
Article Figures & Data
Figures
- Fig 1.
A, I-123 iomazenil SPECT image. B, Automatic coregistration of the I-123 SPECT image with the MR image. The maps are simultaneously reformatted to a matrix that is the same size as the referenced smoothed gray matter map. C, 3D MR image obtained before surgery. D, The MR image is segmented into a gray matter map. E, The gray matter probability map is subsequently binarized. F, Binary map for gray matter convoluted with the point-spread function (smoothed gray matter map). G, Smoothed gray matter map masked by the image E. The coregistered I-123 SPECT image is divided by using the masked smoothed gray matter map on a voxel-by-voxel basis. H, Image B anatomically normalized by the spatial normalization matrices generated in the segmentation process. I, Image G anatomically normalized in the same manner as image H.
- Fig 2.
Samples of the VOI set in the left mesial temporal lesion (A) and the right frontal lesion (B). The uniform size of spheric VOI was established. The size of the VOI (16 mm in diameter) was determined so as to be included in any resected lesion and located in the center of the resected lesion in reference to an MR image acquired after the surgery.
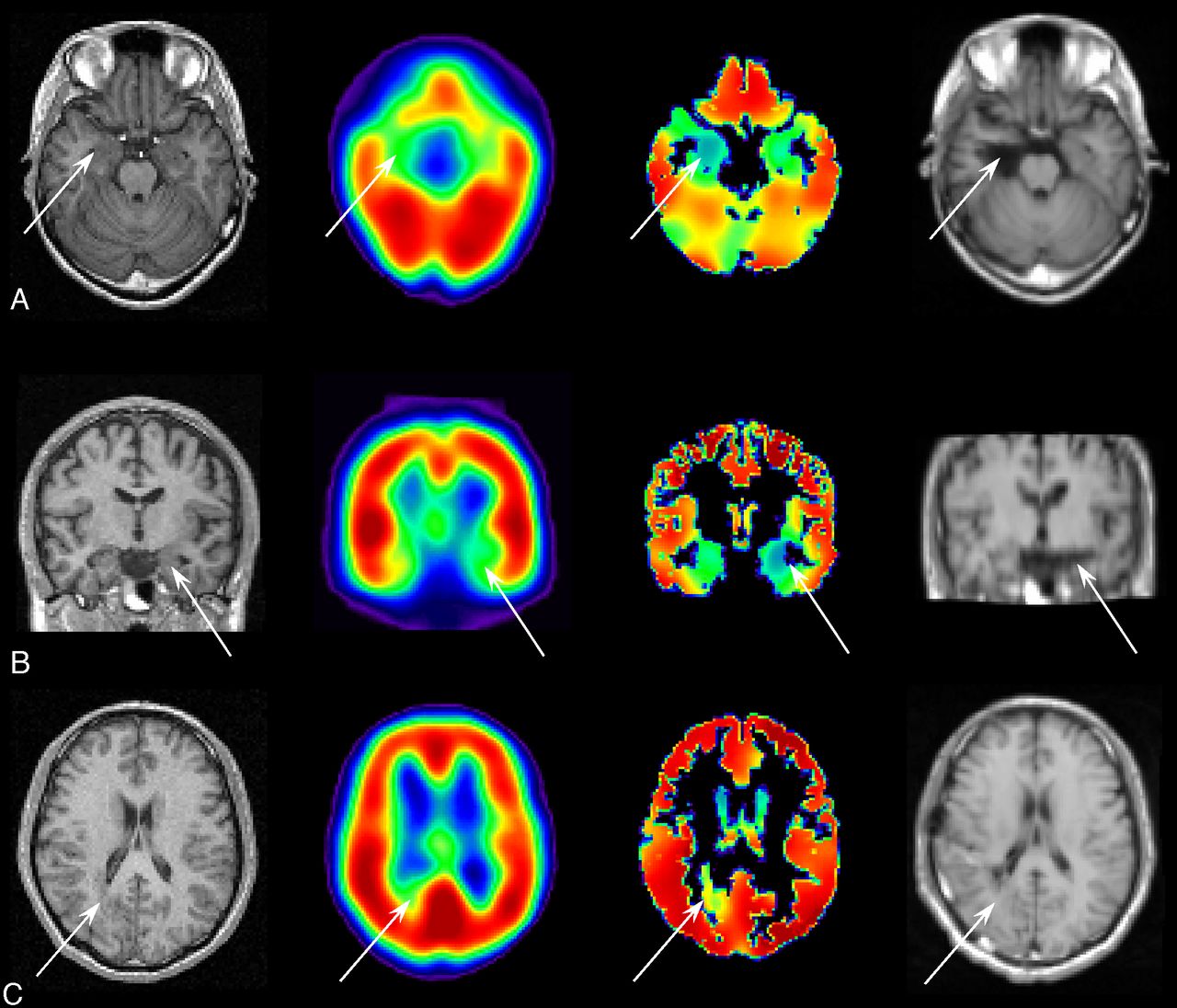
- Fig 3.
MR imaging acquired before surgery (far left column), uncorrected SPECT (the second column from the left), PVE-corrected SPECT (the third column from the left), and MR imaging acquired after surgery (far right column). Arrows indicate the location of resected lesions. A, A case of glioma without any remarkable findings in the uncorrected SPECT, showing a count decrease detected in the PVE-corrected SPECT in the right mesial temporal region. Right mediobasal temporal corticectomy was performed and the postoperative outcome after a 2-year follow-up period was Engel class Ia. B, A case of mesial temporal sclerosis without any remarkable findings in the uncorrected SPECT, showing a count decrease in the PVE-corrected SPECT in the left mesial temporal region. Left selective amygdalohippocampectomy was performed and the postoperative outcome after 2-year follow-up was Engel class Ia. C, A case of heterotopias showing a slight increase in the uncorrected SPECT and a count decrease in the PVE-corrected SPECT in the right temporo-occipital subcortical region. Lesionectomy in the temporo-occipital subcortical area was performed, and the postoperative outcome after 2-year follow-up was Engel class Ia.



Tables
Demographic No. Total 75 Focus laterality Right 35 Left 40 Focus location Temporal 57 Frontal 13 Parietal 1 Occipital 2 Temporo-occipital 1 Parieto-occipital 1 Histologic diagnosis MTS 34 MCD Cortical dysplasia 8 Tuberous sclerosis 2 Heterotopia 1 Tumor Glioma 8 Ganglioglioma 3 Amygdalar hamartoma 3 Angioma 3 DNT 3 Nonspecific No remarkable abnormality 8 Atrophy 2 Prognosis (Engel classification)a Ia 44 Ib 9 Ic-d 0 IIa 0 IIb 22 IIc-d 0 III 0 IV 0 Medicationb CBZ 52 PHT 34 PB 18 VPA 11 CLB 14 DZP 1 CZP 4 Application of invasive EEGc No 52 Yes 23 -
Note:—DNT indicates dysembryoplastic neuroepithelial tumor; CBZ, carbamazepine; PHT, phenytoin; PB, phenobarbital; VPA, sodium valproate; CLB, clobazam; DZP, diazepam; CZP, clonazepam.
↵a Class I: Free of disabling seizures. a, Completely seizure-free since surgery. b, Nondisabling simple partial seizures only since surgery. c, Some disabling seizures after surgery, but free of disabling seizures for at least 2 years. d, Generalized convulsions with antiepileptic drug discontinuation only. Class II: Rare disabling seizures. (“almost seizure-free”) a, Initially free of disabling seizures but has rare seizures now. b, Rare disabling seizures since surgery. c, More than rare disabling seizures since surgery, but rare seizures for the last 2 years. d, Nocturnal seizures only. Class III: Worthwhile improvement. a, Worthwhile seizure reduction. b, Prolonged seizure-free intervals amounting to greater than half the follow-up period, but not <2 years. Class IV: No worthwhile improvement. a, Significant seizure reduction. b, No appreciable change. c, Seizures worse.
↵b Use of anticonvulsants at the time of I-123 iomazenil SPECT examination.
↵c Group of patients who underwent 2-step surgery: intracranial EEG electrode implantation and foci resection. This group comprised 5 cases of MTS, 6 cases of MCD, 7 tumors, and 5 healthy patients.
-
No. Sensitivity (%) Specificity (%) Accuracy (%) Pre-PVC Post-PVC P Pre-PVC Post-PVC P Pre-PVC Post-PVC P Total 75 49 85 <.001 69 85 .003 43 84 <.001 Histologic diagnosis MTS 34 70 93 .004 90 93 NS 67 93 .001 MCD 11 50 90 NS 60 80 NS 30 80 .06 Tumor 20 28 83 <.001 56 83 .06 28 83 <.001 Nonspecific 10 40 60 NS 40 60 NS 30 60 NS Foci location Mesial temporal 41 56 90 <.001 78 90 NS 51 90 <.001 Neocortex 34 41 79 <.001 59 79 .03 32 76 <.001 Invasive EEG Noa 52 56 90 <.001 73 88 .01 48 88 <.001 Yesb 23 35 74 .004 61 78 NS 30 74 .002 Histologic Diagnosis No. Mean AI (%) (SD) Mean AI (%)/CV (%) (SD) Pre-PVC Post-PVC P Pre-PVC Post-PVC P MTS 34 23 16 22 16 NS 0.76 (0.52) 1.1 (0.80) <.001 MCD 11 18 (17) 25 (17) .01 0.55 (0.49) 1.3 (0.82) <.001 Tumor 20 14 (15) 17 (16) <.001 0.44 (0.43) 0.89 (0.81) <.001 Nonspecific 10 16 (22) 14 (16) NS 0.62 (0.98) 0.72 (0.83) NS -
Note:—NS indicates not significant.
-
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.