
Abstract
BACKGROUND AND PURPOSE: As aneurysms arising from the ophthalmic segment of the internal carotid artery increase in size, they can compress the optic nerve, prompting patients to present with visual disturbances. The purpose of this article is to describe the clinical and angiographic results with an emphasis on visual outcomes following the endovascular treatment of ophthalmic segment ICA aneurysms.
MATERIALS AND METHODS: The records of 1254 patients who presented for endovascular treatment of a cerebral aneurysm were retrospectively reviewed to identify 65 consecutive patients who underwent coil embolization of an ophthalmic segment ICA aneurysm. The clinical records, treatment reports, and imaging were reviewed with a focus on visual outcomes.
RESULTS: Twenty-two of the 65 patients (34%) who presented for treatment of an ophthalmic aneurysm reported a visual disturbance at presentation. Fifteen of the 22 patients (68%) experienced an improvement in their symptoms after treatment. Overall, patients with visual symptoms were significantly more likely to benefit from treatment than to have a decline in vision (P = .03). The overall morbidity was 4%, and mortality was 0%. The retreatment rate was high at 30%, though this was disproportionately weighted by an 86% retreatment rate in patients with ruptured aneurysms.
CONCLUSIONS: Patients with visual symptoms attributable to ophthalmic segment ICA aneurysms undergoing endovascular coil embolization were statistically more likely to experience an improvement in their vision than to have worsening or unchanged vision. Coiling was associated with a low morbidity rate, though an elevated retreatment rate.
Aneurysms arising from the ophthalmic segment of the internal carotid artery account for approximately 5% of all intracranial aneurysms.1,2 As these aneurysms increase in size, they can compress the optic nerve, prompting the patient to present with visual disturbances, often involving the inferior and/or nasal fields first.2,3 Both surgical and endovascular treatment of these aneurysms have shown the potential to improve visual disturbances if occurring early.2,4⇓⇓⇓⇓⇓⇓–11 However, treatment of these aneurysms is not without its own set of inherent risks. Retinal artery occlusion or delayed optic ischemia may occur after either surgical or endovascular repair.12⇓–14 A review of recent surgical literature suggests a permanent morbidity ranging from 3% to 38% following treatment of an ophthalmic segment ICA aneurysm.3,5,6,10,15⇓⇓–18 This morbidity includes a risk of new or worsened visual disturbance in 2%–30% of surgically treated patients and 3%–8% of endovascularly treated patients.3,5,6,15,16
This article assesses the angiographic and clinical outcomes of 65 consecutive patients who presented for initial treatment of an ophthalmic segment ICA aneurysm via an endovascular approach. Our goal is to describe the clinical and angiographic outcomes with an emphasis on visual outcomes following the endovascular treatment of ophthalmic segment aneurysms.
Materials and Methods
Study Design
Under the auspices of the institutional review board, the records of 1254 patients who presented for treatment of a cerebral aneurysm between October 2001 and April 2009 were retrospectively reviewed. For the purposes of this article, only ophthalmic segment aneurysms arising from the dorsal internal carotid artery at or immediately adjacent to the origin of the ophthalmic artery were included, in keeping with the definition by Day.2 From our cohort, we identified 65 consecutive patients (5.2%) who presented for initial endovascular treatment of an ophthalmic segment aneurysm. Medical and radiographic records were independently reviewed by a member of the research team who did not participate in the treatment of any of the included patients. Demographics, details of treatments, effects of treatments, results of follow-up procedures, and complications were recorded.
Interventional Procedures
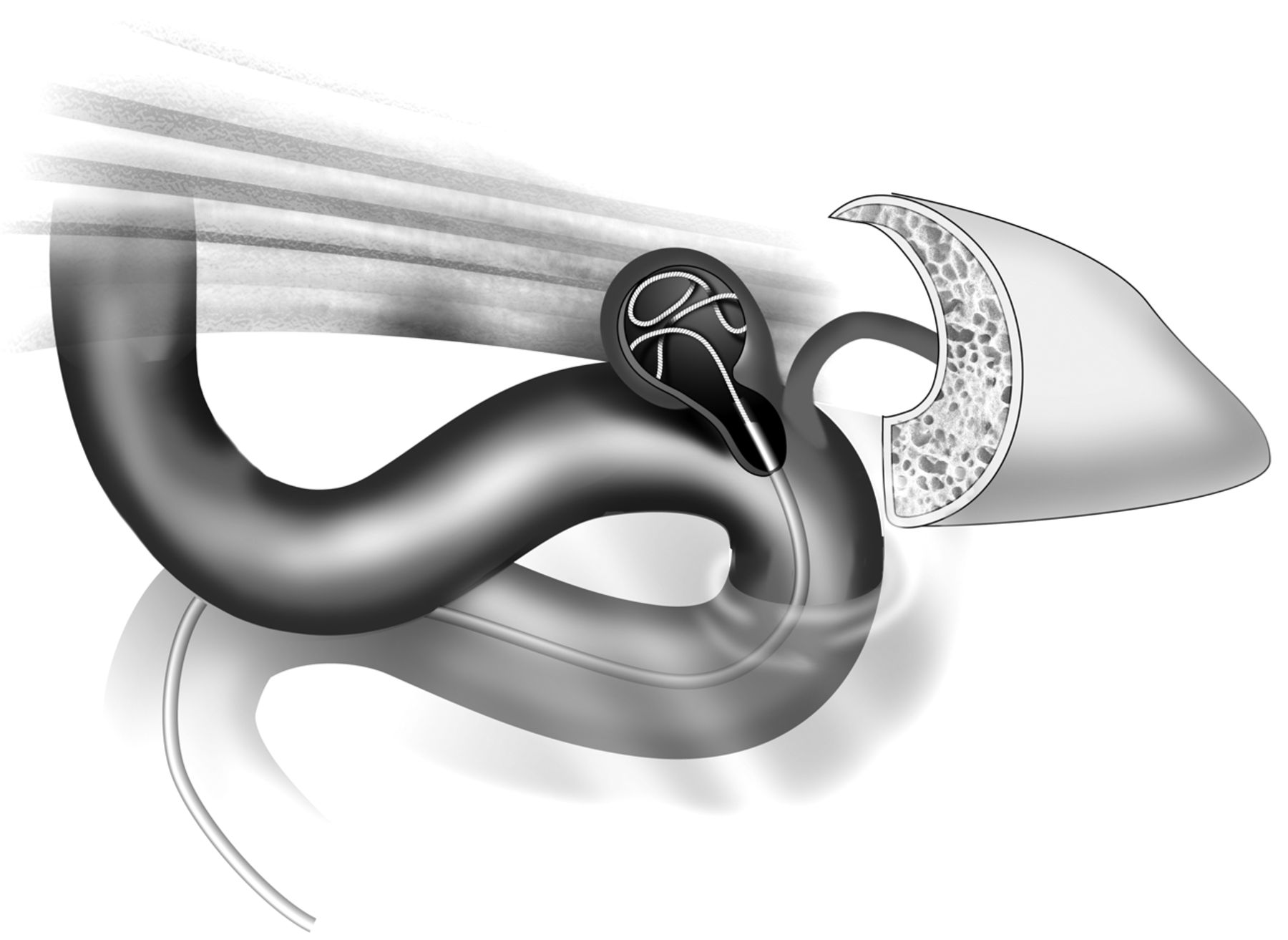
All procedures were performed under the care of 1 of 3 neurointerventional surgeons. Endovascular intervention was performed by using a biplane flat panel digital subtraction unit with the patient under general anesthesia. All patients were treated with a bolus of heparin at the beginning of the procedure to reach an activated clotting time of 250–300 seconds. In standard fashion, a guiding catheter was placed in the internal carotid artery, and diagnostic cerebral angiography was performed. Working projections were obtained, the aneurysm was measured, and under roadmap guidance, a microcatheter was placed into the aneurysm sac (Fig 1). Adjunct treatment measures, such as stent-assistance, dual-catheter technique, or balloon remodeling, were performed at the operator's discretion, as noted in the “Results” section. Immediate postprocedural DSA confirmed the occlusion status of the aneurysm and allowed evaluation of parent vessel patency and thromboembolic procedural complications.

Endovascular coil embolization of an ophthalmic segment aneurysm.
Imaging Assessment
Imaging outcomes were recorded for each case. Immediate treatment outcomes were documented in all cases via digital subtraction angiography in 2 planes. At discharge, patients were scheduled for 6- and 12-month angiographic follow-up with the intent to image via CTA, MRA, or additional DSA studies at 24 months. Long-term follow-up imaging analysis was limited to those patients with at least 12 months' follow-up. The follow-up imaging was evaluated for stability, recurrence, or progressive/delayed occlusion of the aneurysm. In cases of recurrent or residual aneurysms, the remnant was classified according to the Raymond classification scale.19
Clinical Assessment
Through a review of the medical records, the clinical presentation and outcomes were recorded for each patient. Complete neurologic examinations were available for each patient. Visual assessment was performed by a neuro-ophthalmologist, neurologist, neurosurgeon, or neurointerventional surgeon. In patients with visual disturbances believed likely to be related to their ophthalmic segment ICA aneurysms, the preprocedural visual disturbance was recorded and compared with their postprocedural evaluation to assess stability, improvement, or deterioration. Major complications were classified as any hemorrhage, clinically significant infarction, or dissection that was directly related to the procedure, as determined by consensus between the neurointerventionalist and the neurosurgeon or neurologist who provided concurrent care to the patient.
Statistical Analysis
Data are presented as mean and range for continuous variables and as frequency for categoric variables. Statistical analyses of categoric variables were performed by using the χ2 and Fisher exact tests and the Mantel-Haenszel test for linear association, and comparison of means was performed by using the Student t test and Wilcoxon rank sum test as appropriate. Univariate analysis was used to test covariates predictive of the following dependent variables: treatment-related complications, retreatment, and unfavorable visual outcome (decreased visual function or increased visual pain). Additionally, stable or worse visual outcome was defined as those patients with increased visual pain or decreased neurologic function or no improvement in baseline visual pain or neurologic dysfunction. Only 1 patient had improvement in visual dysfunction but increased visual pain and was categorized as an unfavorable visual outcome. No patients had decreased visual pain but decreased visual function. Interaction and confounding were assessed through stratification and relevant expansion covariates. Independent factors predictive of the 5 dependent variables in univariate analysis (P < .20) were entered into 5 separate multivariate logistic regression analyses. P values ≤ .05 were considered statistically significant.20 Statistical analysis was performed with STATA 10.0 (StataCorp, College Station, Texas).
Results
Patient Demographics and Aneurysm Characteristics
Of the 65 patients included in this study, 57 (87.7%) were women (Table 1). The average age was 56 years. Twenty-two of the 65 patients presented with a visual disturbance (Table 2). Eleven patients presented after rupture of the aneurysm. Almost half of the patients were hypertensive (n = 31).
Patient demographics and aneurysm characteristics with breakdown of the characteristics according to the presence/absence of a visual disturbance at presentation
Visual disturbances prompting 22 patients to present for evaluationa
The average diameter of the aneurysms was 8.4 mm, with the difference between ruptured aneurysm diameter (10.6 mm) and unruptured aneurysm diameter (7.9 mm) approaching significance (P = .086). Aneurysms causing a visual disturbance (9.1 mm) tended to be larger than those that did not (8.1 mm), though this was not statistically significant (P = .18).
Most patients (n = 52, 80%) were treated by coil embolization alone. Four patients (6%) were treated by using balloon assistance. Nine (14%) underwent stent-assisted coil embolization.
Visual Outcomes
Twenty-two of the 53 patients (42%) who presented for elective treatment of an unruptured ophthalmic segment ICA aneurysm were found to have a visual disturbance at presentation. A change in visual acuity was the most common symptom (Table 1). Seven of the 22 patients (32%) were evaluated by an ophthalmologist. The average magnification requirement for patients seen by an ophthalmologist was 10.6 ± 6.1. Four of the 7 patients (57%) had a visual field deficit, 2 with a central deficit, 1 with a nasal field deficit, and 1 with a left superior homonymous deficit. Three of the 7 patients (43%) had evidence of optic nerve atrophy. Patients with visual disturbances were more likely to have a larger aneurysm diameter, though this was not statistically significant (Table 1).
Following treatment, patients in this study were much more likely to have an improvement in their visual symptoms than to develop a new or worsening visual disturbance (P = .03). Fifteen of the 22 patients (68%) experienced an improvement in their ophthalmologic examinations as measured by a combination of confrontational testing and a Snellen chart. Five patients (23%) had no change in their visual symptoms. Three of these 5 patients (60%) had documented optic nerve atrophy on their ophthalmologic examination. Two patients (9%) experienced a decline in their visual acuity. One patient (2%) developed a new decline in visual acuity after treatment.
Patients whose visual disturbance improved following endovascular coiling of their ophthalmic segment aneurysm tended to have smaller aneurysms with a smaller neck than those who remained stable or whose vision deteriorated (Table 3).
Aneurysm characteristics among patients who either presented with a visual disturbance or developed one after treatmenta
Complications
Sixteen patients required ≥1 retreatment, resulting in 91 total treatments of the 65 unique aneurysms (Table 4). The overall morbidity from the 91 treatments was 4% (4 cases). There were no deaths. Three of the complications occurred in the 81 treatments of unruptured aneurysms (3%). In 1 of these cases, the patient developed hydrocephalus despite the lack of hemorrhage, requiring a shunt. Two patients presented with an acute infarction >7 days after treatment. Of the 12 treatments of ruptured aneurysms, there was 1 complication (8%). In this case, the patient experienced a postprocedural infarction due to hypoperfusion.
Clinical and imaging outcomes according to the presence/absence of a subarachnoid hemorrhage at presentation
Univariate predictors of treatment-related complications (P < .20) included the presence of subarachnoid hemorrhage (P = .105), no visual disturbance on presentation (P = .102), a history of hypertension (P = .037), packing attenuation of <22% (P = .158), the presence of a stent (P = .171), the use of clopidogrel (0.146), and the presence of residual filling of the aneurysm at the end of the procedure (P = .049). A multivariate analysis showed that patients with ruptured aneurysms were 5.8 times more likely to experience a major complication (95% CI, 1.02–33.03; P = .047). In addition, those patients with hypertension were 5.2 time more likely to experience a complication (95% CI, 1.08–24.93; P = .039).
Imaging Outcomes
Of the 65 aneurysms, 35 (55%) were completely occluded at the end of the procedure. Thirty of the 53 unruptured aneurysms (58%) and 5 of the 12 (42%) ruptured aneurysms were completely occluded at the end of the case (Table 4). At 12 months' follow-up, 2 of the 26 (8%) patients who had some residual filling at the end of the procedure demonstrated delayed occlusion of the aneurysm.
Long-term outcomes (≥12 months) were available for 53 (82%) patients. Overall, 16 (30%) of the patients with at least 12 months' follow-up required retreatment, including 10 of 46 (22%) patients treated electively and 6 of 7 (86%) patients treated after a subarachnoid hemorrhage. Univariate predictors of retreatment (P < .20) included ruptured aneurysm (P = .002), increasing Hunt and Hess scale score (P = .013), family history of aneurysms (P = .144), aneurysms on the left (P =.039), increasing maximum aneurysm diameter (P < .001), increasing maximum neck diameter (P = .008), increasing neck-to-dome ratio (P = .090), decreasing packing attenuation (P = .034), and packing attenuation of <22% (P = .003). The multivariate analysis demonstrated that those with a ruptured aneurysm were 44.2 times more likely to have a recurrence (95% CI, 3.80–514.04; P = .002). In addition, the diameter of the aneurysm was predictive of recurrence (OR = 1.36; 95% CI, 1.10–1.69; P = .005). In particular, aneurysms of >10 mm were at greater risk of recurrence (OR = 12.64; 95% CI, 2.05–78.06; P = .022). Finally, aneurysms with a packing attenuation of ≥22% were 84% less likely to recur (OR = 0.16; 95% CI, 0.03–0.96; P = .045).
Discussion
Patients who present with a visual disturbance attributable to an ophthalmic segment ICA aneurysm can expect further deterioration of their vision if the aneurysm is left untreated.7,21 Once treated, either endovascularly or surgically, a patient's vision would be expected to improve. Suction decompression during surgery relieves the direct mass effect of the aneurysm on the optic apparatus. The means by which endovascular treatment improves visual outcomes is not well-understood. One possibility is that thrombosis after coil embolization may relieve the pulsatile pressure on the optic nerve.22 A review of prior literature suggests that 49% of patients treated endovascularly3⇓⇓–6,12,23 and 63% of patients treated surgically2,5,8⇓⇓–11,23⇓–25 could be expected to experience improvement in their visual symptoms (Tables 5 and 6). Treatment, of course, is not without risk. If one looked broadly at the literature and combined data that included ruptured and unruptured ophthalmic segment ICA aneurysms, approximately 6% of patients treated endovascularly3⇓–5,15,16,18,23 and 9% of patients treated surgically2,3,5,6,9⇓–11,15,17,18,23⇓–25 may develop a new visual disturbance or experience worsening of their visual symptoms. In our series, 68% of patients treated endovascularly experienced an improvement in their visual symptoms. Two of 53 (4%) patients treated electively and 1 of 12 (8%) treated after a rupture developed a new or worse visual disturbance. Of note, 2 of the 3 patients who developed a new or worse visual disturbance were found to have a recurrence of their aneurysm, which may have contributed to their worsening symptoms.14 This information can help neurointerventional surgeons better inform patients about the risks and benefits of the endovascular treatment of ophthalmic segment aneurysms.
Visual outcomes after endovascular treatment of aneurysms affecting the visual pathway
Visual outcomes after surgical treatment of aneurysms affecting the visual pathway
A potential benefit in treating ophthalmic segment ICA aneurysms via endovascular coil embolization is a relative reduction in overall morbidity compared with open surgery. Three of 79 elective treatments (4%) in this study resulted in permanent morbidity. Two of the patients experienced an infarction, 1 of which was clearly related to the procedure and the other most likely not because emboli were found in multiple vascular territories. The third patient developed hydrocephalus after treatment. Overall, the 4% rate of complications reported here is within the range of 0.8%–18%, with an average of 4% reported for 691 endovascularly treated ophthalmic segment ICA aneurysms in the literature.3⇓⇓⇓–7,15,16,18,19,23,25⇓⇓–28 This complication rate is considerably less than those reported for the open treatment of ophthalmic segment aneurysms. Even with the development of microsurgical techniques, the reported morbidity in the literature during the past 5 years ranged from 9% to 39%, with an average of 21% for 381 patients.3,6,10,17,18,23,29 Although this study does not directly compare endovascular and open surgical techniques, the studies that have made this comparison have demonstrated an endovascular complication rate ranging from 0% to 18%, with an average of 4.5% for 358 aneurysms, while the surgical complication rate ranged from 3.7% to 27.5% with an average of 11.2% for 402 aneurysms.3,5,15,16
Of the 65 unruptured aneurysms, 55% were occluded primarily. This finding is similar to the 47% primary occlusion rate of 523 cumulative aneurysms treated endovascularly reported in the literature.3⇓⇓–6,25⇓–27,28 In the 30 patients who presented for at least 12 months of follow-up, 2 aneurysms (7%) that were not completely occluded at initial coiling progressed to complete occlusion at their follow-up examinations. The appearance of 64% of the aneurysms at follow-up was unchanged.
Overall, 30% of the aneurysms reported in this study required retreatment. This retreatment rate is skewed by the 86% retreatment rate in ruptured aneurysms compared with the 22% retreatment rate in unruptured aneurysms (P = .002). At our institution, our intent when treating ruptured aneurysms is to first protect the dome and any suspicious components of the aneurysm that may represent a point of rupture, such as a bleb or pseudoaneurysm. A broad review of the literature suggests a 20% recurrence rate with a range of 9%–53% in 503 aneurysms.3⇓⇓–6,18,25⇓–27,28 As expected, the retreatment rate after open clipping is significantly less than that after endovascular coil embolization. In a direct comparison of endovascular and open treatment of ophthalmic segment aneurysms, Sherif et al18 and Yadla et al6 reported a combined 4% retreatment rate after open clipping.
This study is limited by the retrospective nature and all of the biases imparted therein. Formal neuro-ophthalmologic evaluation was not available for all patients. In each of these cases, a visual assessment was available from a neurologist, neurosurgeon, or the interventional neuroradiologist. In cases of opposition testing, small defects may have been missed by either the patient or the physician. Given the retrospective nature of the study, the quality of the data is dependent on the clinical skill and reporting practices of multiple physicians. Thus, interpretation of improvement or worsening in visual symptoms at follow-up in patients not seen by an ophthalmologist is essentially subjective and dependent on the thoroughness of the documentation.
Conclusions
Patients with visual symptoms attributable to ophthalmic segment ICA aneurysms having undergone endovascular coil embolization were statistically more likely to experience an improvement in their vision than to have worsening or unchanged vision. Coiling was associated with a low morbidity rate (4%). However, the retreatment rate following coiling was elevated (30%).
Footnotes
Disclosures: John Gaughen—UNRELATED: Consultancy: Covidien, MicroVention, Stryker. Mary E. Jensen—UNRELATED: Payment for Lectures (including service on Speakers Bureaus): Speakers Bureau for Stryker Neurovascular; training lectures for Covidien. Avery J. Evans—UNRELATED: Consultancy: Stryker, Covidien, Grants/Grants Pending: Stryker, Patents (planned, pending or issued): US Patent Office, Mod Med Inc, Royalties: Cook, CareFusion.
This work was funded in its entirety by the University of Virginia Department of Radiology.
Paper previously presented at: Annual Meeting of the American Society of Neuroradiology, May 18–23, 2013; San Diego, California.
References
- Received February 19, 2014.
- Accepted after revision April 28, 2014.
- © 2014 by American Journal of Neuroradiology





{kind=link}