
Abstract
SUMMARY: Establishing the diagnosis of morning glory disc anomaly is crucial to appropriate patient treatment. Although typically made clinically, the diagnosis is not always straightforward, especially in circumstances where physical examination is limited. The goal of this study was to define the spectrum and frequency of orbital findings in a series of patients with funduscopically-confirmed morning glory disc anomaly by using MR imaging. MR imaging demonstrated 3 findings in all patients: 1) funnel-shaped morphologic pattern of the posterior optic disc with elevation of the adjacent retinal surface; 2) abnormal tissue associated with the distal intraorbital segment of the ipsilateral optic nerve, with effacement of the regional subarachnoid spaces; and 3) discontinuity of the uveoscleral coat. These findings were not observed in any of the unaffected globes of the study patients. In summary, these consistent and characteristic findings of morning glory disc anomaly should allow for accurate differentiation from other ocular anomalies and have the potential to guide appropriate management of this patient population.
ABBREVIATIONS:
- MGDA
- morning glory disc anomaly
Morning glory disc anomaly (MGDA) is a congenital optic nerve anomaly characterized by a funnel-shaped excavation of the posterior globe that incorporates the optic disc.1 The term was first coined in 1970 by Kindler,2 who noted the resemblance of the malformed optic nerve to the morning glory flower. The funduscopic appearance of the MGDA includes 3 primary features: an enlarged, funnel-shaped excavation in the optic disc; an annulus of chorioretinal pigmentary changes that surrounds the optic disc excavation; and a central glial tuft overlying the optic disc.3 A radial orientation of unusually straight and narrow retinal blood vessels emerging from the periphery of the abnormal disc is an additional diagnostic feature.4 MGDA has been reported to be associated with other ocular anomalies and numerous intracranial abnormalities including midline craniofacial and skull base defects, vascular abnormalities, and cerebral malformations.1,3,5–14
Establishing the correct diagnosis of MGDA guides appropriate ophthalmic management and should also prompt a search for associated intracranial abnormalities.4 Although the diagnosis of MGDA is typically made clinically, imaging may provide added value in several ways. First, when the clinical picture is not definitive, identification of specific features on imaging may serve to establish the diagnosis and reveal the extent and character of associated ocular abnormalities. For example, confusion often arises in distinguishing MGDA from optic nerve coloboma clinically. This distinction is important because of the implications for genetics and family counseling; MGDA is almost universally a sporadic condition whereas optic nerve coloboma is commonly familial and may occur in association with multisystem congenital malformation syndromes.7,15,16 Second, cross-sectional imaging allows for evaluation of the globe in the setting of associated opacities of the refractive media, including persistent hyperplastic primary vitreous, which may mitigate the capacity to make this diagnosis on the basis of the funduscopic examination alone.17 Finally, these patients may undergo imaging for unrelated clinical issues, and identification of the MGDA at imaging may be the only indicator to search for known associated intracranial abnormalities.
Findings in MGDA at cross-sectional imaging have been reported in several case studies. In particular, several groups have reported a defect in the posterior aspect of the globe, presumed to reflect the optic disc excavation observed clinically.17–19 Auber and O'Hara3 have expanded this work by identifying fluffy hyperintense tissue on T1-weighted MR images immediately adjacent to the “funnel-shaped” abnormality of the optic disc, a finding that may represent an imaging correlate of the chorioretinal pigmentary disturbance.3 Unfortunately, these previous reports of at most 2 patients make it difficult to determine the consistency with which individual findings occur in this clinical setting. Furthermore, in our experience, the orbital findings of MGDA at high-quality imaging are not only highly characteristic for this entity but are also of greater breadth than what has been previously reported. The goal of our study was to characterize the spectrum and frequency of orbital findings in a series of patients with MGDA by using MR imaging and to explore the pathogenesis of this optic nerve anomaly on the basis of these radiographic features.
Case Series
Patients
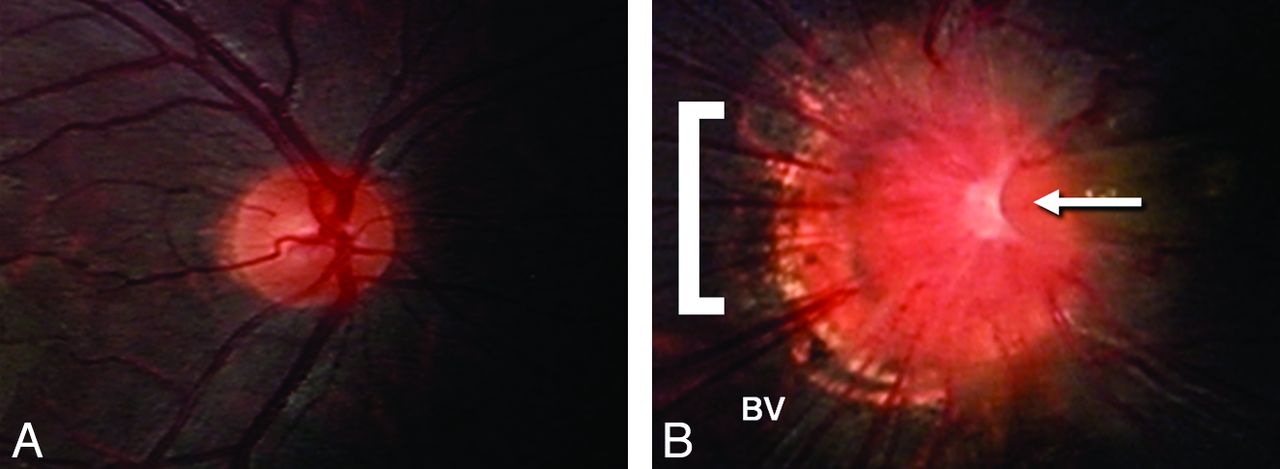
This study was compliant with the Health Insurance Portability and Accountability Act and was approved by the local institutional review board. Patients were identified retrospectively from a search of existing patient data. Inclusion in this study was based on the following criteria: 1) pediatric age group (≤18 years); 2) confirmed diagnosis of MGDA, based on ophthalmologic examination; and 3) an MR imaging examination of the brain and orbits. A total of 6 patients (age range, 8 months–2 years; 3 boys, 3 girls) with a diagnosis of MGDA at funduscopic examination (Fig 1) comprised the final study group.

Fundus photos illustrating normal right optic nerve (A) and morning glory optic nerve anomaly (B). Note the larger overall size, central glial tuft (arrow), halo of pigmentary changes surrounding the nerve (bracket), and the radial orientation of the blood vessels (BV) emanating from the anomalous optic nerve.
MR Imaging
Patients underwent MR imaging with a 3T Tim Trio MR scanner (Siemens, Erlangen, Germany) or a 1.5T Signa TwinSpeed MR scanner (GE Healthcare, Milwaukee, Wisconsin). Representative imaging protocols are as follows:
3T system: 1) Sagittal magnetization-prepared rapid acquistion of gradient echo of the brain (TR, 2530 ms; TE, 3.39 ms; number of acquisitions, 1; flip angle, 7°; TI, 1450 ms; FOV, 22 cm; acceleration factor, 2; voxel size, 1 × 1 × 1 mm). 2) Axial FSE T2-weighted imaging of the brain (TR, 11,730 ms; TE, 89 ms; number of acquisitions, 2; flip angle, 120°; FOV, 20 cm; acceleration factor, 2; voxel size, 0.6 × 0.4 × 2.5 mm). 3) Axial FLAIR imaging of the brain (TR, 9000 ms; TE, 137 ms; TI, 2500 ms; number of acquisitions, 1; flip angle, 150°; FOV, 20 cm; acceleration factor, 2; voxel size, 0.6 × 0.6 × 4 mm). 4) Axial and coronal high-resolution fat-saturated T2WI of the orbits (TR, 6000 ms; TE, 94 ms; number of acquisitions, 3; flip angle, 120°; FOV, 16 cm; acceleration factor, 2; voxel size, 0.6 × 0.4 × 2 mm). 5) Axial and coronal high-resolution T1WI (TR, 605 ms; TE, 10 ms; number of acquisitions, 2; flip angle, 90°; FOV, 16 cm; voxel size, 0.4 × 0.3 × 2 mm).
1.5T system: 1) Sagittal T1WI of the brain (TR, 459 ms; TE, 10 ms; number of acquisitions, 2; flip angle, 90°; FOV, 16 cm; voxel size, 0.7 × 0.6 × 4 mm). 2) Axial FSE T2WI of the brain (TR, 4050 ms; TE, 102 ms; FOV, 20 cm; voxel size, 0.6 × 0.4 × 4 mm). 3) Axial FLAIR imaging of the brain (TR, 10,000 ms; TE, 160 ms; TI, 2200 ms; FOV, 20 cm; voxel size, 0.6 × 0.4 × 2.5 mm). 4) Axial and coronal high-resolution fat-saturated T2WI (TR, 5230 ms; TE, 118 ms; number of acquisitions, 3; flip angle, 150°; FOV, 16 cm; acceleration factor, 2; voxel size, 0.5 × 0.4 × 3 mm). 5) Axial and coronal T1WI (TR, 400 ms; TE, 10 ms; number of acquisitions, 2; flip angle, 90°; FOV, 16 cm; voxel size, 0.6 × 0.6 × 3 mm).
All images were acquired with standard phased array coils: a 32-channel head coil for 3T and an 18-channel head-and-spine coil for 1.5T.
Image Review and Analysis
All imaging examinations were reviewed by 2 pediatric neuroradiologists (M.J.P. and S.E.), each with a minimum of 5 years of dedicated subspecialty experience in neuroradiology. Specifically, the presence or absence of the following orbital findings was evaluated and tabulated: 1) funnel-shaped morphologic pattern of the optic disc; 2) elevation of the adjacent retinal surface; 3) dehiscence and abnormal morphologic features of the uveoscleral coat at the optic nerve insertion, manifest as discontinuity of the normal ring of T2 hypointensity (and enhancement) that reflects the sclera, choroid, and lamina cribrosa20; 4) abnormal tissue associated with the distal intraorbital segment of the optic nerve (ipsilateral to the MGDA); 5) effacement of the subarachnoid spaces of the distal optic nerve sheath (ipsilateral to the MGDA) resulting from this abnormal tissue; 6) fat within the distal optic nerve sheath; 7) enhancement within the distal optic nerve; and 8) size of the globe. Associated intracranial findings were also noted, with particular attention to the following features: 1) skull base abnormalities, including cephaloceles; 2) evidence of Moyamoya disease; 3) callosal dysgenesis; and 4) midline facial defects.5–7,11,13,18,21,22
Imaging Findings
Orbital Findings.
Although most patients had unilateral retinal abnormalities at fundoscopy (n=5), 1 patient was diagnosed with bilateral MGDA. MR imaging results demonstrated a funnel-shaped morphologic pattern of the optic disc with elevation of the adjacent retinal surface in all patients (Fig 2A). This elevated region demonstrated hyperintensity in all patients on the T1WI (Fig 2B). Also observed in all patients was abnormal tissue associated with the distal intraorbital segment of the ipsilateral optic nerve; this tissue was associated with effacement of the subarachnoid spaces (Fig 2A). Posterior discontinuity of the uveoscleral coat across the lamina cribrosa was also observed in all patients (Fig 2A). In a similar fashion, in patients who received gadolinium, there was discontinuity of the posterior choroidal–lamina cribrosa enhancement. These findings were not observed in any of the contralateral unaffected globes of the study patients (excluding the patient with bilateral MGDA). Less consistent orbital findings included the following features: 1) fatty infiltration of the distal optic nerve sheath (n=3; Fig 3A), 2) enhancement within the distal aspect of the optic nerve (n=2; Fig 3B), 3) small size of the globe containing the MGDA (n=2), and 4) retinal detachment (n=1) (Table).

A, Axial fat-saturated T2WI through the orbits of a patient with right MGDA demonstrates a funnel-shaped morphologic pattern of the optic disc (white arrow) with elevation of the adjacent retinal surface. This image also demonstrates abnormal tissue associated with the distal intraorbital segment of the ipsilateral optic nerve and effacement of the subarachnoid space at that level (white arrowhead). Also note discontinuity of the uveoscleral coat at the optic nerve insertion (compare with normal left globe where the curvilinear hypointensity of the uveoscleral coat is continuous across the lamina cribrosa; black arrowhead). B, Axial T1WI demonstrates hyperintensity within the elevated region of the retina (white arrow) as well as fat within the distal optic nerve sheath (white arrowheads).

A, Axial T1WI through the orbits of a different patient with right-sided MGDA again demonstrates fat within the distal optic nerve sheath (white arrowheads). B, Axial gadolinium-enhanced fat-saturated T1WI through the orbits in the same patient demonstrates enhancement in the region of the distal optic nerve (white arrowheads), which is thought to represent displaced choroidal tissue, perhaps in concert with glial, fibrous, and pigment epithelial proliferation. Careful inspection and cross-correlation established the locale of enhancement to be immediately internal to the fat in the optic nerve sheath. Of note, the fat within the nerve sheath is saturated on this sequence, confirming its identity. These images also demonstrate an associated retinal detachment; the patient is status post a scleral banding procedure.
Patient characteristics and imaging findings in MGDA
Extraorbital Findings.
Enlargement of the prechiasmatic segment of the ipsilateral optic nerve, consistent with optic nerve glioma, was observed in 1 patient. Asymmetry of the optic chiasm, abnormally small contralateral to the MGDA, was observed in 1 patient. One patient had evidence of internal carotid steno-occlusive vasculopathy with collaterals, consistent with Moyamoya disease. Finally, persistence of the craniopharyngeal canal was observed in 1 patient; in this case, there was mildly anomalous positioning of the pituitary gland within the proximal aspect of the canal. No evidence of midline facial defects, callosal dysgenesis, or basal cephaloceles was identified in the study population (Table).
Discussion
Here we report the MR imaging findings in 6 patients with MGDA confirmed by funduscopic examination. Consistent orbital findings included the following features: 1) funnel-shaped morphologic pattern of the optic disc associated with elevation of the adjacent retinal margins, 2) abnormal tissue associated with the distal intraorbital segment of the ipsilateral (to the MGDA) optic nerve, 3) effacement of the regional subarachnoid spaces on the basis of this soft tissue, and 4) discontinuity of the normal uveoscleral coat at the optic nerve insertion. This constellation of findings has not been reported in other ocular abnormalities and may serve to establish the radiologic diagnosis of MGDA.
Our observations are consistent with the few previous imaging studies of MGDA. Hu17 reported protrusion of the vitreous through a defect in the posterior wall of the globe by using CT in 6 patients with MGDA and forebrain defects. Several studies have also used MR imaging to describe MGDA. Görbe et al18 reported a posterior excavation of the optic disc in 1 patient with MGDA associated with multiple cerebral malformations; in a similar fashion, Tonami et al19 reported a “colobomatous area” in the region of the optic disc associated with retinal detachment in 1 patient with morning glory syndrome. Auber and O'Hara3 described intraorbital but extraocular findings in a report of 2 patients. In addition to an enlarged, funnel-shaped optic disc with overlying fluffy T1 hyperintense material, they observed enhancement at the distal aspect of the optic nerve in a very similar configuration to that observed in 2 of our patients. Of interest, this study also demonstrated an abnormal aggregate of fat within the optic nerve of 1 patient. In contradistinction to our observations, however, this fat was remote from the optic disc and was not clearly confined to the nerve sheath. Our observations broaden the constellation of ocular findings of the MGDA and, furthermore, establish a set of consistent and characteristic orbital imaging findings for this entity. It is worth noting that, although a detailed description of the MR imaging findings in optic nerve coloboma is beyond the scope of our methodology, retinal elevation, soft tissue in the distal aspect of the optic nerve, and optic nerve sheath fat have not been reported in association with this entity.23,24
The embryologic basis for the development of MGDA has yet to be elucidated. In the minority of patients, MGDA may occur in association with midline facial defects, callosal dysgenesis, and basal encephalocele. On the basis of the overlapping critical periods of development for the frontonasal process, midfacial structures, and primordium of the eyes, this so-called morning glory syndrome is believed to emerge from a single insult occurring during induction of the forebrain. However, the nature of the embryologic defect that leads to the MGDA itself remains the subject of debate. Superficial similarities initially prompted consideration of MGDA as a part of the optic nerve coloboma spectrum, a disorder that results from incomplete closure of the embryonic fissure. However, most now consider MGDA to be a distinct entity that develops as a result of combined dysgenesis of both ectodermal and mesodermal elements.2 On the basis of histopathologic analyses, it has been hypothesized that MGDA results from a defect in the maturation of the posterior sclera that results in a failure of normal fusion and allows the optic disc, lamina cribrosa, peripapillary retina, and choroid to herniate posteriorly.25,26 Also observed in these studies has been a marked lack of mature differentiation of the sclera, with the outer surface being replaced by disorganized spindle cells arranged in a coarse reticular form resembling that of embryonic mesenchyme.25,26 The optic nerve sheath may demonstrate similar findings and, in addition, contained localized aggregations of fat with a loose areolar appearance.25,26
This theory, along with previously published pathologic images, closely parallels and informs our observed MR imaging findings. According to this theory, the consistently observed dehiscence of the posterior uveoscleral coat may, in fact, represent the primary abnormality of the MGDA. The abnormal tissue we observed at the distal optic nerve may then reflect evagination of the choroid and peripapillary retina into the perineural space with associated effacement of CSF. Enhancement in this region is presumably related to the displaced choroidal tissue, perhaps in concert with glial, fibrous, and pigment epithelial proliferation.25,26 The observed retinal depression, therefore, likely represents a “false physiologic pit, formed by the coapted internal surface of the prolapsed retina”.25 Finally, elevation of the adjacent optic disc margins may result from some combination of retinal folding and redundancy; thickening of the retina because of pseudofibrotic metaplastic retinal pigment epithelium; and/or an annular glial mass overlying the scleral dehiscence, all of which have been observed histologically.25,26 Each of these findings could potentially demonstrate T1 hyperintensity and may therefore account for the observed signal intensity of this elevation in our study.3 Of note, imaging in 3 of our patients demonstrated fat within the distal optic nerve sheath, also consistent with previous histopathologic studies.25,26
MGDA has been reported to be associated with a broad range of cranial abnormalities. Ocular associations are particularly numerous and include retinal detachment, persistent hyperplastic primary vitreous, congenital cataract, nanophthalmos, eyelid hemangioma, drusen, and preretinal gliosis.2,8,21,27 Of these, we observed retinal detachment in 1 patient. Abnormal communication between the subretinal, subarachnoid, and vitreous spaces in MGDA may account for this frequent association.21,28 Abnormalities of the visual pathways have also been reported in MGDA, including atrophy/hypoplasia of the contralateral optic chiasm as well as optic nerve glioma.3,29 In our cohort, we observed each of these findings in 1 patient. The optic chiasm atrophy/hypoplasia in MGDA could result either from retrograde axonal degeneration in the setting of an intracranial lesion or from antegrade degeneration related to the ganglion cell deficit within the developing retina.8 The relationship between MGDA and optic nerve glioma remains largely unexplored.
MGDA is associated with intracranial vascular abnormalities, which range from static segmental aplasia of the circle of Willis to a progressive vasculopathy (Moyamoya disease), in up to 45% of patients. 5,9,11–13,22 Indeed, one of our patients demonstrated the characteristic findings of Moyamoya, including steno-occlusive changes of the anterior circulation and extensive lenticulostriate collateralization. The association of MGDA with vascular abnormalities has been proposed to reflect the fact that, during the fourth week of gestation, the internal carotid arteries develop in close relationship to the optic vesicles.30 However, the exact relationship between these 2 systems in patients with MGDA, particularly in the setting of a progressive disease such as Moyamoya disease, has yet to be elucidated. There has been at least 1 report suggesting that the coexistence of hemangioma, MGDA, and intracranial vascular abnormalities may reflect a manifestation of PHACES association.31
MGDA has also been associated with skull base abnormalities, including basal cephaloceles.1,13 It has been proposed that the incomplete fusion of the palates abrogates normal development of the optic nerves, potentially by drawing them into the defect.32 Although no cephaloceles were detected in our cohort, we observed in 1 patient a patent craniopharyngeal canal with herniation of the pituitary gland into its proximal aspect. The posterior pituitary bright spot was present, and the patient's endocrine function was intact. The absence of a consistent association in our study sheds doubt on a causal relationship between skull base abnormalities and development of the MGDA.
Conclusions
We have demonstrated several consistent orbital features of MGDA with MR imaging in the largest series to date. These findings may allow for accurate differentiation from other optic nerve and associated ocular anomalies and have the potential to guide appropriate management of this patient population, especially in situations where funduscopic examination is limited.
Footnotes
Disclosures: Caroline D. Robson—UNRELATED: Consultancy, Royalties: Amirsys, Comments: Content author and editor. Gena Heidary—UNRELATED: Grants/Grants Pending: Knights Templar Eye Foundation; Payment for Lectures (including service on speaker bureaus): I received honoraria from the Lancaster Course held at Colby College, where I teach a session on pediatric neuro-ophthalmology every year. I have been participating in the course for the past 3 years. I also, in 2011, taught a boards review course through the Osler Institute. The institute provided me with an honorarium for my time teaching the residents. Finally, I received an honorarium for speaking at St. Anne's Hospital on neuro-ophthalmic emergencies. Michael J. Paldino—UNRELATED: Grants/Grants Pending: Foundation of the American Society of Neuroradiology.* *Money paid to institution.
REFERENCES
- Received December 18, 2012.
- Accepted after revision January 23, 2013.
- © 2013 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}