
Abstract
BACKGROUND AND PURPOSE: Dermatofibrosarcoma protuberans is a rare, locally aggressive sarcoma of the skin in children and adults, usually involving the trunk and extremities and less commonly the head and neck. Despite clinical reports in the literature on the management of dermatofibrosarcoma protuberans, there are limited articles describing its imaging features.
MATERIALS AND METHODS: We retrospectively reviewed the demographics and imaging findings in all 24 patients with pathologically proven dermatofibrosarcoma protuberans of the head and neck seen at a tertiary cancer center between 2001 and 2010.
RESULTS: Twenty-two of the 24 lesions were nodular and well circumscribed; 19 of the 24 were located on the scalp. On imaging, all 24 lesions involved subcutaneous tissues. The lesions ranged in size from 0.6–9.5 cm (mean, 3.7 cm; standard deviation, 2.3 cm). Twelve lesions involved the soft tissues either at or extending directly to the midline. Thirteen lesions were associated with bulging of the skin surface. Fourteen lesions were imaged with CT and 14 with MR imaging. Whereas variable enhancement patterns were noted on CT and MR imaging, dermatofibrosarcoma protuberans was usually T2-hyperintense and demonstrated marked enhancement. None of the lesions was associated with bone invasion, perineural spread, or nodal/distant metastasis.
CONCLUSIONS: Knowledge of the imaging characteristics of dermatofibrosarcoma protuberans may alert neuroradiologists to include dermatofibrosarcoma protuberans in the differential diagnosis of lesions about the head and neck with similar imaging characteristics.
ABBREVIATIONS:
- DFSP
- dermatofibrosarcoma protuberans
- PDGFB
- platelet-derived growth factor β-chain
- PDGF-R
- platelet-derived growth factor receptor tyrosine kinase
Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive sarcoma of the dermis with a high cure rate.1,2 DFSP often presents in the third or fourth decade of life, most commonly involving the trunk (50–60%) or proximal extremities (20–30%) and less commonly involving the head and neck (10–15%).3,4 DFSP grows in an infiltrative manner and has the capacity for local recurrence, though it rarely metastasizes.5,6
The imaging features of DFSP of the trunk and extremities are nonspecific, including low signal on T1 and high on T2 on MR imaging, with uniform enhancement after contrast administration.7,8 CT findings include isoattenuated to hypoattenuated lesions without calcifications and uniform (small lesions) to heterogeneous (large lesions) enhancement after contrast administration.9 Previously published reports on DFSP have highlighted its clinical features, but only a few small series have outlined its imaging features.7,8,10 The purpose of this study was to more comprehensively define the CT and MR imaging appearance of DFSP of the head and neck.
Materials and Methods
This study was approved by the Institutional Review Board of The University of Texas MD Anderson Cancer Center, which waived the requirement for informed consent. We retrospectively reviewed the demographics and radiologic images of 24 patients with pathologically proven DFSP of the head and neck seen at our institution between 2001–2010.
Fourteen patients underwent CT of the head and neck, and 14 patients underwent MR imaging of the head and neck. The CT examinations were performed after intravenous administration of contrast material. Soft tissue and bone windows were evaluated in all patients. MR imaging sequences included axial T1 precontrast, orthogonal T1 postcontrast, and T2-weighted sequences (Table).
Patient demographics and image appearance
The following imaging features were documented: lesion size, location, enhancement pattern, calcification, and perineural spread; associated osseous abnormality; and presence of nodal or distant metastasis.
Results
Clinical Features
The patients ranged in age from 15–72 years (mean, 42.5 years; median, 40 years) and included 12 women and 12 men. Seventeen patients presented with a primary, untreated tumor, and 7 patients presented with recurrent disease. The most common presenting symptom was a slowly enlarging mass (n = 18). Six patients described a history of trauma before development of a slowly growing mass at the same site as the trauma. The trauma occurred 2 years before presentation in 2 patients, 6–11 years before presentation in 3 patients, and as a child in 1 patient. DFSP was diagnosed through biopsy in all 24 patients.
Imaging Findings
On imaging, 19 lesions involved the scalp; other locations included the posterior neck (n = 1), left face to midline (n = 1), pre-auricular region (n = 1), chin (n = 1), and cheek (n = 1). All 24 lesions involved the subcutaneous soft tissues. Eighteen lesions extended up to the skin surface, and, of these, 13 were associated with bulging of the skin, 2 were associated with an exophytic fungating component, and 2 were associated with skin retraction; 1 was associated with none of these findings. Twelve of the lesions involved the soft tissues either at (n = 6) or near the midline (n = 6). The lesions ranged in size from 0.6–9.5 cm (mean, 3.7 cm; standard deviation, 2.3 cm). Twenty-two of the 24 lesions were nodular and well-circumscribed; the nodules were singular in 13 cases, coalescent in 6 cases, and multiple but separated in 3 cases. Two lesions had an infiltrative pattern; both manifested as recurrences in the operative field. None of the patients had evidence of osseous destruction, cervical lymph node, or distant metastasis.
CT Findings
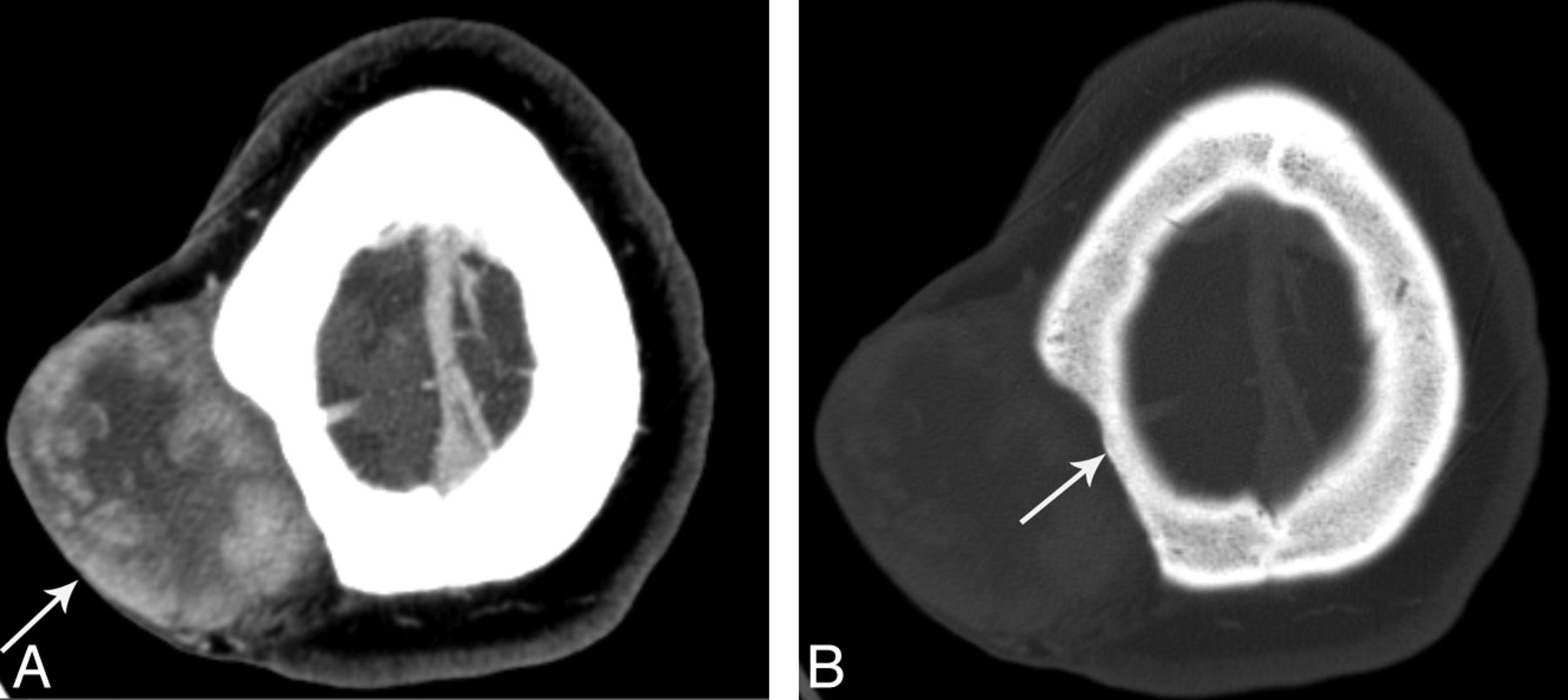
The 14 lesions imaged with CT demonstrated enhancement that was either minimal (n = 3), heterogeneous (n = 3) (Fig 1A), or homogeneous (n = 8). There was no evidence of calcification, and none of the lesions demonstrated CT evidence of perineural spread. Osseous destruction was absent; however, thinning of the underlying calvaria (Fig 1B) was seen in 2 patients (patients 10 and 16).

A 31-year-old woman (patient 10) with DFSP of the right parietal scalp. Contrast-enhanced axial CT in soft tissue (A) and bone window (B) shows a 6.1 × 4.8-cm heterogeneously enhancing mass (A, arrow) that bulges the skin surface outward and thins underlying calvaria (B, arrow).
MR Imaging Findings
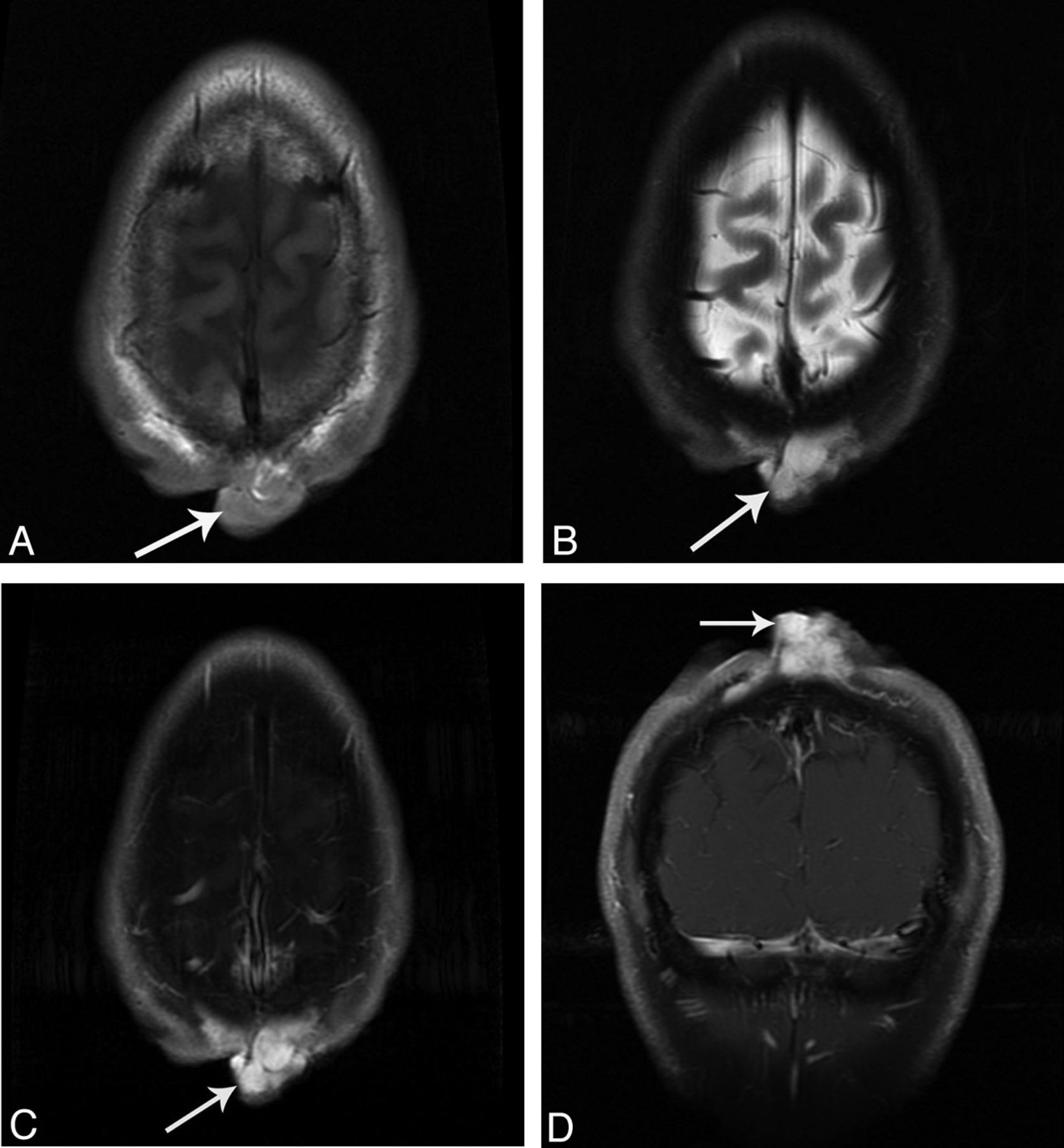
All 14 lesions imaged with MR were T1-isointense to muscle (Fig 2A); 10 lesions were T2-hyperintense (Fig 2B) and 4 were iso-intense to hypointense to muscle. T1 postcontrast enhancement patterns ranged from mild (n = 1) to markedly heterogeneous (n = 4) or markedly homogeneous (n = 9) (Fig 2C,-D). Neither perineural spread nor bone involvement was present in any case.

A 31-year-old man (patient 1) with DFSP of the parietal midline scalp. MR imaging shows a 3.5 × 1.8-cm T1-isointense, T2-hyperintense, coalescing nodular mass with marked homogeneous enhancement in the parietal midline scalp (arrows). A, Axial noncontrast T1. B, Fast spin-echo T2 with fat saturation. C, T1 postcontrast axial with fat saturation. D, T1 postcontrast coronal with fat saturation.
Pathologic Findings
Most the lesions were found in the lower dermis and the subcutaneous tissue. All tumors manifested spindle cell proliferation arranged in light storiform patterns. Although infiltrative with ill-defined boundaries, the cells were bland and lacking mitotic activity and nuclear pleomorphism.
Seven patients presented to our institution with recurrent disease after having undergone resection at other centers. In 6 of the 7 patients, the pathologic specimens from the initial resection were submitted and reviewed by our pathology department. In all 6 patients, DFSP was present at the surgical margins.
Treatment
The lesions were treated with surgical excision (n = 9), excision and radiation (n = 8), excision and chemotherapy (n = 3), chemotherapy (n = 3), or all 3 treatments (n = 1). All of the patients were still alive at the time of this report.
Discussion
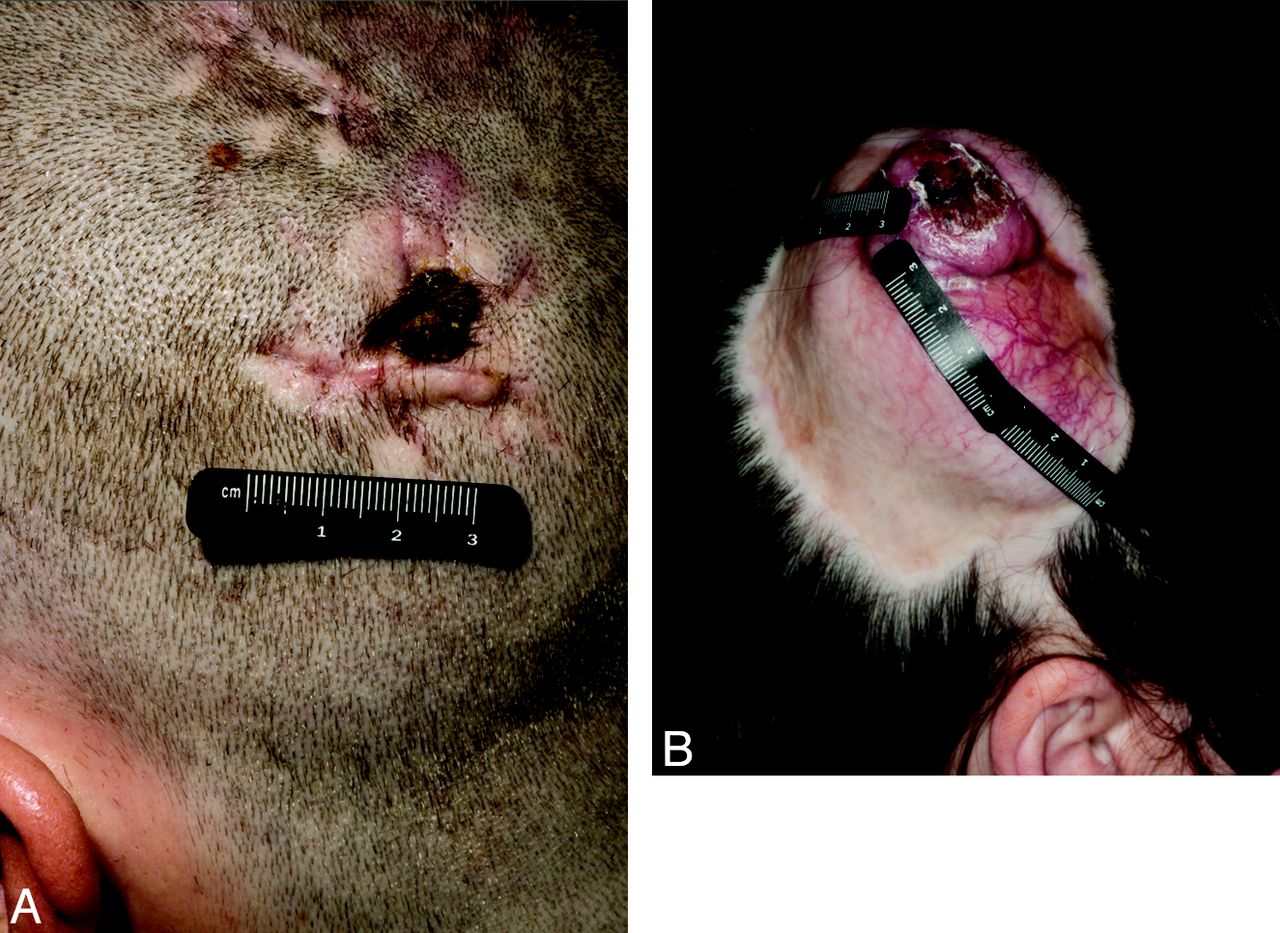
DFSP typically presents as a slow-growing, painless, and firm subcutaneous nodule.11 The lesions can be multiple and may coalesce to form an indurated plaque (Fig 3), which on clinical examination is often violaceous.12,13 The growth rate is variable; some lesions remain stable in size for many years, whereas others demonstrate slow progressive growth.14 DFSP can arise in healthy skin or in areas of repeated trauma, vaccination sites, irradiated skin, or scars.15 Six patients in our series had a history of local trauma before the development of DFSP, and the interval between the trauma and development of DFSP varied. Tattoo sites also show a predilection for benign and malignant changes and should be evaluated during regular skin examinations; DFSP should be considered in the differential diagnosis of neoplasms arising within areas of tattoos.16

Photographs of 2 patients with DFSP. A, Patient 16, a 25-year-old man with a large DFSP of the scalp extending from the midline near the vertex down to the left lower parietal region with subcutaneous infiltration. B, Patient 10, a 31-year-old woman with a large DFSP of the right paramedian posterior parietal scalp.
In our series, DFSP lesions ranged in size from 0.6–9.5 cm, and half were located at or extended to the midline. Variable enhancement was noted on CT (Fig 1A), similar to prior reports.8,9 On MR imaging, almost all of the cases showed marked enhancement (Fig 2C,-D), which has not previously been reported.7,8 None of the lesions was associated with perineural spread, nodal, or distant metastases. No osseous destruction was demonstrated; however, calvarial thinning was seen in 2 patients. These 2 patients (patients 10 and 16) had the largest lesions, which suggests that the thinning could be related to a pressure effect. Although none of the lesions in our series showed intracranial extension, this has been described in 2 case reports.10,17
None of the patients in our series had local or nodal metastasis, perineural spread, or bone destruction. In contrast, 2–3% of all patients with squamous cell carcinoma of the skin have metastasis, which occurs almost exclusively through lymphatic channels and only rarely through hematogenous spread.18 Perineural spread occurs in basal cell carcinoma, squamous cell carcinoma, and melanoma (desmoplastic), usually involving cranial nerves V and VII.19,20
Bony destruction is uncommon with skin tumors, but when bone destruction is noted on imaging, malignant melanoma and squamous cell carcinoma should be considered.21⇓–23
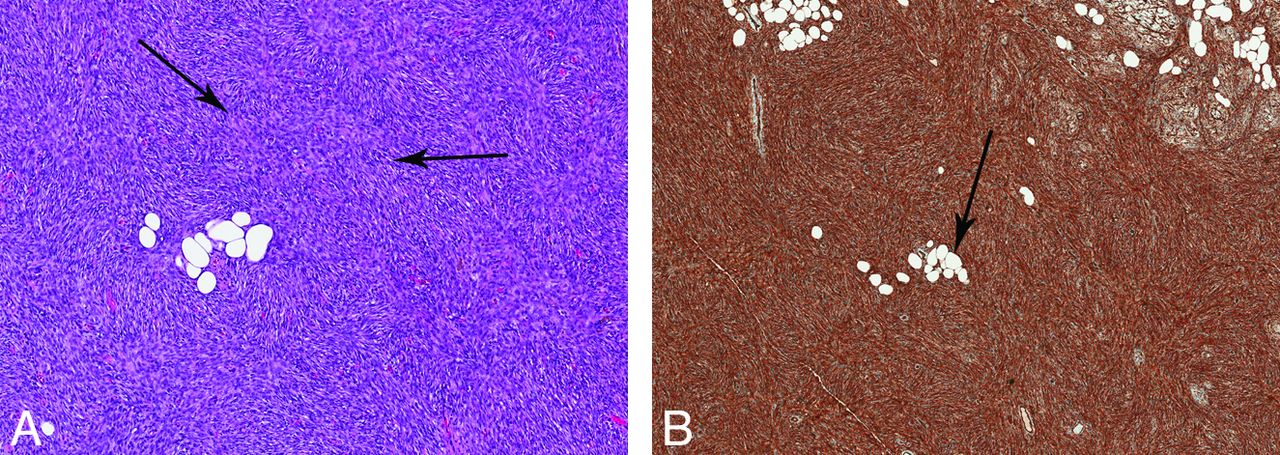
Histologically, DFSP is an infiltrative soft tissue neoplasm of the dermis and subcutaneous tissues. DFSP is composed of bland, elongated spindle cells with a storiform, or whorled, pattern arranged around foci of collagen or vascular spaces, radiating outward like the spokes of a wheel (Fig 4A).24 Infiltration around fat cells may produce a honeycomb appearance of the fat (Fig 4B).25 Immunohistochemical analysis may assist if the diagnosis as DFSP is positive for CD34 staining (Fig 4B), with a reported sensitivity of 84–100%.26⇓–28 Because other skin lesions are also positive for CD34 staining, CD34 is not specific for DFSP; however, CD34 positivity in combination with the histologic features makes the diagnosis.

Pathologic specimen of DFSP. A, Hematoxylin and eosin stain. Elongated spindle cells with a storiform (whorled) pattern arranged around foci of collagen or vascular spaces, radiating outward (arrows). B, CD34 stain. The specimen is positive for CD34 staining. Fat entrapment is noted with a honeycomb pattern (arrow).
At the genetic level, the critical initiating event in DFSP development is rearrangement of chromosomes 17 and 22 in the form of a supernumerary ring chromosome [r (17; 22)] or a reciprocal translocation [t (17; 22)]. Either of these rearrangements results in chimeric fusion of the genes encoding the platelet-derived growth factor β-chain (PDGFB) and the collagen type 1 α1-chain, which in turn results in autocrine activation of the platelet-derived growth factor receptor tyrosine kinase (PDGF-R), which triggers the proliferation of DFSP tumor cells.29,30
Treatment options include complete surgical excision, including wide excision and Mohs micrographic surgery, radiation, and imatinib mesylate.2,11,31 Imatinib, a competitive tyrosine kinase inhibitor, is currently approved by the Food and Drug Administration for the treatment of adult patients with unresectable, recurrent, and/or metastatic DFSP, and this may in turn facilitate tumor resection and or decrease disfigurement.32 After local resection, the 5-year survival rate is 93–100%.33,34 In agreement with these previously reported findings, none of the patients in our series had died of disease at the time of this report. Local recurrence occurs in 20–55% of cases.12⇓–14,35 Most local recurrences occur within 3 years11,12,35; only 30% occur after 5 years.32 The lungs are the most common site of distant metastasis,12,30,36,37 and metastasis has been reported to occur in 5–6% of cases.13,14,34,35,38,39
Differential diagnoses of other cutaneous neoplasms that could be confused with DFSP include dermatofibroma, epidermal cyst, peripheral nerve sheath tumor, nodular fasciitis, cavernous hemangioma, liposarcoma, nodular type of melanoma, and mycosis fungoides.21,40,41 Dermatofibroma can have imaging findings similar to DFSP on CT and MR imaging but is most frequently seen in the extremities, whereas DFSP is most commonly seen in the trunk.42,43 Epidermal cyst, most commonly an incidental finding, does not enhance on both CT and MR, unless infected, whereas DFSP shows variable enhancement on CT and MR imaging.44,45 Peripheral nerve sheath tumors are usually close to a major nerve, with certain signs such as split fat or fascicular or target sign, which are absent in DFSP.45,46 Plexiform neurofibromas tend to be asymmetric and diffuse, whereas DFSP most commonly is nodular.47,48 Clinically, patients with plexiform neurofibromas have neurofibromatosis type 1. Nodular fasciitis can be indistinguishable from DFSP by imaging. However, on MRI, one may see fascial tail sign, which is the linear extension of the lesion along the fascia, which also may appear to be enhanced. Nodular fasciitis favors the upper extremity, whereas DFSP favors the trunk.40,41,49 Cavernous hemangioma has low attenuation on CT, and calcifications are common, features not seen in DFSP.49,50 Liposarcoma contains fat, which is not present on DFSP.45 The nodular type of melanoma is mostly clinically blue to black, and DFSP is often violaceous. Melanotic melanoma is hyperintense on T1-weighted images and hypointense on T2-weighted images. Melanomas can have associated lymphadenopathy and osseous destruction not usually found in DFSP.44,51,52 Mycosis fungoides is the most common type of cutaneous T-cell lymphoma. CT findings include skin thickening, edema, soft tissue infiltration, lymphadenopathy, and systemic manifestations, not typically found in DFSP.45,53 The imaging findings of DFSP are nonspecific, but the combination of imaging findings, location of the lesion, and clinical features of the lesion help narrow the differential diagnosis of these cutaneous lesions mimicking DFSP.
Limitations of the study include the retrospective nature of the review. Similar imaging studies were not available for each patient, and, for the 7 patients presenting to our center with recurrent disease, the initial imaging of the primary lesion was not submitted for interpretation. However, the pathologic specimens for 6 of the 7 patients with recurrent DFSP were reviewed by our pathology department. DFSP was present at the surgical margins in all 6 specimens, which suggests that recurrent disease may be associated with incomplete surgical resection. This is in keeping with published reports of high recurrence rates in patients with positive surgical margins.54 The most significant prognostic factor in patients with DFSP has been the extent of surgical resection.2
Conclusions
DFSP of the head and neck region typically involves the dermis of the scalp, is often well-circumscribed with a nodular appearance, presents as a subcutaneous mass of variable size, often occurs near the midline, and is associated with bulging of the skin surface. Variable enhancement patterns are noted on CT, but, on MR imaging, DFSP is usually T2-hyperintense with marked enhancement. There is a high propensity for local recurrence but a low incidence of bone invasion, perineural spread, and nodal or distant metastasis. Neuroradiologists should be familiar with the imaging appearance of DFSP and include DFSP in the differential diagnosis of head and neck dermal tumors with similar imaging characteristics.
Acknowledgments
We wish to thank Stephanie Deming for editorial assistance.
Footnotes
Disclosures: Adel K. El-Naggar—UNRELATED: Grants/Grants Pending: NIH,* NCI,* NIDCR*; Other: Salivary Gland Tissue Biorepository,* Comments: Contract with NIH to collect extremely rare cancers of the head and neck and distribute to researchers conducting relevant research (*money paid to institution).
Paper previously presented as a poster at: Annual Meeting of the American Society of Head and Neck Radiology, October 3–7, 2012; Miami Beach, Florida.
The University of Texas MD Anderson Cancer Center is supported in part by the National Institutes of Health through Cancer Center Support Grant CA016672.
References
- Received February 10, 2013.
- Accepted after revision April 19, 2013.
- © 2014 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.