
Abstract
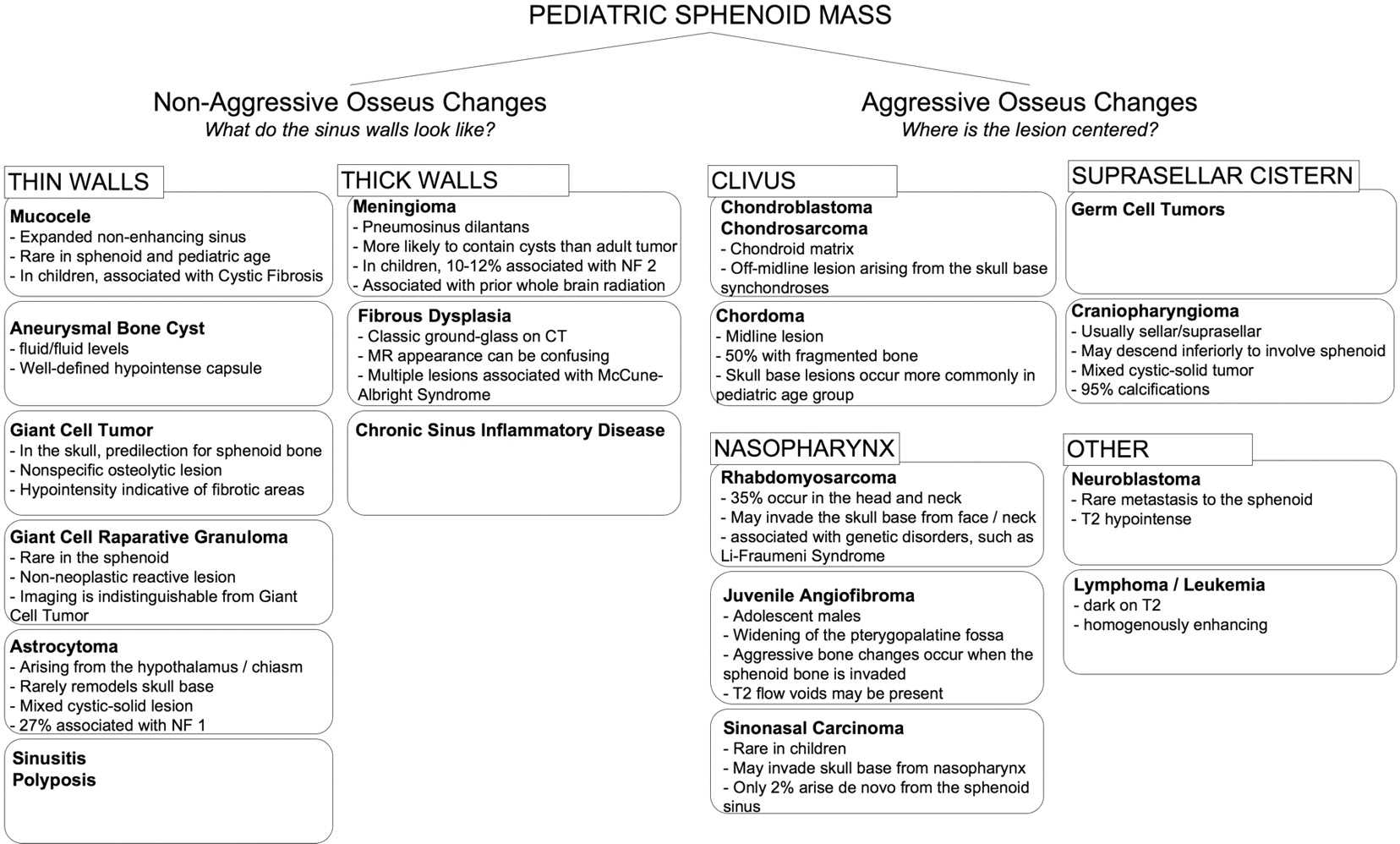
SUMMARY: Childhood central skull base masses are rare, often difficult to diagnose, and have overlapping imaging findings. In this review, we provide an overview of the epidemiology, clinical findings, and management of pediatric sphenoid bone and sphenoid sinus masses with an emphasis on imaging findings that may help to differentiate lesions. Radiologic-pathologic correlation is provided. Finally, an imaging-based algorithm is presented as a guide to help radiologists narrow their differential diagnoses. Some of the entities discussed are virtually unique to the pediatric population; others occur rarely in this age group but should be considered in the appropriate clinical setting. Entities included in the discussion are grouped into 2 categories: those that cause nonaggressive osseous remodeling and those that are more commonly associated with aggressive bone changes. Mucocele, aneurysmal bone cyst, giant cell lesions, meningioma, and fibrous dysplasia tend to remodel bone, while entities such as chordoma, craniopharyngioma, rhabdomyosarcoma, sinonasal carcinoma, and neuroblastoma may cause more aggressive local bone changes.
Abbreviations
- FLAIR
- fluid-attenuated inversion recovery
- HE
- hematoxylin-eosin
- NF 1
- neurofibromatosis type 1
- NF 2
- neurofibromatosis type 2
- T1WI
- T1 weighted imaging
- T2WI
- T2 weighted imaging
Masses of the sphenoid bone and sphenoid sinus in the pediatric population are uncommon; however, a wide range of pathologies can involve this central skull base structure, including benign and malignant lesions. Several of these entities are specific to pediatric patients, and the presence of skull base abnormalities in children should provoke their consideration. Due to its central location, abnormalities of the sphenoid bone can affect many critical skull base structures. Levine1 described 13 sensitive structures that are at risk in the setting of sphenoid disease: the dura, the cavernous sinus, the internal carotid artery, the oculomotor nerve, the pituitary gland, the optic nerve and chiasm, the trochlear nerve, the ophthalmic nerve, the abducens nerve, the maxillary division of the trigeminal nerve, the sphenopalatine ganglion, the sphenopalatine artery, and the pterygoid canal and nerve.
Preoperative imaging is critical in these patients for proper surgical planning. Appropriately narrowing the preoperative differential diagnoses can aid in treatment planning. For example, lesions such as juvenile angiofibroma, which are highly vascular, may warrant preoperative embolization. It is also important to determine the extent of the lesion into adjacent spaces, including the intracranial compartment. This will affect surgical choices and whether joint sinus and neurosurgical intervention is necessary. While there is overlap in imaging findings between these lesions, some findings can help the radiologist to narrow the differential diagnosis and certain lesions have classic radiographic appearances.
We present an array of pediatric cases of both benign and malignant masses of the sphenoid bone. Histologic images are provided for correlation. The identification of lesions occurring characteristically in a pediatric population and of helpful clinical and radiologic features is emphasized, with attention paid to typical imaging characteristics and patterns of involvement. Some of the cases discussed are common pediatric lesions (juvenile angiofibroma, chordoma); others do not typically occur in children and, when they do, should prompt the search for specific clinical associations (cystic fibrosis and mucoceles, neurofibromatosis type 2 and meningioma); still others are truly rare entities with only a handful of cases previously reported in the literature (giant cell reparative granuloma, metastatic neuroblastoma). We also include an imaging-guided algorithm to aid in the preoperative diagnosis of these lesions (Fig 1).

An imaging-guided algorithm.
Entities Typified by Nonaggressive Osseous Changes
Mucoceles
Mucoceles (Fig 2) are expansile masses most commonly found in the ethmoidal and frontal sinuses.2 They are less common in the sphenoid sinus but have similar imaging characteristics in that location. These are cystic lesions lined with respiratory epithelium and filled with mucoid secretions.3 Mucoceles occur as a result of sinus ostia obstruction following chronic sinus inflammation, polyposis, trauma, surgery, or tumor.4 These masses are rare in children and should warrant a work-up for cystic fibrosis.3 Patients may present with a variety of clinical symptoms ipsilateral to the lesion, ranging from headache to cranial nerve impingement.5

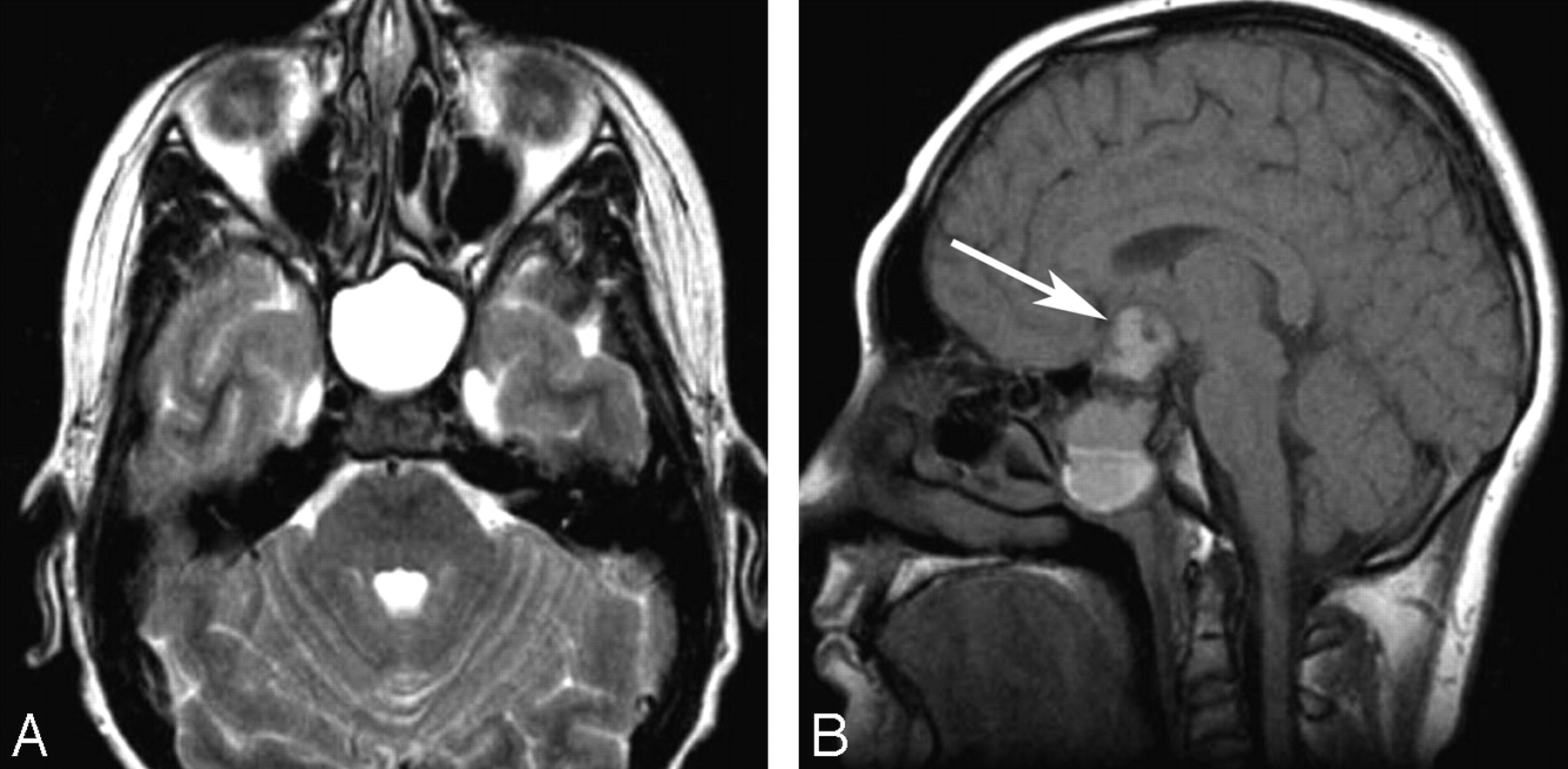
An 18-year-old man with sphenoid mucocele. A, Axial T2WI demonstrates a fluid-filled and expanded sphenoid sinus. B, Sagittal noncontrast T1WI shows a fluid/debris level within the lesion. Relative hyperintense material on T1WI reflects proteinaceous fluid content. There is intracranial extension with loss of the cortical margin of the planum sphenoidale (arrow).
CT demonstrates an isoattenuated smooth mass with bowing and thinning of the osseous margins. The MR imaging appearance is variable, depending on the protein concentration and viscosity of the contents of the lesion; however, usually mucoceles are high intensity on T2WI and can vary in T1 relaxation characteristics. There may be thin rim enhancement2; however, if enhancement is thick or nodular, mucopyocele or neoplasm should be considered. Surgical resection commonly through an endoscopic approach or marsupialization is usually curative.5
Aneurysmal Bone Cyst
Aneurysmal bone cysts, (Fig 3) are non-neoplastic multicystic lesions composed of non-endothelial lined blood-filled spaces. They are most common in individuals between 10 and 20 years of age.6,7 Only 1% of aneurysmal bone cysts occur in the skull, for they are usually found in long bones and vertebrae,8 with a mere handful of case reports9–12 affecting the sphenoid sinus. According to Lichtenstein,7 aneurysmal bone cysts may arise secondary to a circulatory disturbance such as venous thrombosis or arteriovenous malformation. Resulting increased venous pressure within bone is believed to lead the formation of this dilated and engorged vascular lesion. Others say the inciting circulatory disturbance is the result of some other primary lesion such as a giant cell tumor, nonossifying fibroma, chondroblastoma, or fibrous dysplasia, among others. Accordingly, one-third of aneurysmal bone cysts have some other associated lesion.6

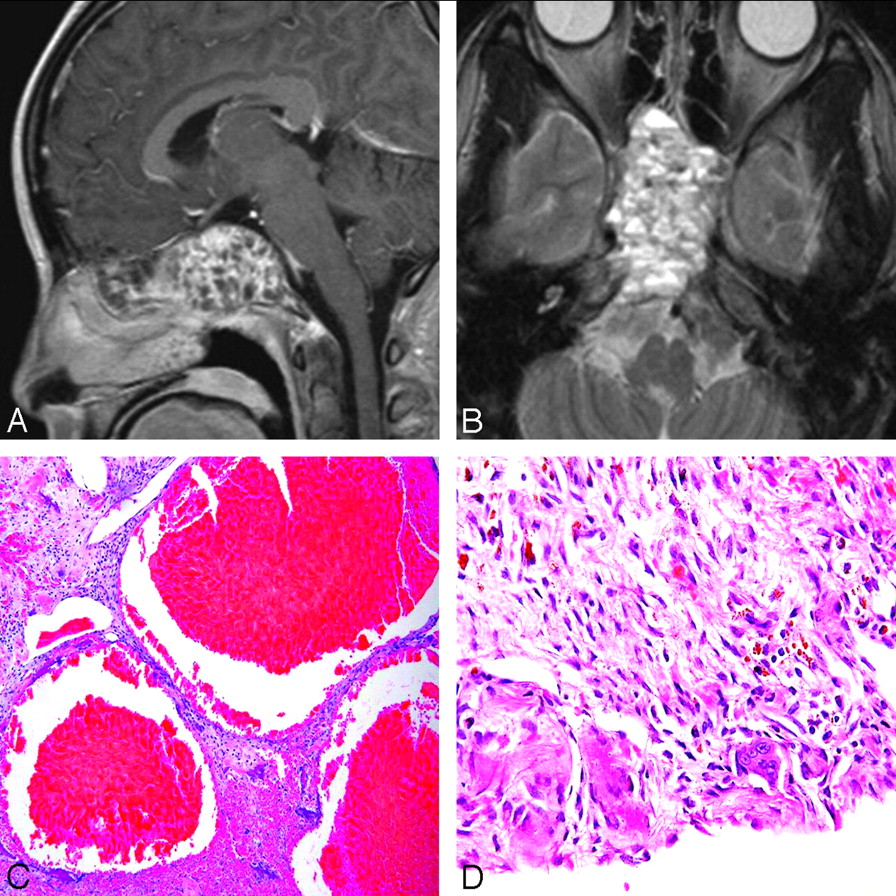
A 19-year-old woman with aneurysmal bone cyst. A and B, Gadolinium-enhanced sagittal T1WI (A) and axial T2WI (B) show multiple fluid/fluid levels in a complex multicystic mass centered on the sphenoid bone, expanding the bone and filling the sphenoid sinus. C, Photomicrograph shows blood-filled cavernous channels at low-power magnification with (HE staining, original magnification ×4). D, Higher power photomicrograph shows spindle cells in the vessel walls, reactive bone formation, and multinucleated giant cells typical of these lesions (HE staining, original magnification ×40).
Clinical symptoms are secondary to pressure and mass effect and include headache, sinus congestion, and cranial nerve palsies.13 Plain films may reveal a complex cystic lesion with a thin shell of periosteal bone.7 CT classically shows a heterogeneous mass with multiple fluid/fluid levels.14,15 MR imaging also shows these fluid/fluid levels, with heterogeneous signal intensity on both T1WI and T2WI and frequently multiple internal septations,16 as a well-defined hypointense capsule.14 Treatment aims at complete surgical excision through a transcranial-transbasal or transfacial approach.17
Giant Cell Lesions
Giant cell lesions include 2 main subtypes: giant cell tumor and giant cell reparative granuloma (Fig 4). These are believed to be related entities but are histologically distinct from one another. Giant cell tumors are true neoplasms, and giant cell reparative granulomas are non-neoplastic reactive lesions.18

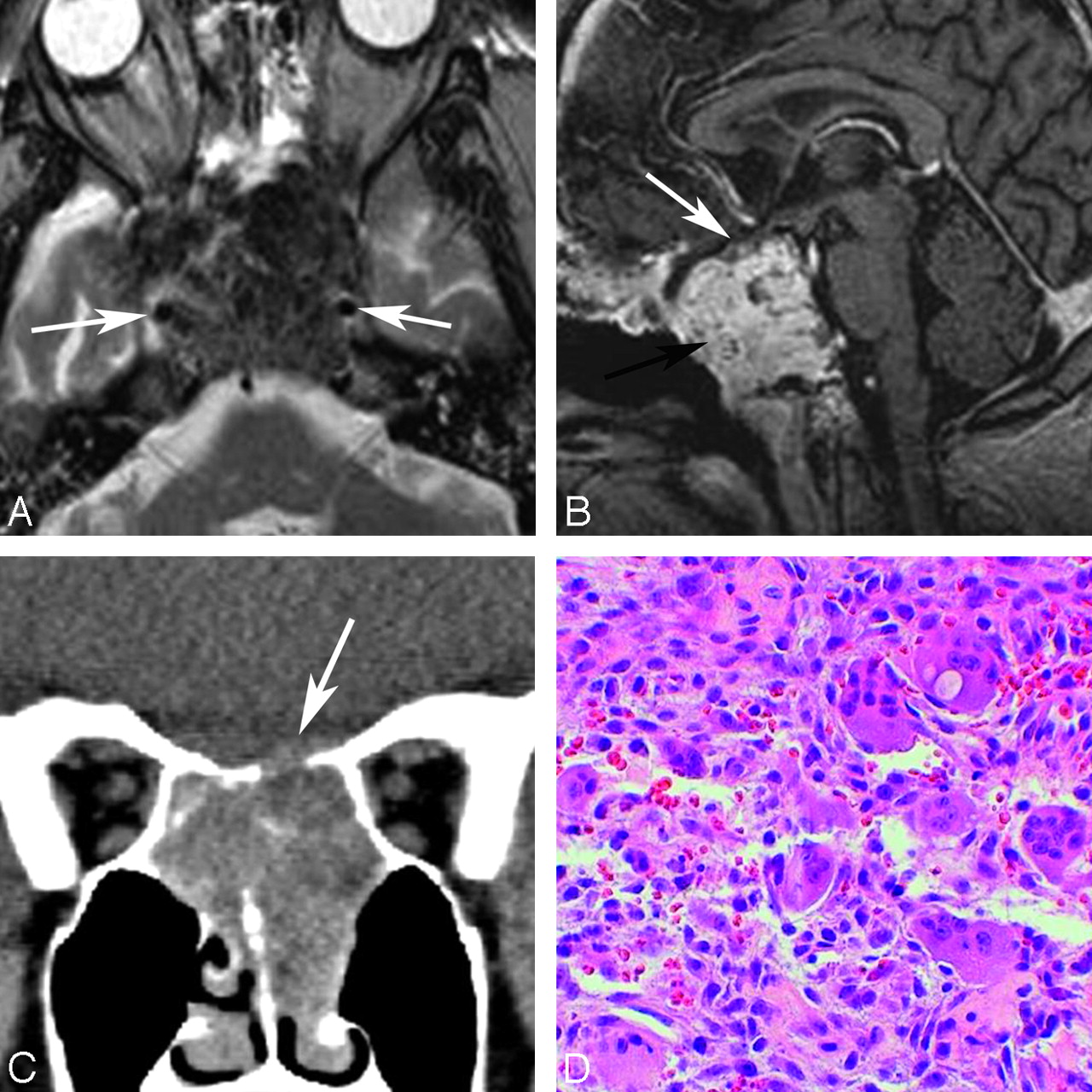
Two patients with giant cell lesions of the sphenoid bone. A, An 18-year-old man with sphenoid giant cell tumor: axial T2WI shows relative hypointense areas within a lesion centered on the sphenoid bone and obliterating the sphenoid sinus cavity. These hypointense areas may represent areas of old blood products and fibrotic change. The carotids are displaced laterally (arrows). B, Gadolinium-enhanced sagittal T1WI shows the lesion avidly enhancing (black arrow). The pituitary gland and sella are displaced cephalad (white arrow). C, A 27-year-old woman with giant cell reparative granuloma. Coronal reformatted image in a soft-tissue window from a noncontrast CT scan shows a soft-tissue mass centered on the sphenoid sinus with dehiscence of the planum sphenoidale (arrow). D, HE stain on the photomicrograph shows giant cells with multiple nuclei, fibrous tissue, and blood products characteristic of this reactive lesion (original magnification ×40).
Giant cell tumors and giant cell reparative granulomas are indistinguishable on imaging. CT shows an osteolytic lesion without surrounding sclerosis and an enhancing soft-tissue mass. MR imaging findings are nonspecific: The lesion is usually isointense to gray matter on T1WI and T2WI and intensely enhancing after contrast administration.19 Areas of low signal intensity may be seen corresponding to fibrosis or blood products.20 There may be fluid/fluid levels similar to those seen in aneurysmal bone cysts; sometimes the 2 lesions are associated and occur together.6
Giant cell tumors are benign neoplasms that may exhibit locally aggressive behavior.21 They are more common in females and have a peak incidence during the fourth decade of life. These are relatively rare in the pediatric population. One report found 7% of giant cell tumors occurring in persons younger than 15 years of age.22 Giant cell tumors occur rarely in the skull, but when they do, they have a predilection for the sphenoid bone and also for the temporal bone.21 Clinical symptoms may include pain, swelling, ophthalmoparesis, and trigeminal hypesthesia.21,22 Imaging reveals a sharply marginated expansile lytic osseous lesion typically without sclerosis. Bone dehiscence may occur, and there is frequently associated contrast enhancement.23 Surgical resection is the treatment of choice, though radiation may be used if gross total resection cannot be achieved. Associated malignancy occurs in approximately 10% of cases, with many of these malignancies occurring after primary treatment with radiation.22
Giant cell reparative granulomas are non-neoplastic lesions that have a more fibrogenic quality than true giant cell tumors. Unlike giant cell tumors, they are most often located in the maxilla and mandible and occur in younger patients.24 Sphenoid bone involvement is rare, and there is only 1 prior report in the literature of 2 patients, 1 of whom was a child.20 Both of these patients had involvement of the lateral sphenoid bone. There have been no prior reports of giant cell reparative granuloma within the sphenoid sinus.
Because there is often a history of antecedent trauma25 and the mass has similar histologic features to aneurysmal bone cyst, several researchers believe giant cell tumor to be a reactive lesion.24 Symptoms are again related to gradual impingement on surrounding structures and may include epistaxis and nasal obstruction.25 Surgical excision is usually curative, and this lesion lacks the high recurrence rate of true giant cell tumors.24
Meningioma
Meningiomas (Fig 5) are benign slow-growing tumors that originate from the outer covering layers of the brain. They are frequently located along the falx, convexity, and the sphenoid ridge.4 Sphenoid ridge meningiomas may result in hyperostosis of the sphenoid bone and enlargement of the sinus cavity, pneumosinus dilatans. It is uncommon for a meningioma to extend into the sphenoid bone and sphenoid sinus.

A 10-year-old female patient with central skull base meningioma invading the paranasal sinuses. Axial postcontrast T1WI demonstrates an enhancing mass within the central skull base. The mass involves the ethmoid and sphenoid sinuses and was a biopsy-proved meningioma. Nonenhancing anterior portion of the sphenoid sinus is filled with secretions (black arrow). Multiple additional schwannomas are seen in the Meckel cave and the internal auditory canal (white arrows) in this patient with neurofibromatosis type 2. Although meningioma is common in adults, in pediatric patients, the lesion is much rarer and occurs in the setting of neurofibromatosis type 2 or prior radiation therapy.
Meningiomas are common lesions in adults but are rare in patients younger than 18 years of age. In fact, they make up only 1%–4% of all intracranial tumors in children.26 Predisposing factors in the pediatric age group include neurofibromatosis type 227 and prior whole brain radiation.28 One study found visual disturbance to be the most common clinical symptom associated with sphenoid meningiomas.29 There may be unilateral exophthalmos or oculomotor nerve involvement resulting in vision loss and diplopia.4
For the most part, pediatric meningiomas and meningioma within the sphenoid sinus share imaging findings with the adult version of the tumor. Angiography demonstrates a hypervascular tumor with displacement of adjacent vessels. On unenhanced CT, the mass is typically hyperattenuated compared with brain. On MR imaging, the tumor is typically isointense on T2WI compared with gray matter, enhances intensely on postcontrast images, and may demonstrate a dural tail.30 Compared with their adult counterparts, a greater number, approximately 12%–24%, of childhood meningiomas contain cysts.31 Surgical resection remains the mainstay of therapy.27
Fibrous Dysplasia
Fibrous dysplasia (Fig 6) is an idiopathic skeletal developmental anomaly that can affect 1 bone (monostotic form) or multiple bones (polyostotic form).32 It often occurs early in life, with an average age of 10 years at onset.33 The skull base is commonly involved. When patients have involvement of multiple bones along with cutaneous lesions and endocrine abnormalities, they are given a diagnosis of McCune-Albright syndrome.24 According to Lichtenstein,33 fibrous dysplasia may stem from a developmental anomaly of bone that results in the medullary cavity becoming filled with fibrous tissue. Lesions of the skull can grow quite large and cause facial deformity, exophthalmos, and narrowing of skull base foramina. The lesions often stop enlarging after puberty.24

A 13-year-old girl with fibrous dysplasia affecting the sphenoid bone. A, Bone window on CT shows classic ground-glass attenuation in the sphenoid bone. B, The sphenoid sinuses are small and demonstrate mucosal disease. The lesion is hypointense on T2WI. C, This MR imaging appearance is likely attributable to the fibrous stroma, illustrated on the photomicrograph with HE stain demonstrating woven bone embedded in a spindle cell stroma (original magnification ×4). Fibrous dysplasia can have extreme heterogeneity on MR imaging and can be a confusing lesion to diagnose. Correlation with CT should always be done.
On plain films, fibrous dysplasia has a classic ground-glass appearance, though involvement of the sphenoid bone may be difficult to appreciate on radiography.2 CT is useful for skull base lesions, when plain film diagnosis is not possible. CT also demonstrates the characteristic ground-glass appearance, often with an associated sclerotic rim.34 MR imaging features of fibrous dysplasia are variable and can be misleading because the lesion may look rather aggressive. Correlation with CT is critical to make the appropriate diagnosis. The lesions may be homogeneously low signal intensity on T1WI and appear variable on T2WI.35 Radionuclide bone scanning may be useful for detecting early polyostotic disease and follow-up. Lesions demonstrate increased radionuclide uptake in both perfusion and static bone imaging.36 These lesions generally have a good prognosis; therefore, treatment should be conservative. Rarely, they may undergo spontaneous malignant transformation, and radiation therapy would increase this risk.24
Hypothalamic/Chiasmatic Astrocytoma
Pilocytic astrocytoma (Fig 7) is a low-grade tumor that can occur anywhere in the central nervous system, but one of the common locations is the hypothalamic/optic region.37 It is not unusual for an astrocytoma in this region to extend into the sellar region. With time, the sella may be expanded and osseous dehiscence may occur along the floor of the sella and planum sphenoidale. Astrocytic tumors that involve the sphenoid bone tend to cause remodeling of the bone seen best on CT. MR imaging demonstrates a hypointense lesion on T1WI and a hyperintense lesion on T2WI.2 Cystic components may be present.37

A 4-year-old girl with hypothalamic astrocytoma. A, Sagittal postcontrast T1WI shows a large enhancing mass extending from the suprasellar region. The lesion expands and fills the sella with remodeling of the sphenoid bone. The sphenoid sinus is small (black arrow). Postoperative changes and artifacts are present (white arrow). B and C, Compact and spongy areas are seen on photomicrographs of histopathologic specimens, correlating to solid and cystic components of the tumor (HE staining; original magnification ×40).
There are 2 main histologic variants: typical and pilomyxoid,38 and both occur most commonly in the pediatric age group. The distinction carries important prognostic implications. Pilocytic tumors occur at a mean age of 4.8 years and have an indolent course with excellent long-term prognosis. On the other hand, the pilomyxoid variant occurs at a younger age (mean age, 1.5 years), has a greater recurrence rate, a greater CSF dissemination rate, and a shorter survival time.37 There is an association with neurofibromatosis type 1.2 Gross total resection is the treatment of choice,39 but surgery is often limited due to morbidity and mortality.40
Entities Typified by Aggressive Osseous Changes
Chordoma
Chordomas (Fig 8) are rare neoplasms that arise from notochordal remnants. They are most commonly found in the spheno-occipital and sacrococcygeal regions.24 In the skull base, chordomas cause aggressive osseous changes and may not only involve the clivus as is typical but also may extend into the intracranial compartment and sphenoid bone and sphenoid sinus. CT shows an enhancing soft-tissue mass with internal densities thought to represent fragments of bone and invasion of surrounding structures. MR imaging is necessary for delineation of tumor extent and shows variable intensity and enhancement on T1WI. High intensity is typical on T2WI.2

Two patients with chordoma involving the sphenoid bone. A, An 18-year-old male patient. Axial T2WI shows a multicystic lesion involving the central skull base, including the sphenoid bone, sphenoid sinus, posterior ethmoids, and left middle cranial fossa. Focal areas of T2 hyperintensity are seen. B, In the coronal reformatted image, a bone window shows dehiscence of the planum sphenoidale (arrow). C, An 11-year-old boy with chordoma. Sagittal noncontrast T1WI shows the lesion to nearly fill the sphenoid sinus. There is a small residual aerated portion of the sphenoid sinus cavity (arrow). D, Photomicrograph shows that neoplastic epithelioid cells form cords in a mucoid background (HE staining; original magnification ×40).
There is a bimodal age distribution for chordomas. Those situated in the skull base occur more frequently in the younger population. From an article by Ridenour et al,41 35 pediatric patients with chordoma were studied and they showed longer survival times compared with their adult counterparts, though it was suggested that this may vary depending on the histologic subtype. Chordomas are twice as common in males as in females,42 and the tumor is locally aggressive with a high recurrence rate.24,42 Patients may present with headache, visual disturbances, or cranial nerve palsies.2 The tumor can also cause mass effect on the pituitary gland, resulting in endocrine symptoms or obstruction of the nasal passages.24 Treatment involves maximum safe resection along with high-dose radiation therapy via proton beam radiation or radiosurgery.43
Craniopharyngioma
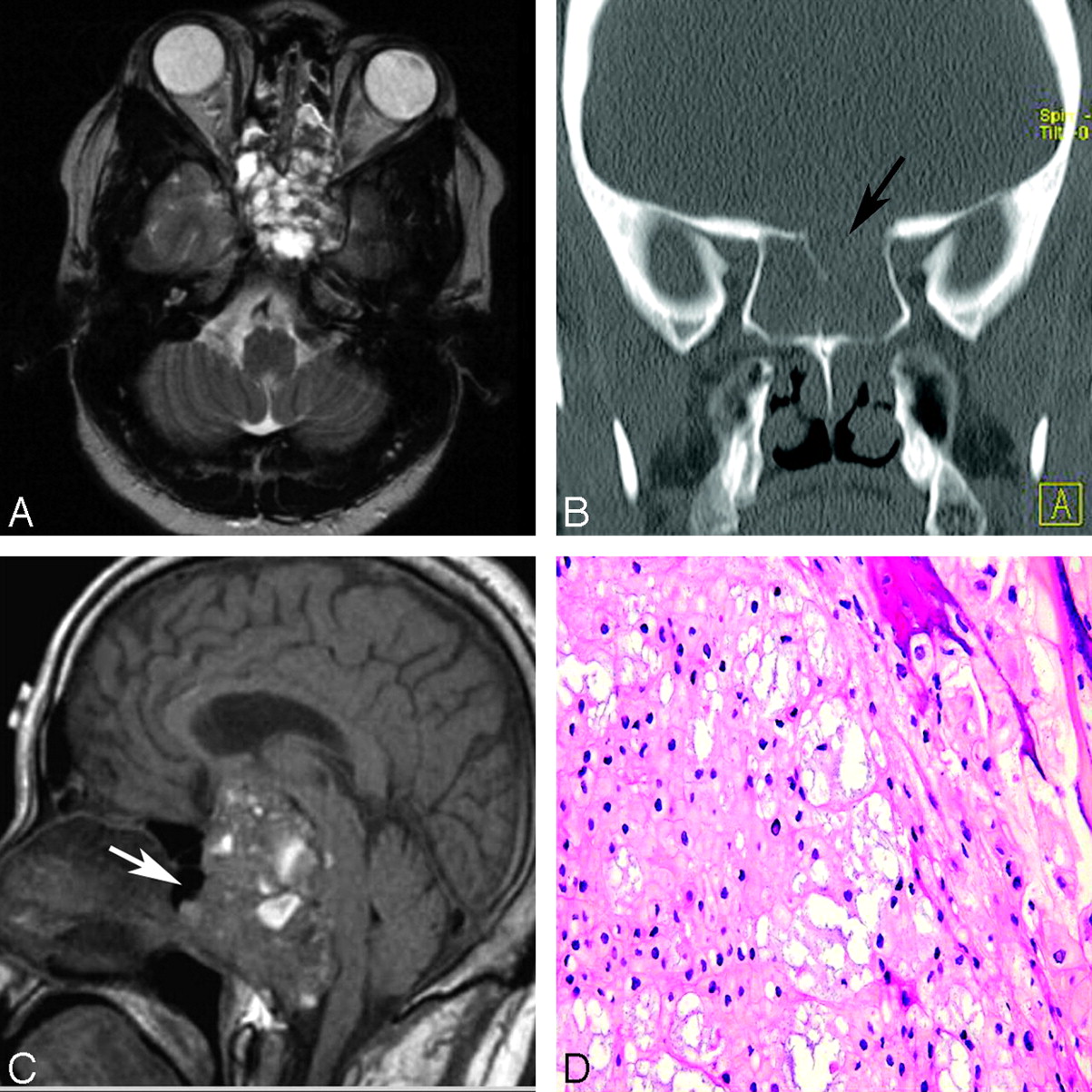
Craniopharyngioma (Fig 9) is a slow-growing benign tumor arising from retained elements of the Rathke pouch, the embryologic forerunner of the anterior pituitary gland.44 There is a bimodal age distribution: school-age children and adults 50–60 years of age.45 There are 2 distinct histologic subtypes: adamantinomatous and papillary. The predominant histology in the pediatric population is adamantinomatous.46 Craniopharyngiomas are predominantly located in the sellar and suprasellar regions, though they may uncommonly descend inferiorly enough to involve the sphenoid bone.47 CT characteristics include heterogeneity, calcification, cyst formation, and contrast enhancement.44 The lesion shows variable signal intensity on T1WI and high signal intensity on T2WI.2 Treatment options are variable, depending on the location of the lesion. Complete surgical resection is frequently easier to achieve in children because they tend to present earlier in the course of disease with less concurrent inflammation and glottic reaction.48

A 12-year-old boy with craniopharyngioma. A, Axial fluid-attenuated inversion recovery image shows the cystic portion of the tumor (black arrow) within the central sphenoid bone (white arrow). There is a fluid/fluid level. B, Photomicrograph of a histopathologic specimen shows findings characteristic of craniopharyngioma, with nests of anucleated squamous cells embedded in fibrous tissue and clefts consistent with cholesterol (HE staining; original magnification ×10).
Rhabdomyosarcoma
Rhabdomyosarcoma (Fig 10) is a malignant neoplasm derived from primitive mesenchymal tissue that expresses myogenic differentiation.49 It can also arise in tissue such as the urinary bladder, which does not normally contain striated muscle.38 There is a bimodal age distribution, with 1 peak during the first decade of life and a second during adolescence.49 The embryonal subtype is more common among infants and young children, with the alveolar subtype tending to occur mainly in adolescents.4 A slight male predilection exists. In 1 study, 36% of rhabdomyosarcomas in children were located in the head and neck.49 Depending on the precise location, these have the potential to invade the skull base. Most cases of rhabdomyosarcoma are sporadic; however, it is believed that a genetic predisposition may exist as evidenced by the association with hereditary disorders including Li-Fraumeni syndrome.50 Patients often present with nasal, aural, or sinus obstruction, with or without mucopurulent or sanguinous discharge.38 CT reveals a poorly defined enhancing soft-tissue mass with aggressive destruction of bone.51 In general, the prognosis for head and neck rhabdomyosarcomas is more favorable than for those arising in other locations due to the earlier stage at presentation, though this may not be true for skull base lesions.49 Complete surgical resection is the goal, but if it is not possible, a combination of surgery, chemotherapy, and radiation is used.50

A 16-year-old boy with rhabdomyosarcoma. A, Bone window from a noncontrast CT examination show opacification of the right-sided paranasal sinuses, including the right sphenoid sinus (arrow). There are areas of dehiscent bone involving the maxillary sinus walls. B, Soft-tissue window shows the lesion involving the right nasal cavity, right maxillary and sphenoid sinuses, right orbit, and right pterygopalatine fossa (white arrow). Note the normal fat within the left pterygopalatine fossa (black arrow).
Juvenile Angiofibroma
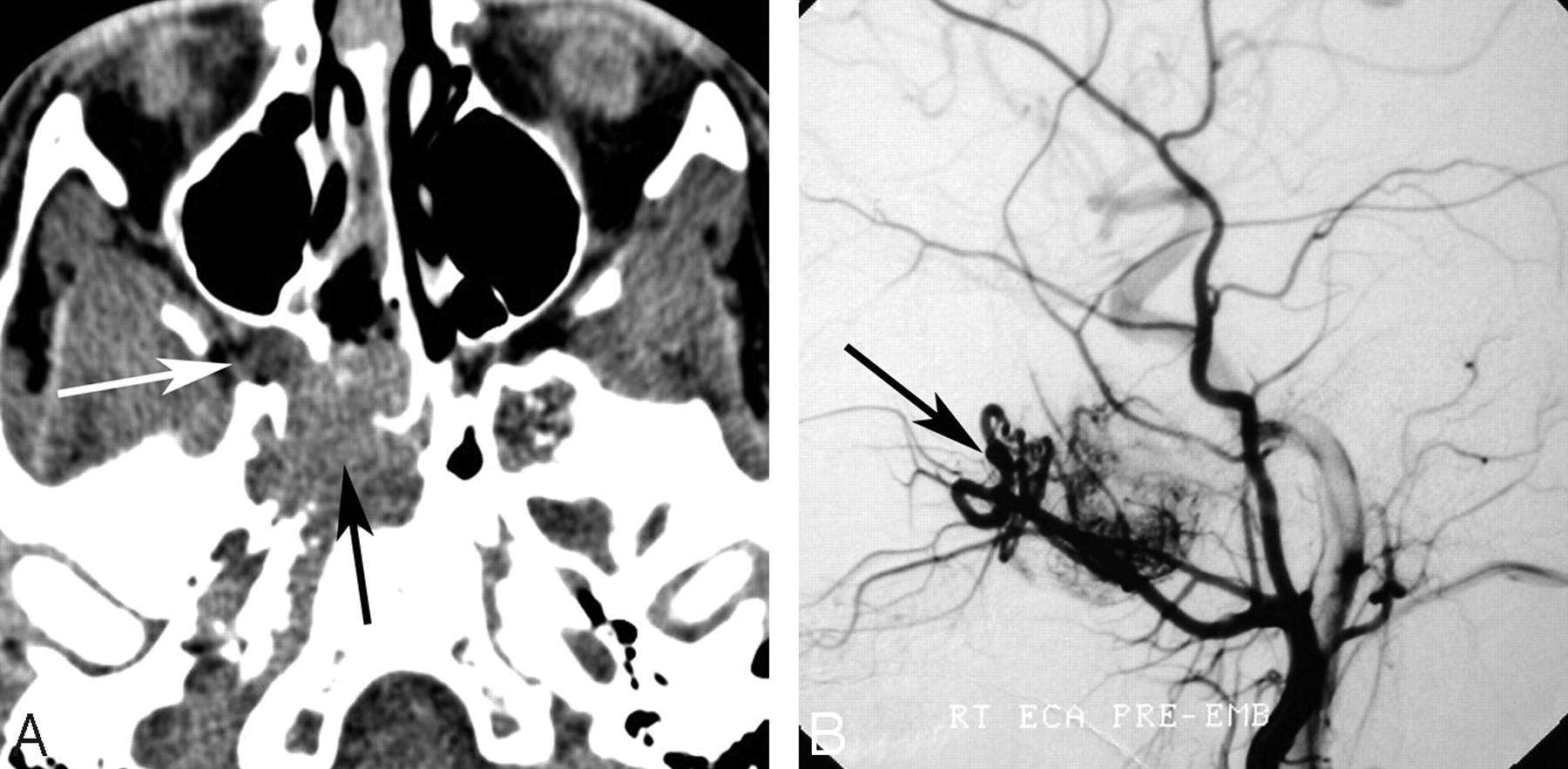
Juvenile angiofibroma (Fig 11) is a highly vascular benign neoplasm occurring in the nasopharynx or posterior nasal cavity. It is locally aggressive and often invades surrounding structures.52 It may invade posteriorly into the sphenoid bone and sinus. According to a study by Witt et al, 53 all juvenile patients with angiofibroma in their series were males between 11 and 21 years of age. Lesions may also arise within the sphenopalatine foramen, the medial egress of the pterygopalatine fossa.2

A 16-year-old boy with juvenile angiofibroma. A, Axial unenhanced CT scan demonstrates widening of the right sphenopalatine foramen with abnormal soft tissue obliterating the normal fat within the pterygopalatine fossa (white arrow). Soft tissue extends anteriorly into the posterior nasopharynx and posteriorly into the sphenoid bone and right sphenoid sinus (black arrow). B, Lateral projection from a right external carotid artery angiogram in the arterial phase demonstrates an attenuated tumor blush and an enlarged internal maxillary artery with tortuous vessels in the right pterygopalatine fossa (arrow).
Patients present with a range of symptoms, including nasal obstruction, exophthalmos, and severe recurrent epistaxis.52 CT shows a lesion isoattenuated to muscle with marked enhancement. Commonly, the lesion causes expansion of the pterygopalatine fossa.54 As the lesion grows, it can cause aggressive bone changes to the skull base, however.55 The lesion is included in this discussion along with other entities that cause aggressive bone changes because when it involves the sphenoid bone, typically the erosive bone changes are aggressive-appearing. On MR imaging, these highly vascular tumors may demonstrate flow voids. Angiography shows an attenuated tumor stain and recruitment of surrounding vessels.2 These tumors frequently begin to regress on their own at puberty.52 Surgery is the treatment of choice. When the tumor involves the sphenoid sinus and has limited infratemporal fossa involvement, an endoscopic approach can be used.56 Preoperative embolization may be useful56 because the lesions are highly vascular and blood loss during surgery can be significant.53
Sinonasal Carcinoma
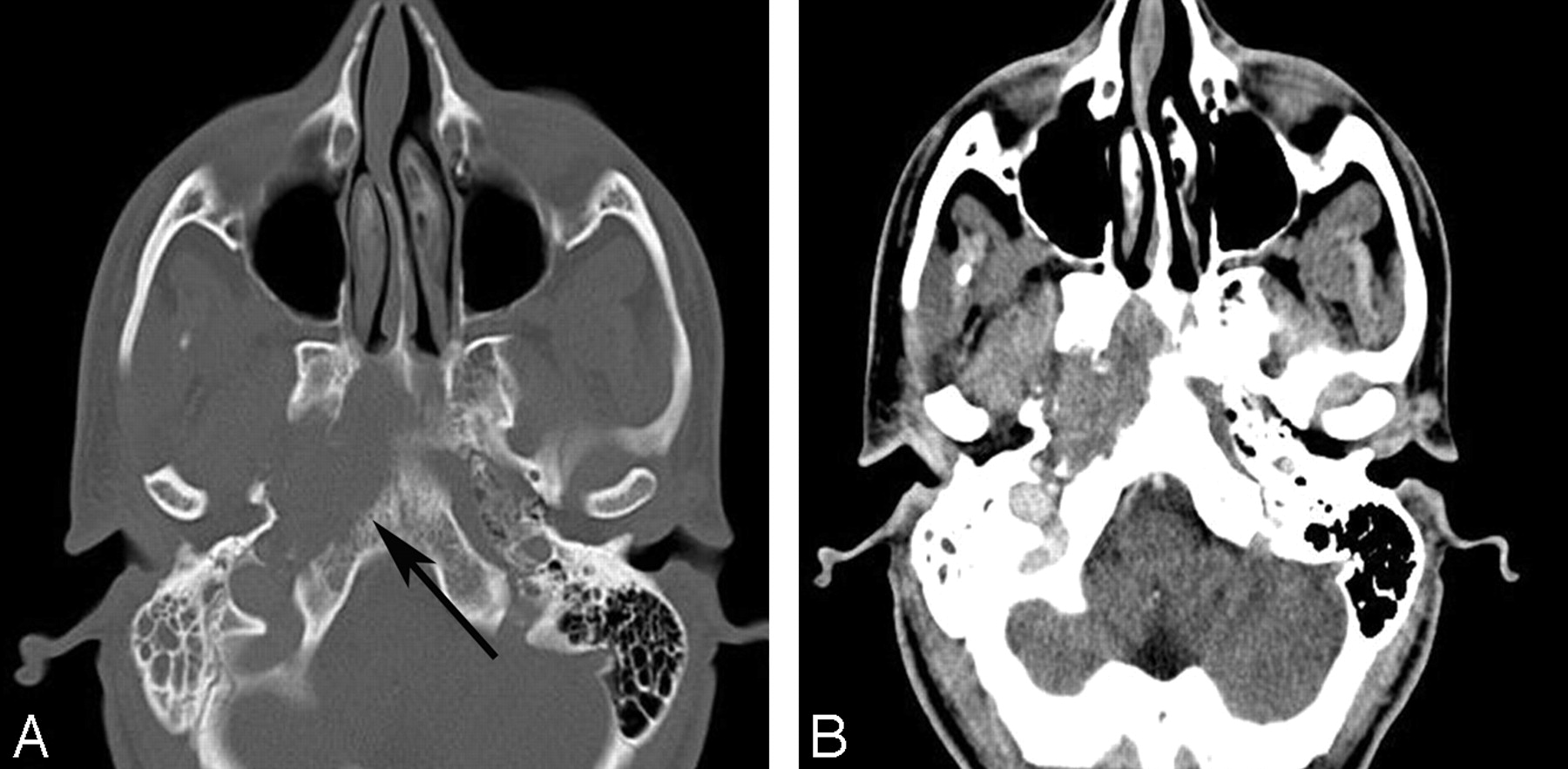
Sinonasal carcinoma (Fig 12) is generally thought of as an adult tumor, though when one is dealing with pediatric patients, this entity should not be forgotten.57 The mass usually presents with locally advanced disease.58 The most common histologic subtypes are squamous cell carcinoma and adenocarcinoma. Nasopharyngeal primaries may invade posteriorly and superiorly into the skull base. Only 2% of nasal and paranasal squamous cell carcinomas are primary to the sphenoid sinus.58 CT is useful for demonstrating bone destruction, but MR imaging is better for mapping soft-tissue extent. Treatment includes a combination of surgery, chemotherapy, and radiation therapy.59

A 20-year-old man with sinonasal carcinoma. A, Bone window from an unenhanced CT scan shows destructive osseous changes (arrow). B, Soft tissue window at the same level shows an associated soft tissue mass in the right central skull base.
Neuroblastoma
Neuroblastoma (Fig 13) arises from primitive sympathetic neuroblasts of the embryonic neural crest.60 It is the most common solid tumor in children, with a median age at diagnosis of 19 months.38 Head and neck lesions are typically metastases.4 Neuroblastomas can be clinically silent until they invade or compress adjacent structures, metastasize, or produce paraneoplastic syndromes.60 One previous case report of a patient with neuroblastoma metastasis to the sphenoid sinus described symptoms of vision loss, frontal bossing, prominent vessels on the forehead, periorbital ecchymoses, and bilateral mild proptosis.61

A 3-year-old girl with neuroblastoma. A, Sagittal postcontrast T1WI shows a mass centered on the sphenoid bone, an unusual location for a neuroblastoma metastasis, obliterating the sphenoid sinus. There is mass effect on the gyrus rectus. B, A multilobulated mass demonstrates characteristic relative hypointense signal intensity on an axial T2WI. The lesion has an intracranial component, extending along the anterior aspect of the middle cranial fossae bilaterally (arrows). C, The left adrenal primary is shown on coronal postcontrast T1WI of the abdomen.
On imaging, metastatic neuroblastoma may have calcifications and cystic components and frequently appears as an area of mottled bone destruction when bone is involved. CT of the abdomen may reveal the primary tumor.62 MR imaging characteristics are nonspecific, and the lesion is typically low intensity on T1WI and high intensity on T2WI.63 Depending on stage, age, and tumor pathology, treatment may consist of surgery, chemotherapy, or radiation therapy.38
Summary
Pediatric masses involving the sphenoid bone and sinus are rare but deserve special attention because of their location within the central skull base. When faced with a pediatric sphenoid mass, one should consider certain entities. In many cases, CT and MR imaging are complementary studies and important for preoperative evaluation. While the imaging findings of these lesions overlap, specific imaging patterns may help to narrow the differential diagnoses. Postoperative imaging is also crucial to watch for lesion recurrence because of difficulties in attaining gross total resection.
Indicates open access to non-subscribers at www.ajnr.org
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}