
Article Figures & Data
Figures
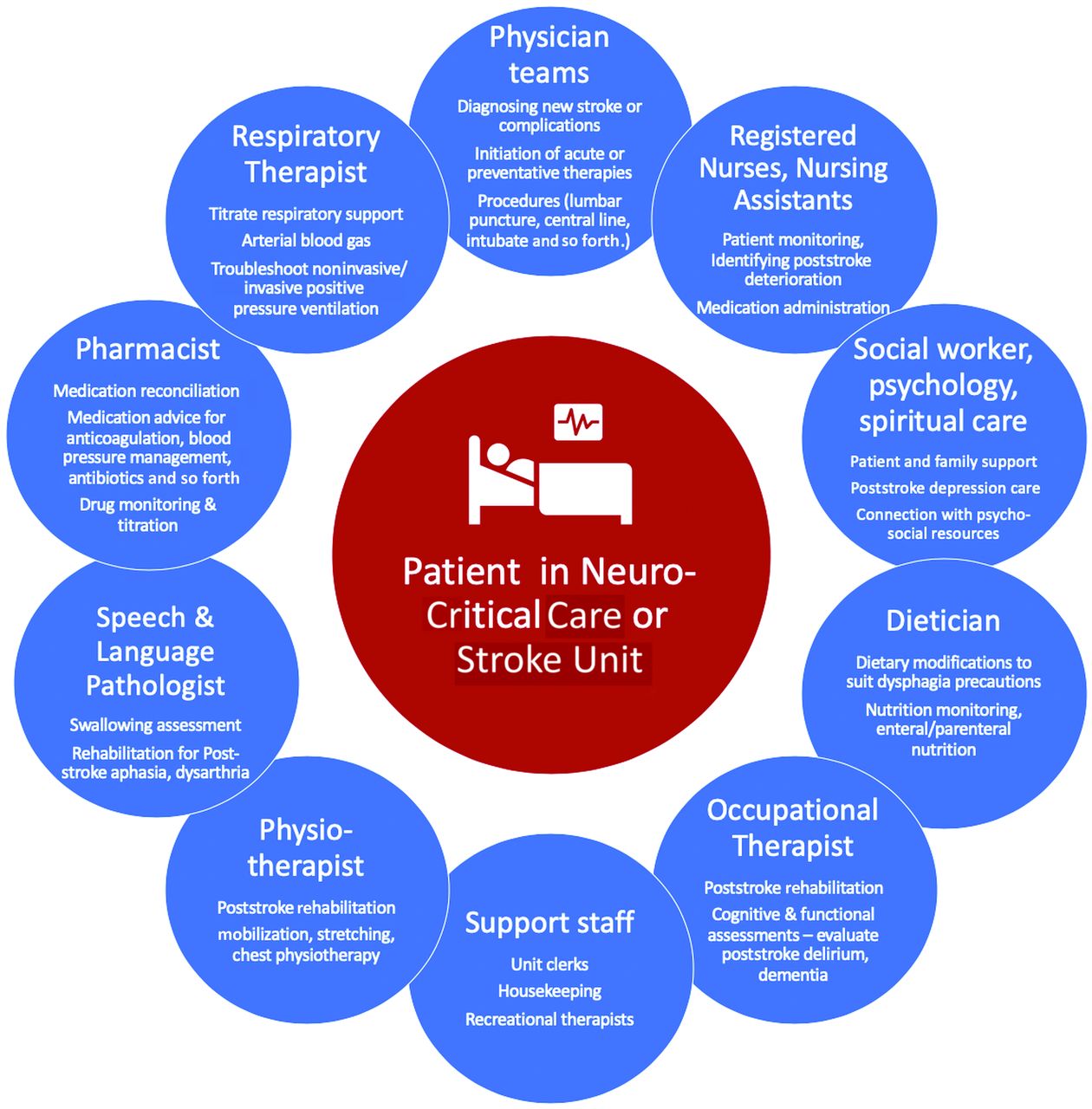
- FIGURE.
A model of patient-centered multidisciplinary care in the Neuro-ICU or stroke unit that is both helpful and reassuring for new staff members. The model is quite similar in both the neuro-critical care and stroke units with the notable exception of respiratory therapists who are often not part of medical stroke units. While this model is, of course, generalizable to nonstroke settings as well, some specific examples are illustrated to show how different members of the team may synergistically address a stroke-related problem. For example, in a patient with dysphagia, the nursing or physician team may be the first to notice a poststroke deterioration with the patient choking or coughing during a simple trial. This prompts the team to involve the speech and language pathologist who confirms poststroke dysphagia and recommends a temporary nasogastric tube, which is inserted by a nurse (perhaps with a new nursing team member observing this common task), with the dieticians then helping ensure that the nasogastric feed provided meets the patient’s feeding requirements, potentially monitoring for a refeeding syndrome. These changes may be overwhelming for the patient and family, prompting the team to involve psychology to assess poststroke depression as well as social work and spiritual care to connect the patient and family to key resources.

Tables
- Table 1:
Four key principles for integration of new staff in the stroke team during a health care crisis
Key Principle Explanation/Implementation Strategy Example Transfer of key knowledge New staff members should be primarily taught the key principles of their new working environment; these should be kept as brief and concise as possible in order not to overwhelm new staff Neuroangiography suite: never walk in the room without a lead apron if a patient is on the table Neuro-ICU: never use a nasogastric tube until proper placement has been confirmed by a clinician (most commonly by a portable chest x-ray) Stroke unit: never feed a patient with stroke with dysphagia solid food until a swallow screen has been performed Open communication and nonjudgmental atmosphere New staff members have to feel comfortable telling core members if they do not feel comfortable doing a certain task and should not hesitate to ask for help or advice A new staff member is told to monitor a patient on an alteplase infusion but does not know what symptoms or signs to look for; he or she explains this to the supervisor who reassigns the patient to a more experienced member and helps train the new member in this important task Strategic task assignment To avoid mistakes and treatment delays, new team members should execute tasks that are as closely related as possible to their core field of expertise A nurse from the nephrology ward joins the stroke team; he or she is familiar with management of patient vitals but not with neuroangiography-specific terminology, eg, guidewire, balloon-guide catheter; thus, the task should be focused on management of patient vitals rather than procedure-specific peculiarities Graded responsibility and learning New staff members should gradually take on new tasks and responsibilities; they should feel comfortable performing a certain task and be capable of executing it safely before they are assigned additional, more complicated tasks A schedule that pairs shifts of new team members with core team members; new team members are intermixed in new roles, as they have to learn new and complex tasks - Table 2:
Take-home points for new staff and unique-versus-generic aspects of stroke care in the neuroangiography suite
Most Important Teaching Points (Take-Home Points) for New Team Members Unique Characteristics of the Neuroangiography Suite Environment (Not Ideal Tasks for New Team Members) Generic Aspects of the Neuroangiography Suite Environment That Are Similar to Those in Other Medical Areas (Appropriate Initial Tasks for New Team Members) Radiation awareness Handling the groin puncture/access site Blood pressure control,1 hemodynamic monitoring Boundaries between sterile vs nonsterile environment Handling of catheters and devices Management of IV lines Location of key emergency drugs and equipment (epinephrine, oxygen, intubation kit), key/safe combinations in case some drugs (eg, opiates) are stored in a safe Navigating the angiography machine Clinical monitoring of the patient during the procedure Phone numbers and schedule of neurointerventionalists, anesthesiologists, techs, and nurses on call Image reconstruction and labeling Documentation of patient status - Table 3:
Take-home points for new staff and unique-versus-generic aspects of stroke care in the Neuro-ICUa
Most Important Teaching Points (Take-Home Points) for New Team Members Unique Characteristics of the Neuro-ICU Environment (Not Ideal Tasks for New Team Members) Generic Aspects of the Neuro-ICU Environment That Are Similar to Those in Other Medical Areas (Appropriate Initial Tasks for New Team Members) Key components of neuromonitoring (vital signs, neurologic vital signs: pupils, Glasgow Coma Scale, intracranial pressure, NIHSS score, and so forth) Resuscitation of unstable patient on initial presentation or with complications (eg, procedures surrounding airway management, status epilepticus treatment, intracranial pressure/herniation treatment, shock management, and so forth) Monitoring vital parameters, level of consciousness, and respiratory parameters of nonintubated patients Recognizing potential life-threatening complications Monitoring patients on invasive or noninvasive positive pressure ventilation Management of enteral feeds and IV fluids Location of key equipment (code cart, difficult airway cart) and medications Care and use of arterial and central lines, administration of vasopressors Basic medication administration (may include managing alteplase/tenecteplase infusions, depending on background) Team members and rolesChain of help, contact information (pager/phone)Examples: ICU buddy team member (RN, RT, pharmacist, and so forth), charge nurse, NCC/stroke fellow, NCC/stroke attending physician on call Use and interpretation of multimodal neuromonitoring:Intracranial pressure monitors (external ventricular drain)Cerebral oxygenation monitors: continuous brain tissue oxygenation, near-infrared spectroscopy, jugular venous catheterCerebral blood flow monitorsCerebral microdialysisContinuous electroencephalography Placement and care of nasogastric/orogastric tube, IV line, Foley catheter, and so forth Key elements of AIS/ICH/SAH management (see also Table 4), basic and advanced life support Brain death assessments and management Bathing, turning, mobilizing patients Organ donation: donation after circulatory death or donation after neurologic death Charting/documentation of patient course Palliation, depending on circumstances; for patients with COVID-19, institutions may have unique policies for automatic do-not-resuscitate orders or care limitations that incorporate neurologic prognosis formation Note:—RN indicates registered nurse; RT, respiratory therapist; NCC, neurocritical care; AIS, acute ischemic stroke; ICH, intracerebral hemorrhage.
↵a For specific Neuro-ICU take-home points for the management of patients with acute ischemic stroke, intracranial hemorrhage, and subarachnoid hemorrhage, see On-line Table.
- Table 4:
Take-home points for new staff and unique-versus-generic aspects of stroke care on the stroke unit
Most Important Teaching Points (Take-Home Points) for New Team Members Unique Characteristics of the Stroke Unit Environment (Not Ideal Tasks for New Team Members) Generic Aspects of the Stroke Unit Environment Similar to Other Medical Areas (Appropriate Initial Tasks for New Team Members) Recognizing an acute stroke, recurrent stroke, and abrupt neurologic deterioration of recent ischemic or hemorrhagic stroke Monitoring a patient in the unit after receiving IV alteplase (involves watching for angioedema, bleeding, frequent neurologic vital sign monitoring, close blood pressure control, and so forth) Obtaining/interpreting scheduled vital signs (temperature, blood pressure, heart rate, respiratory rate, oxygen saturation) and point-of-care blood glucose in patients Managing infusions of alteplase for stroke or of heparin (eg, for intraluminal thrombosis, venous sinus thrombosis) Being part of the acute stroke thrombolysis team (being comfortable with the “code stroke” and mixing alteplase) Foley catheter insertion, urinary dipstick testing, and identification of potential urinary tract infection Grossly identifying patients who are potentially aspirating versus those safe to swallow Managing a patient at risk of malignant middle cerebral artery or cerebellar stroke (involves closely watching for neurologic deterioration and liaising with stroke/neurosurgery team for potential decompressive craniectomy) Managing the patient’s routine medications and reconciling them with those taken preadmission NG insertion, feeding, and NG medication administration Managing a patient with a major intracranial hemorrhage (involves watching for emerging symptoms of hydrocephalus or major hematoma expansion that may warrant neurosurgical intervention or ICU transfer) Caring for a patient in the subacute-to-chronic poststroke period with/without medical issues like urinary tract infection, cellulitis, or pressure ulcers Performing a NIHSS bedside examination Receiving a patient after thrombectomy (involves monitoring the groin puncture site or managing hematoma) Evaluation and initial management of a patient with chest pain or shortness of breath (eg, poststroke myocardial infarction, aspiration pneumonia) Pager or phone numbers and schedule of stroke fellows and neurologists on call Receiving a patient after carotid endarterectomy (involves watching for reperfusion complications, lower cranial neuropathies interfering with swallowing) Evaluation and initial management of a patient with deep vein thrombosis Understanding basic stroke mechanisms for early secondary prevention Defining a stroke mechanism through a sophisticated understanding of neurovascular anatomy, localization, and cerebrovascular syndromes Working with patient and pharmacy to ensure proper dosing and administration of early secondary stroke prevention (eg, antithrombotics, statin therapy, blood pressure regimen, smoking cessation) Note:—NG indicates nasogastric tube.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.