
Abstract
BACKGROUND AND PURPOSE: Long-term follow-up data of coiled basilar tip aneurysms are scarce, and little is known about the risk of late aneurysm-related adverse events. We followed a cohort of 154 patients with basilar tip aneurysms coiled between 1995 and 2006.
MATERIALS AND METHODS: Imaging and clinical data were retrospectively reviewed. The incidence and timing of retreatment, rebleeds, and progressive mass effect by continuous aneurysm growth were recorded. Risk factors for retreatment were assessed.
RESULTS: Clinical follow-up of 144 of 154 patients who survived the admission period was a mean of 9.8 years (median, 10.2; range, 0.3–20.1 years). During this period, 37 basilar tip aneurysms (26%) were additionally coiled (annual incidence rate, 2.6%; 95% CI, 1.8%–3.6%). Aneurysm size of >15 mm was the most important independent predictor for retreatment (OR, 8.7; 95% CI, 3.4–22.5). The first additional coiling was performed in the first year of follow-up in 17 of 37 patients (46%) and in 20 patients (54%) at a later time up to 17.2 years. Nine rebleeds occurred in 9 of 106 patients who initially presented with SAH after a median follow-up of 8.3 years (range, 0.3–16.6 years). The annual incidence rate was 0.7% (95% CI, 0.4%–1.5%). Eight patients died of aneurysm-related adverse events: 3 of rebleed and 5 of progressive mass effect.
CONCLUSIONS: Retreatment of coiled basilar tip aneurysms was frequently needed during follow-up, also at long intervals. Most late mortality was from progressive mass effect, not from rebleeds. Life-long MRA follow-up at yearly intervals is recommended.
Approximately 20% of coiled of intracranial aneurysms show reopening at follow-up, of which half are retreated.1 Risk factors for reopening with time are large aneurysm size, a wide neck, the presence of intraluminal thrombus, low packing attenuation, initial incomplete occlusion, duration of follow-up, and location in the posterior circulation.2⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–17 In general, additional coiling is advocated in reopened aneurysms to prevent rebleeding. Most reopenings occur in the first year after coiling and become apparent at the first imaging follow-up after 6–12 months. A first time reopening beyond the 12-month follow-up is infrequent.6,7,9,10,12,13
Aneurysms at the basilar tip form a special subset of intracranial aneurysms. First, surgery is a less likely option in these aneurysms, and even aneurysms with unfavorable configuration are coiled, whereas unfavorable aneurysms in the anterior circulation can be clipped. Basilar tip aneurysms are located on a vascular bifurcation and often have a wide neck. Therefore, reopening in basilar tip aneurysms is more frequent than in aneurysms at other locations.1,2,10,13,16,17 Second, some coiled basilar tip aneurysms show continuous growth with progressive mass effect on the brain stem.17
We followed a cohort of 154 patients with basilar tip aneurysms coiled between 1995 and 2006 for up to 20 years, to assess survival, frequency and timing of reopening, and retreatment. In addition, clinical events from the basilar tip aneurysm, such as rebleeds and progressive mass effect by continuous growth, were recorded.
Materials and Methods
We retrospectively followed a cohort of 154 consecutive patients with basilar tip aneurysms coiled between January 1995 and August 2006. Details on the follow-up of a mean of 4.4 years of this patient cohort have been published previously.18 We extended the clinical and MR angiographic follow-up time to obtain long-term clinical data and assess possible risk factors for late basilar tip aneurysm–related adverse events.
Study Population
The cohort of 154 patients with coiled basilar tip aneurysms included 42 men (27%) and 112 (73%) women, with a mean age of 50.5 years at the time of coiling (median, 50 years; range, 25–73 years). There were 114 ruptured (74%) and 40 unruptured aneurysms (26%). The mean aneurysm size was 11.1 mm (median, 10 mm; range, 2–30 mm). There were 83 small aneurysms (<10 mm), 61 large aneurysms (11–24 mm), and 10 giant aneurysms (>25 mm). Demographics during follow-up of patients who survived the hospital admission period included sex, age, rupture status of the aneurysm, occlusion after coiling, use of supporting devices during coiling, procedural complications, and clinical and imaging outcomes. Additional coiling and its complications and timing during the years were documented. After we encountered several unexpected late adverse events in a short period in patients with coiled basilar tip aneurysms in 2012, we adapted our follow-up protocol and actively attempted to extend the MRA follow-up in as many patients as possible. Patients without imaging follow-up in the past 4 years were invited for follow-up MRA by letter. If there was no response, we contacted the general practitioner to find out whether the patient was still alive, and if not, we asked for the date and cause of death. Patients in poor clinical condition in nursing homes were excluded from extended imaging follow-up. Patients with a contraindication for MR imaging were invited for follow-up conventional angiography.
Follow-Up MR Imaging and Indications for Retreatment
MR imaging was performed on a 3T system (Intera R10; Philips Healthcare, Best, the Netherlands) by using a phased array head coil (MR Imaging Devices, Gainesville, Florida) with sensitivity encoding.
The MR imaging protocol included axial and coronal T2-weighted fast spin-echo, coronal T1-weighted spin-echo, and high-resolution multiple overlapping thin-slab acquisition 3D time-of-flight MRA sequences. The MRA protocol was validated in the follow-up of coiled intracranial aneurysms.19
Reopening was defined as flow on MRA at the base of the aneurysm, caused by either compaction of the coil mesh, aneurysm regrowth, or migration of coils into intra-aneurysmal thrombus. Results of follow-up MRA were evaluated by a multidisciplinary team. In general, any reopening was an indication for additional coiling. Only exceptionally, additional treatment was not performed or postponed for anatomic or clinical reasons.
Statistical Analysis
Putative risk factors for retreatment of the basilar tip aneurysm were assessed with univariate logistic regression analysis. Odds ratios were calculated for the following variables: median aneurysm size, rupture status, sex, age at first treatment, and duration of follow-up in years. Then, multivariate logistic regression analysis was performed with reopening of the basilar tip aneurysm as a dependent variable. Aneurysms that were additionally coiled were expressed as a proportion, and timing of the first retreatment was graphically displayed in a cumulative event plot.
For ruptured basilar tip aneurysms, rebleed was expressed as an annual incidence rate with corresponding 95% confidence intervals and was graphically displayed in a cumulative event plot.
The occurrence of progressive mass effect by the aneurysm was also calculated as an incidence rate.
The t test was used for continuous variables, and the Fisher exact test, for categoric data. A P value < .05 was considered statistically significant. Statistical analysis was performed with MedCalc Statistical Software, Version 14.12.0 (MedCalc Software, Mariakerke, Belgium).
Results
Clinical and Imaging Follow-Up
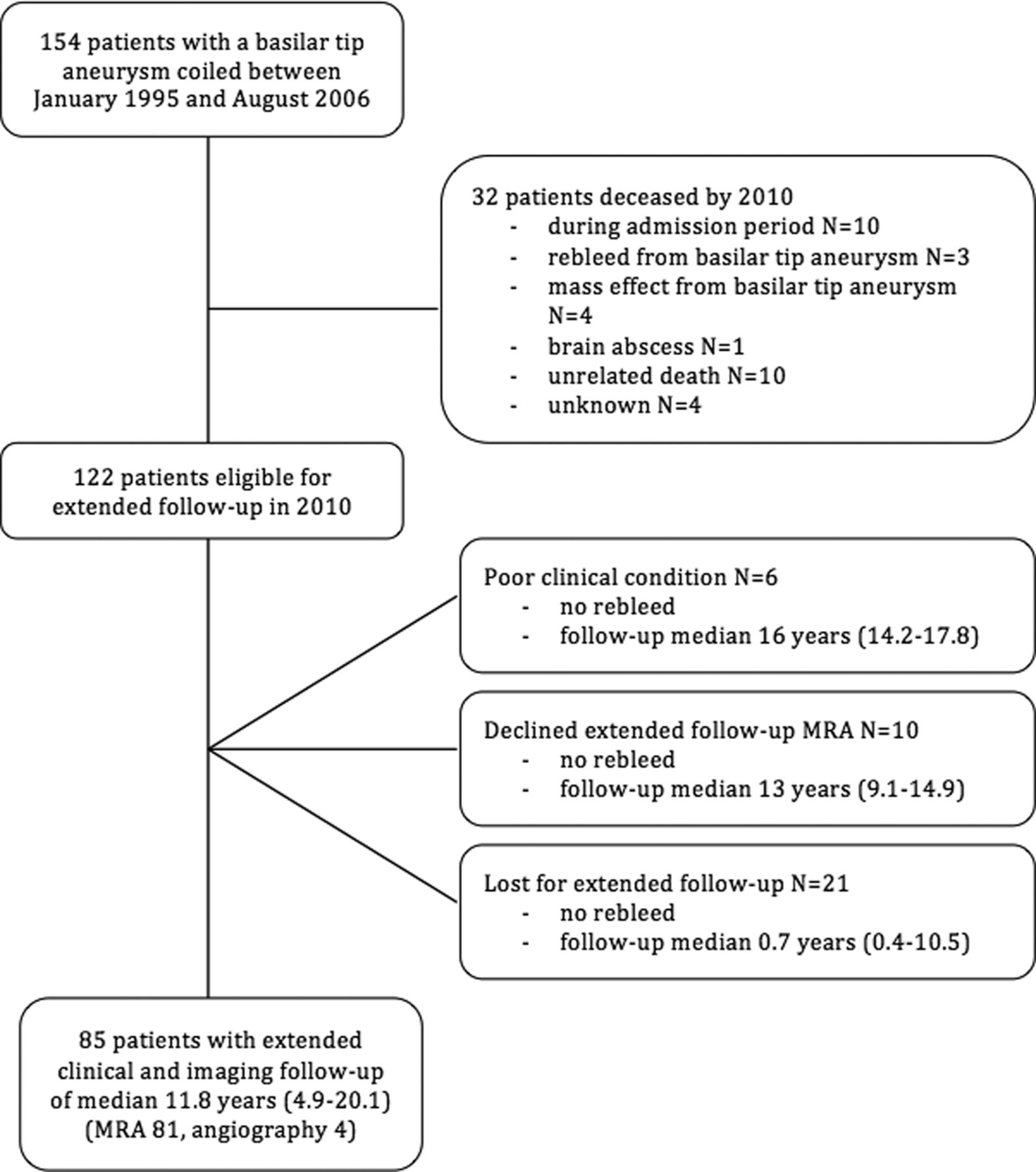
Figure 1 is a follow-up scheme of the cohort. Of 154 patients, 32 had died by 2010.

Follow-up scheme of 154 patients with a basilar tip aneurysm.
Of 122 patients who were eligible for extended follow-up in 2010, 85 (70%) had extended MRA (n = 81) or angiographic (n = 4) follow-up at a median of 11.8 years (range, 4.9–18.4 years). In 2 of these patients, angiography was performed after a rebleed from the basilar tip aneurysm at 16.6 and 15.2 years after coiling (Fig 2).

A 41-year-old man with a coiled ruptured basilar tip aneurysm in 1997 and a rebleed 15 years later. A, Angiography in 2006, 9 years after coiling in 1997, shows an adequately occluded basilar tip aneurysm. B, CT in 2012 demonstrates a rebleed from the basilar tip aneurysm. C, Angiography reveals regrowth of the aneurysm (arrow). D, After additional coiling, the aneurysm is completely occluded (arrow).
Incidence of Retreatment
Clinical follow-up of 144 patients who survived the admission period was for a mean of 9.8 years (median, 10.2 years; range, 0.3–20.1 years), totaling 1461 patient-years. During this period, 37 basilar tip aneurysms (26%) were additionally coiled. The annual incidence rate for retreatment was 2.5% (95% CI, 1.8%–3.5%).
The timing of the first additional coiling is graphically displayed in Fig 3. First additional coiling was performed in the first year of follow-up in 15 of 37 patients (41%) and in 22 patients (59%) later, up to 17.2 years after the first coiling. In 15 of 37 patients (41%), additional coiling was performed more than once and up to 5 times. The timing of additional treatments in these patients is displayed in Fig 4. In total, 68 additional coilings were performed during follow-up, all without complications (complication rate, 0%; 95% CI, 0%–5.7%).

Timing of first retreatments in 37 patients with reopened basilar tip aneurysms.

Timing of retreatments in 15 patients with coiled basilar tip aneurysms and >1 recurrence.
Risk Factors for Retreatment
The results of logistic regression analysis are summarized in Table 1. In univariate analysis, age at first coiling, ruptured aneurysm status, and the mean period of follow-up were not different between patients with or without additional coiling during follow-up. Male sex and median aneurysm size were significantly associated with additional coiling (OR, 2.6 and 1.1). Because large aneurysm size is a well-known risk factor for aneurysm reopening, aneurysm size was further analyzed in quintiles. Aneurysms of 16–30 mm had a 9-fold higher chance of retreatment during follow-up than aneurysms of 2–6 mm (OR, 8.5; 95% CI, 2.5–29.3).
Univariate analysis of risk factors for retreatment of coiled basilar tip aneurysms in 144 patients
In multivariate analysis, aneurysm size of >15 mm was a strong independent predictor (OR, 8.7; 95% CI, 3.4–22.5). In addition, male sex was an independent risk factor for retreatment (OR, 2.7; 95% CI, 1.1–6.5). Age at first treatment, the mean period of follow-up, and ruptured aneurysm status were not independent risk factors.
Incidence of Rebleed
The mean follow-up of 38 of 40 patients who presented with unruptured basilar tip aneurysms and who survived the first treatment was 8.5 years (median, 9.1 years; range, 0.3–17 years). There were no first-time hemorrhages in these patients.
The clinical follow-up of 106 patients with a ruptured basilar tip aneurysm who survived the hospital admission period was a mean of 9.8 years (median, 10.2 years; range, 0.4–18.7 years), totaling 1158 patient-years. Nine episodes of rebleed were recorded in 9 patients. Three patients died of the rebleed (0.3, 7.2, and 16.1 years after first treatment). Rebleeds occurred after a median follow-up of 8.3 years (range, 0.3–16.6 years). The annual incidence rate for rebleed was 0.7% (95% CI, 0.4%–1.5%).
Progressive Mass Effect
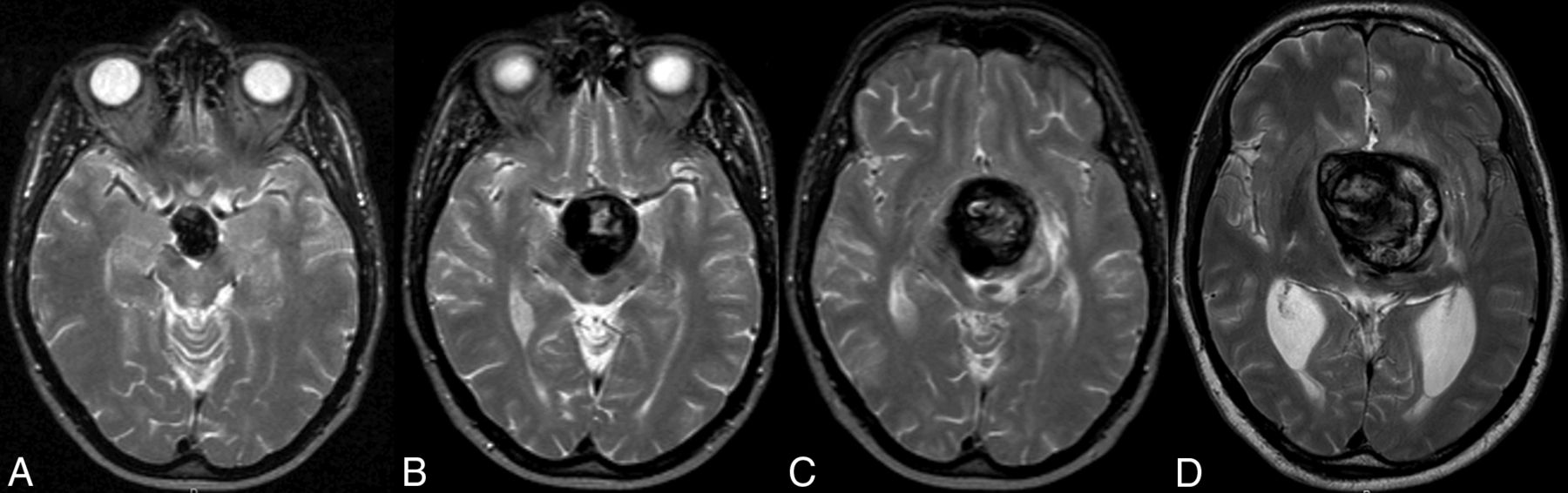
Progressive compression on the brain stem by continuous growth of the basilar tip aneurysm occurred in 6 patients (Fig 5). Follow-up in these patients was a mean of 7.2 years (median, 5 years; range, 0.5–17.8 years), totaling 42.8 patient-years (Table 2). The annual incidence rate of progressive mass effect was 0.4% (95% CI, 0.2%–0.9%). In 5 deceased patients, this was the cause of death; in 4 patients, it was by progressive brain stem compression. In 1 patient, progressive growth of the aneurysm in an anterior direction caused compression of the chiasm with loss of vision 10.8 years after the first coiling. Despite partial surgical resection of the aneurysm, the patient died 1 month later.

Serial MR images of a 40-year-old man with a coiled ruptured basilar tip aneurysm in 2003. A, Transversal T2-weighted MR image from December 2003 shows a basilar tip aneurysm 6 months after coiling. B, MR imaging in May 2008 shows enlargement of the aneurysm and compression of the brain stem. C, MR imaging in March 2009 shows further growth, now with edema in the brain stem. D, MR imaging in December 2009 shows a rapid increase in size with enormous compression of the brain stem. The patient died 1 month later.
Characteristics of 6 patients with progressive mass effect by continuous growth of the basilar tip aneurysm despite (repeat) coiling
Aneurysm-Related Mortality
During the follow-up period, 8 patients died of aneurysm-related adverse events: Three patients died of rebleed and 5 died of progressive mass effect from the basilar tip aneurysm.
Discussion
This long-term follow-up study of 154 coiled basilar tip aneurysms showed that retreatment during follow-up was performed in a quarter of patients. Almost half of retreatments were in the first year after coiling, but first retreatments were also performed up to 17 years after the first coiling. In 4 patients, the first retreatment was >10 years after coiling. A substantial proportion of retreated aneurysms were retreated more than once, up to 5 times. All retreatments were without complications. The incidence of retreatment of basilar tip aneurysms of 25% is significantly higher than that of aneurysms at other locations: In a meta-analysis by Ferns et al,1 the overall retreatment rate was 10%, with aneurysm sizes of >10 mm and location in posterior circulation as risk factors. There are probably 3 reasons for this higher incidence of retreatment in aneurysms located on the basilar tip: First, in general, all basilar tip aneurysms are coiled; they are also aneurysms with unfavorable anatomy and an inherent higher chance of reopening. Surgical clipping is rarely considered an alternative for coiling. Second, almost half of the basilar tip aneurysms were of large or giant size. Third, our follow-up duration was extremely long, and various first retreatments were performed at very long follow-up intervals: In 8 of 37 patients, the first retreatment was >8 years after the first coiling.
The most important independent risk factor for retreatment was aneurysm size; increasing aneurysm size increases the chance of reopening and retreatment. Large aneurysm size as a risk factor for reopening and retreatment is a well-known and consistent finding in follow-up studies after coiling.1⇓–3,5⇓⇓⇓⇓–10,12⇓⇓⇓⇓–17 The second independent risk factor was male sex. We have no explanation for this finding. In 1 previous study, male sex was also found to be a risk factor for reopening after coiling.7
Rebleeds occurred in 9 of 106 patients with ruptured basilar tip aneurysms who survived the admission period at time intervals ranging from 4 months to 16.6 years after coiling. In 3 patients, the rebleed was fatal. The annual incidence rate for recurrent hemorrhage was a 0.7%, low but higher than approximately 0.3% in other studies comprising aneurysms at all locations.20,21 This finding emphasizes the need for a regular and life-long follow-up scheme to detect reopening in a timely manner and prevent rebleeds by retreatment. Even after many years of stable aneurysm occlusion, reopening and rebleed may still occur.
Our study also demonstrated that most late mortality was due to continuous growth of some basilar tip aneurysms despite adequate first-time occlusion with coils and additional coiling when possible.22,23 Why this phenomenon occurs in some aneurysms remains unclear. We were unable to identify risk factors for this infrequent event. Aneurysm growth may become apparent at any time during follow-up. The growth rate varies, and episodes of growth may alternate with stable periods. Patients with a growing basilar tip aneurysm can present with various clinical signs because of compression on the brain stem, such as cognitive dysfunction with apathy and loss of initiative, motor and gait difficulties, and cranial neuropathies with or without signs of hydrocephalus. In our population, most patients presented with gradually progressive cognitive decline; 1 patient presented with progressive loss of vision from compression on the chiasm. The prognosis of a growing basilar tip aneurysm is poor, with variable times from onset of symptoms to death. Therapy can only be palliative, with steroids and treatment of hydrocephalus. Aneurysm debulking was performed in 1 patient but was not effective.
Our protocol for coiled aneurysms was fairly consistent during the follow-up period. Patients with large and giant basilar tip aneurysms and those who were coiled more than once had a tailored follow-up scheme, with MRA every 1–3 years. Patients with no regular follow-up scheme were actively contacted at different times to participate in various follow-up studies.2,5,10,12,13,16,18 Despite this close monitoring, in 2012, we encountered several unexpected serious late clinical adverse events in a short time in patients with coiled basilar tip aneurysms. At that point, we decided to recall patients without follow-up imaging in the past 4 years for MR imaging and MRA, and 85 of 122 eligible patients responded positively. This response resulted in a very long clinical and imaging follow-up for the cohort. There are no other comparable studies with very long-term follow-up of basilar tip aneurysms, to our knowledge.
This retrospective study has several drawbacks. Clinical and imaging follow-up was not complete in all patients. Some patients had irregular or large intervals between follow-up imaging, and the assessment of the timing of reopening was thus inaccurate. In some patients, the cause of death remained unknown. Not all patients responded positively to an invitation for extended imaging follow-up.
The principal conclusion from this extended follow-up study of coiled basilar tip aneurysms is that serious adverse events may become apparent for the first time very long after a first or additional coiling. Aneurysms may be stable for long periods before or after reopening or rebleed. Coiled basilar tip aneurysms that increase in size despite adequate occlusion at first or repeated treatment have a poor prognosis. The growth rate is unpredictable; it can be slow or quick and gradual or alternating. When hydrocephalus occurs, it should be treated. When brain stem compression is accompanied by edema, steroids may be administered as palliation. With our follow-up scheme, most aneurysm-related mortality was from continuous aneurysm growth, not from rebleeds.
Conclusions
A regular and life-long clinical and imaging follow-up protocol is advisable in patients with both ruptured and unruptured basilar tip aneurysms that have been coiled. In our opinion, yearly MR imaging should be adequate to detect reopening needing additional treatment in a timely manner. Recurrent episodes of hemorrhage can thus be prevented.
Footnotes
Drs van Eijck and Bechan contributed equally to this article.
References
- Received February 24, 2015.
- Accepted after revision March 24, 2015.
- © 2015 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}