
Article Figures & Data
Figures
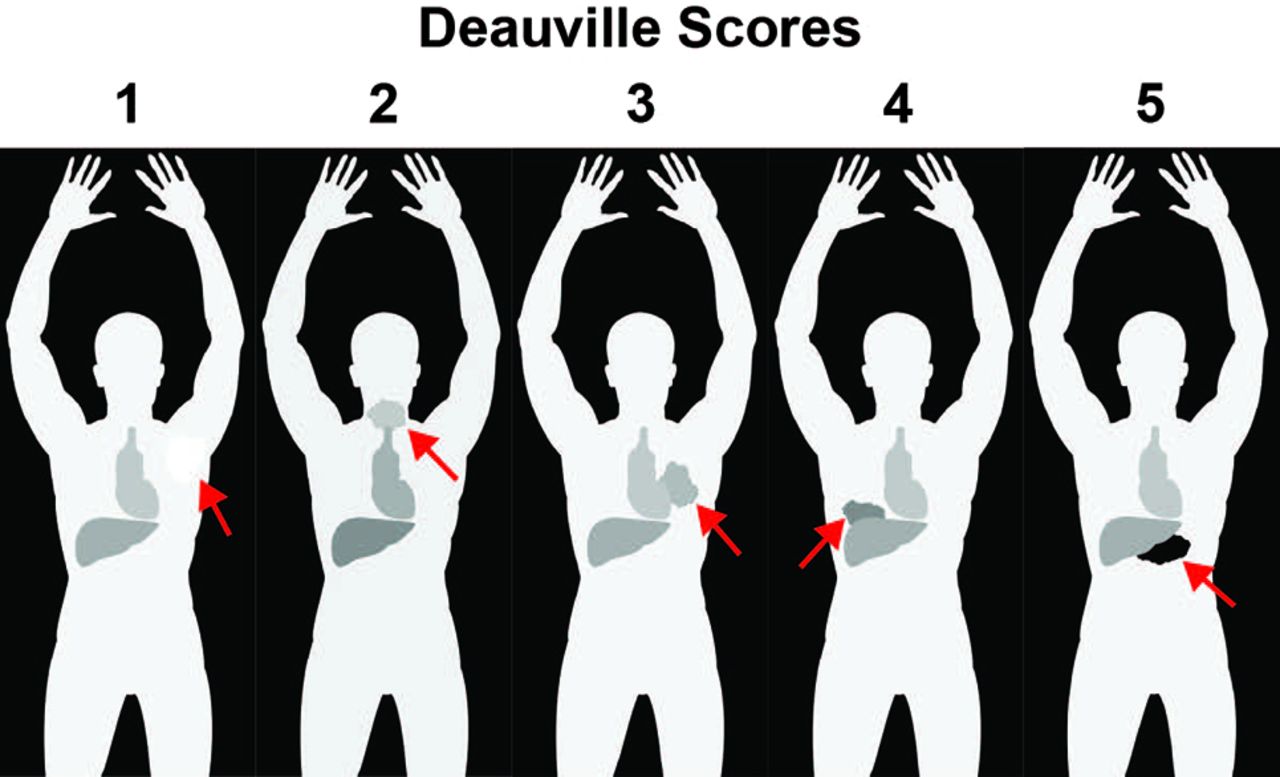
- Fig 1.
The D5PS scores of lesions qualitatively based on the FDG uptake relative to the mediastinal blood pool (MBP) and hepatic parenchymal FDG activity. The figure demonstrates hypothetical masses (arrows) and their FDG uptake relative to the MBP and liver activity. D5PS score of 1 for a left axillary mass with FDG uptake no greater than background activity. D5PS score of 2 for cervical mass with FDG uptake above background but less than MBP or liver. D5PS score of 3 for hilar mass with FDG uptake greater than MBP but less than or equal to the hepatic activity. A D5PS score of 4 for a mass in right lung base with FDG uptake greater than both MBP and liver. A D5PS score of 5 for a midabdominal mass with FDG uptake markedly greater than that of the liver.
- Fig 2.
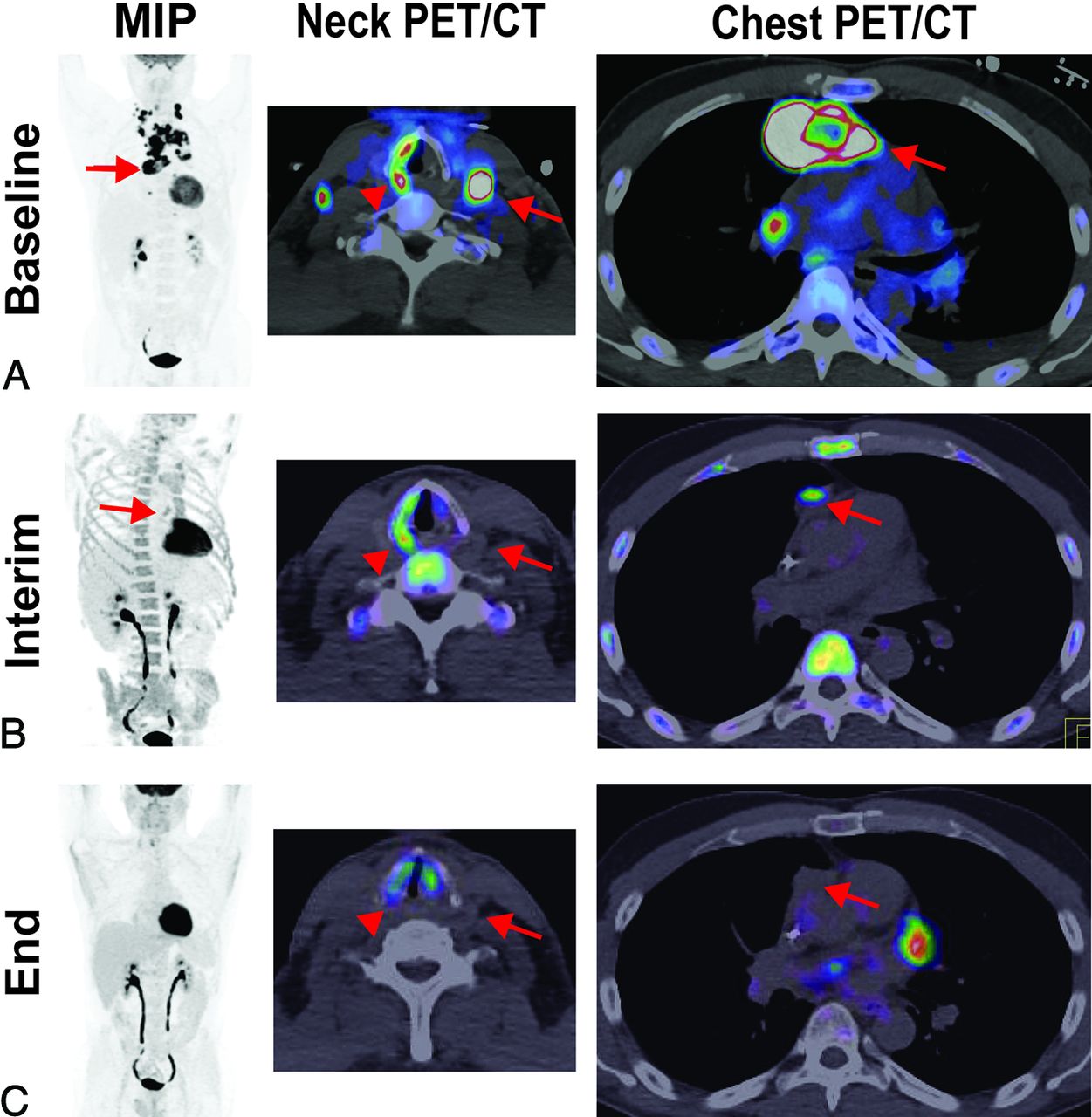
A partial metabolic response and CMR based on Lugano criteria. A 47-year-old man with diffuse large B-cell lymphoma demonstrates (A) baseline intense FDG avidity in mediastinal (MIP and PET/CT of the chest [arrows denote a large pericardial lymph node conglomerate]) and bilateral levels III and IV lymphadenopathy (PET/CT of the neck [arrow denotes a large level III node]), a D5PS score of 5. Incidentally, on the PET/CT of the neck, the arrowhead denotes a dysfunctional right vocal cord, likely due to disease impacting the ipsilateral recurrent laryngeal nerve. B, Interim imaging demonstrates reduced but persistent FDG uptake (2 times greater than the liver) in the retrosternal, pericardial mass (MIP and PET/CT of the chest [arrows]), consistent with a D5PS score of 5 but a Lugano designation of a partial metabolic response. There was interval resolution of the cervical lymphadenopathy. C, End-of-treatment imaging shows a residual pericardial mass on CT (arrow), without FDG uptake above background, consistent with a D5PS score of 1 and a Lugano designation of CMR.
- Fig 3.
A posttreatment D5PS score of 5 but partial metabolic response based on Lugano criteria. Baseline imaging demonstrates diffuse lymphadenopathy, including cervical levels II–IV, axillary, mediastinal, abdominal periaortic/pericaval, and right greater than left iliac chains, with intense FDG avidity (arrows), consistent with a D5PS score of 5. Interim imaging during treatment demonstrates significantly reduced size and FDG avidity of the cervical, axillary, and mediastinal lymphadenopathy (arrows), now predominantly limited to the periaortic/pericaval regions and right greater than left iliac chains. The lymph nodes still have FDG avidity markedly greater than mediastinal blood pool and liver, consistent with a D5PS score of 5, but the reduction in size, number, and intensity results in a Lugano designation of a partial metabolic response.
- Fig 4.
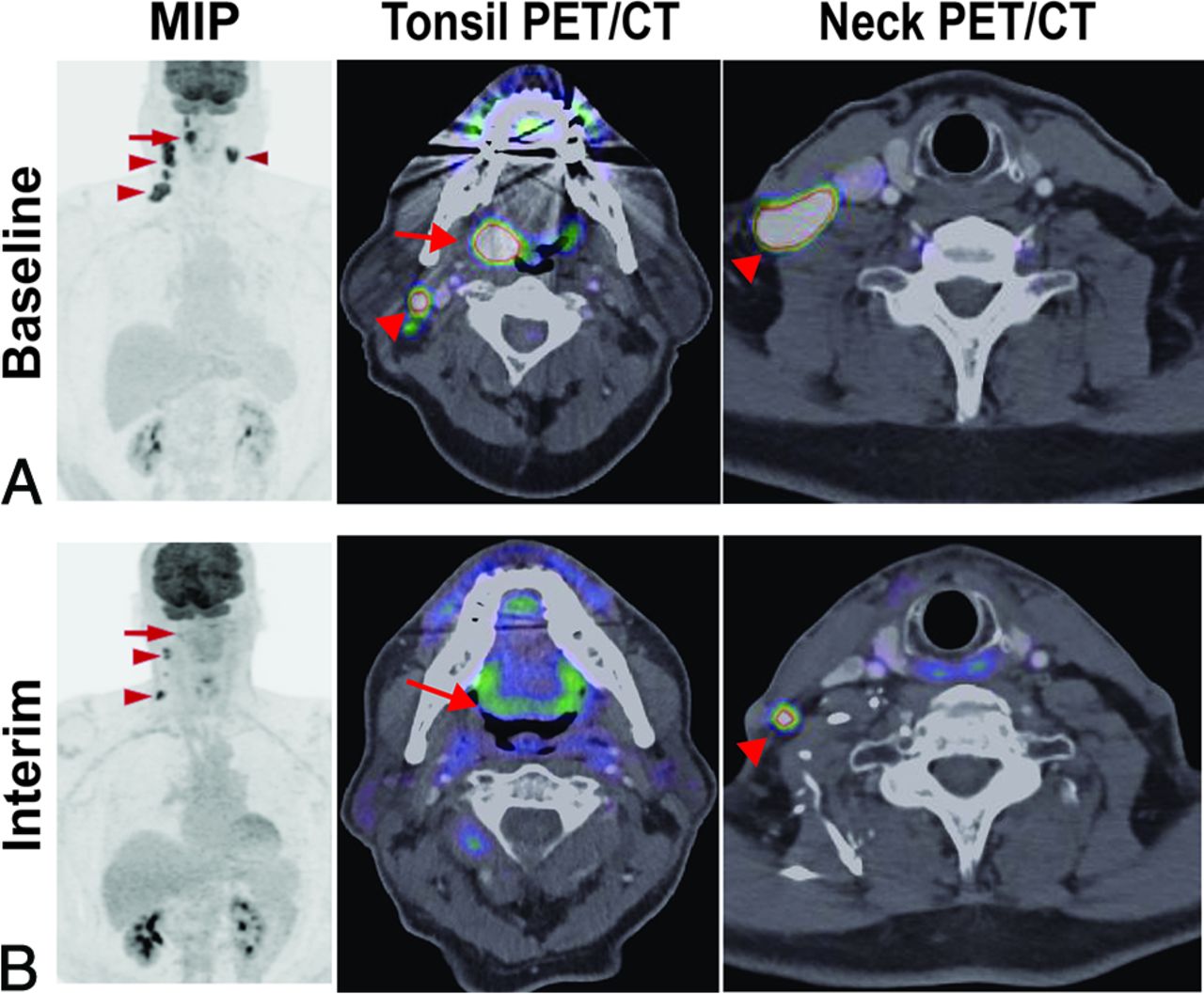
Hopkins criteria score of 5 in right tonsillar squamous cell carcinoma, consistent with residual tumor. A 71-year-old man with right tonsillar squamous cell carcinoma. MIP from baseline PET/CT demonstrates a Hopkins criteria score of 5 in the primary right tonsillar tumor (arrow) and right greater than left level II–IV cervical lymph nodes (arrowheads). Examination after radiation and chemotherapy shows resolution of the right tonsillar FDG uptake (arrow) and some of the cervical lymph nodes but persistent, focal, and intense FDG uptake in 2 ipsilateral level III and IV lymph nodes (arrowheads); a Hopkins criteria score of 5 is consistent with residual tumor.
- Fig 5.
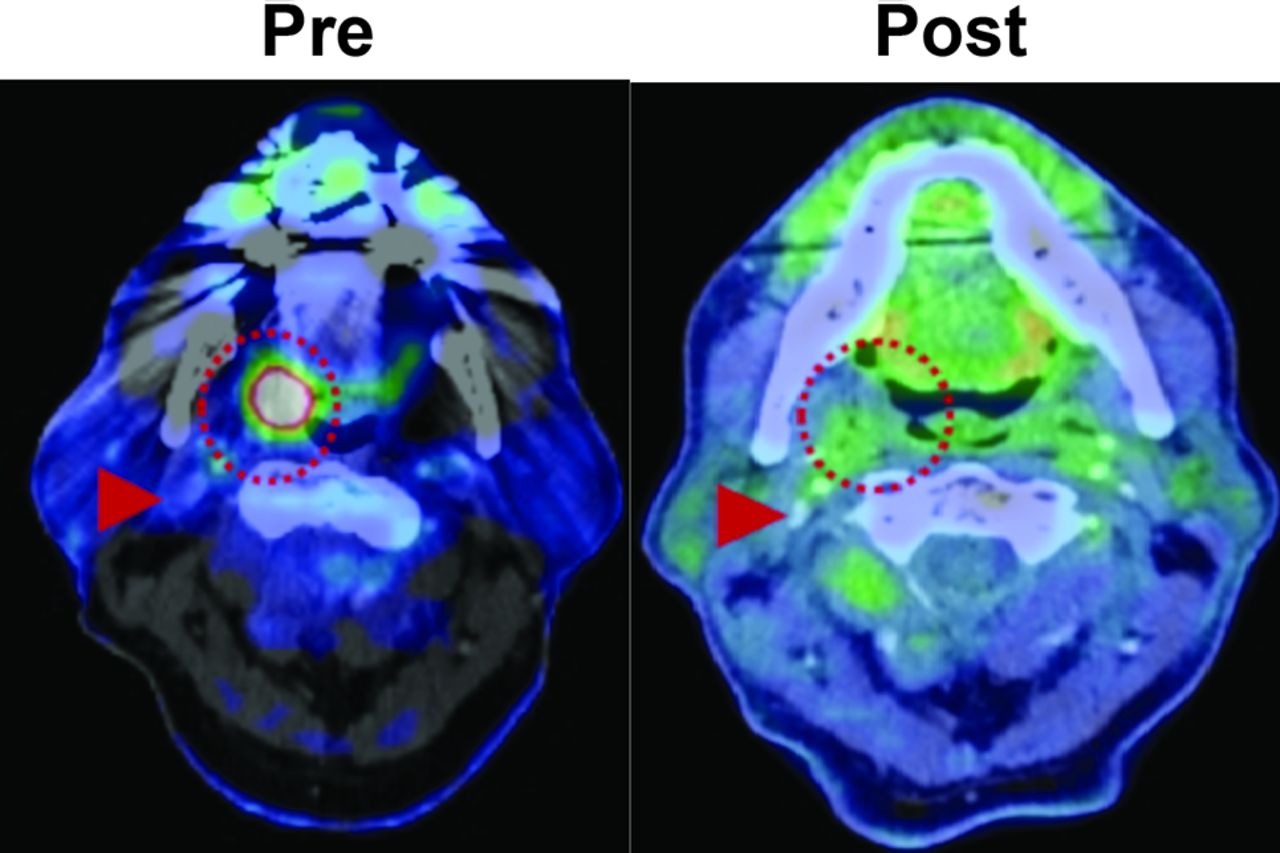
Hopkins criteria score of 2 and NI-RADS score of 1 in right tonsillar squamous cell carcinoma, consistent with a CMR. A 71-year-old man with an intensely FDG-avid right tonsillar squamous cell carcinoma (dotted circle) on pretreatment PET/CT. After treatment, the mass has resolved, with FDG uptake in the region just above the adjacent right internal jugular vein (arrowhead) but similar to the surrounding oropharyngeal soft tissues, consistent with a Hopkins criteria score of 2 and an NI-RADS score of 1 at the primary site. By using Hopkins or NI-RADs criteria, the findings are consistent with an overall CMR.
- Fig 6.
An NI-RADS score of 2a in left tonsillar squamous cell carcinoma (SCCa) after chemoradiation, consistent with a Hopkins criteria score of 3 and posttreatment inflammation. A 63-year-old man with a history of left tonsillar SCCa. A, Baseline oblique MIP shows markedly hypermetabolic primary left tonsillar SCCa (arrow). After completion of chemoradiation therapy, repeated FDG PET/CT was obtained. B, Oblique MIP and axial PET/CT show residual hypermetabolic mucosal activity of moderate intensity (arrow) throughout the tonsil bed. The findings are compatible with NI-RADS 2a. Linked management recommendations in the NI-RADS criteria suggest correlation with direct visualization given that such a finding typically represents non-neoplastic FDG uptake. As a comparison, the FDG uptake is greater than the liver and much greater than the internal jugular vein, this is consistent with a Hopkins criteria score of 3. The findings suggest benign posttreatment inflammation. Lesions with this score can be false-negatives and demonstrate intermediate overall survival and progression-free survival compared with scores of 1–2 and 4–5. Due to the false-negative probability, these lesions should be biopsied before altering the treatment plan.






Tables
Technique Complete Response Partial Response No Response PD CT Complete disappearance of disease or decrease in the lymph node long axis to <1.5 cm Multiple: ≥ 50% decrease in SPD of up to 6 lesions. Single: ≥ 50% decrease in PPD No criteria for PD and <50% decrease in SPD of up to 6 lesions. (1) New or increased lymphadenopathy (long axis >1.5 cm): new nodes, ≥ 50% increase in PPD, or >0.5 cm increase in diameter for ≤2 cm or >1.0 cm for >2 cm; (2) splenic volume increase: with splenomegaly, >50% increase in length, or without splenomegaly, ≥2 cm increase in length; (3) new or larger lesions; (4) recurrent previously resolved lesions; (5) new extranodal lesion >1 cm (or <1 cm if unequivocally lymphoma) FDG-PET/CT D5PS score of 1, 2, or 3 in disease sites, with or without residual mass D5PS score of 4 or 5, with reduced uptake compared with baseline D5PS score of 4 or 5, with no signficant change in FDG uptake D5PS score of 4 or 5, with increased uptake intensity compared with baseline and/or new FDG-avid foci Note:—SPD indicates sum of the product of the diameters (PPD).
↵a For non-FDG avid lymphomas, the following CT-based measurement criteria are used to determine tumor response classification; adapted from Ref. 15.
D5PS Scoreb Lesion FDG Uptake 1 At or below background 2 Less than or equal to mediastinal blood pool 3 Greater than or equal to mediastinal, but less than hepatic blood pool 4 Greater than hepatic blood pool 5 Markedly greater than hepatic blood pool X Designator for nonlymphomatous lesion Hopkins Criteria Scoreb Lesion FDG Uptake Therapy Response 1 Focal uptake less than IJV CMR 2 Focal uptake greater than IJV, but less than liver Likely CMR 3 Diffuse uptake greater than IJV and liver Likely posttreatment inflammation 4 Focal uptake greater than liver Likely residual tumor 5 Focal uptake markedly greater than liver Residual tumor Description Category Imaging Findings Management Incomplete 0 New baseline study or unavailable previous imaging Previous imaging No evidence of recurrence 1 Posttreatment changes without mass or abnormal FDG uptake Routine surveillance Low suspicion (superficial) 2a Enhancement without FDG uptake or mild/moderate FDG uptake without a mass Direct visual inspection Low suspicion (deep) 2b Enhancement without FDG uptake or mild/moderate FDG uptake without a mass Short imaging follow-up High suspicion 3 New or enlarged mass or lymph node, enhancement, and intense FDG uptake Biopsy Definitive recurrence 4 Pathologically proved or definite progression Clinical management ↵a The NI-RADS risk stratification guidelines grade head and neck tumor treatment response; adapted from Ref. 26.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}