unilateral opacity limited to the olfactory cleft (Fig 6B), which led to careful endoscopy of this very narrow cavity and biopsies that revealed the diagnosis of adenocarcinoma of the olfactory cleft.14 The most common presentation of nasal adenocarcinoma includes nasal airway obstruction, epistaxis, nasal discharge, pain, or swelling of facial soft tissue. Only poor attention has been paid to loss of the sense of smell, probably because either patients or general practitioners do not always care about the loss in sense of smell or perhaps otorhinolaryngologists do not always perform careful endoscopic examination of the olfactory cleft or ask for CT scans in patients having lost the sense of smell. Radiologists should now search for small olfactory cleft opacities more than for ethmoidal labyrinth opacities in woodworkers with anosmia and actually in all patients with anosmia. The role of systematic endoscopic and/or CT examination of the olfactory clefts15 in people exposed to wood dust needs to be evaluated as a means of early detection of occupational adenocarcinoma.
In conclusion, most clinicians and radiologists have paid attention to the ethmoidal labyrinth during the last 2 decades. Pathology in the adjacent olfactory cleft does, however, also exist. Woodworkers’ adenocarcinoma, an occupational malignancy, was believed, until recently, to originate in the ethmoidal labyrinth. Endoscopic endonasal surgery has recently revealed its origin in the olfactory cleft. Our study indicates that CT can preoperatively suggest the diagnosis of adenocarcinoma due to remodelling features of the olfactory cleft in woodworkers.
References
- Received September 4, 2008.
- Accepted after revision February 7, 2009.
- American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}