
Abstract
BACKGROUND AND PURPOSE: Selective voluntary motor control is an important factor influencing gross motor function, interjoint coordination, and the outcome of hamstring-lengthening surgery in spastic cerebral palsy. Using DTI, we investigated whether selective voluntary motor control would show strong correlations with WM motor tract microstructure and whether selective voluntary motor control is more sensitive to global WM impairment than gross motor function.
MATERIALS AND METHODS: Children with spastic bilateral cerebral palsy born preterm and typically developing children were recruited. The Selective Control Assessment of the Lower Extremity (SCALE) and Gross Motor Function Measure (GMFM) were assessed in participants with cerebral palsy. Participants underwent brain MR imaging to collect DWI data. Tract-Based Spatial Statistics was used to analyze the WM for between-group differences and correlations with SCALE and GMFM. ROI analyses compared motor regions.
RESULTS: Twelve children with cerebral palsy (mean age, 11.5 years) and 12 typically developing children (mean age, 10.3 years) participated. Altered DTI outcomes were found throughout the whole brain for the cerebral palsy group. SCALE, developed to evaluate selective voluntary motor control in cerebral palsy, showed significant positive correlations with fractional anisotropy in more WM voxels throughout the whole brain and for motor regions, including the corticospinal tract and corpus callosum, compared with GMFM. A significant negative correlation between radial diffusivity and SCALE, but not GMFM, was found within the corpus callosum.
CONCLUSIONS: SCALE was a more sensitive clinical correlate of motor and whole-brain WM tract impairment in children with spastic bilateral cerebral palsy, suggesting greater anisotropy and myelination in these regions for those with higher selective voluntary motor control.
ABBREVIATIONS:
- AD
- axial diffusivity
- CC
- corpus callosum
- CerPed
- cerebral peduncle
- CP
- cerebral palsy
- CST
- corticospinal tract
- FA
- fractional anisotropy
- GMFCS
- Gross Motor Function Classification System
- GMFM
- Gross Motor Function Measure
- MD
- mean diffusivity
- PLIC
- posterior limb of the internal capsule
- RD
- radial diffusivity
- SCALE
- Selective Control Assessment of the Lower Extremity
- SCR
- superior corona radiata
- SVMC
- selective voluntary motor control
- TDC
- typically developing children
Periventricular leukomalacia is an MR imaging finding associated with perinatal injury to the cerebral WM. Children born prematurely are at higher risk of neurologic sequelae, including spastic bilateral cerebral palsy (CP) associated with periventricular leukomalacia.1⇓-3 Within spastic bilateral CP, there is a wide range of clinical outcomes, and lower extremity function varies among individuals. The microstructural properties of cerebral WM and the neuronal organization associated with the range of motor impairments in spastic CP are not well-understood.1,2
Spastic CP is associated with damage to the corticospinal tract (CST) and other motor pathways that are responsible for selective voluntary motor control (SVMC). SVMC reflects the ability to perform isolated, skilled, and precise movements of a joint or limb with control of force and speed on request.4 Impaired SVMC affects coordination between the lower extremity joints, resulting in coupling of the hip, knee, and ankle to varying degrees.5 SVMC was shown to have a strong influence on the gait and mobility characteristics of children with spastic CP.6,7 In addition, it has been used as a prognostic factor for hamstring surgery8 and selective posterior rhizotomy.9 SVMC, as measured by the Selective Control Assessment of the Lower Extremity (SCALE)4, had a larger causal effect on gross motor function compared with dynamic motor control (based on gait electromyography), strength, spasticity, contractures, and bony deformities.7
DTI is often used to assess microstructural WM differences in children with spastic bilateral CP.1,2,10,11 This MR imaging technique provides image contrast based on the translational displacement or diffusion of water molecules in the brain.12,13 DTI measures of fractional anisotropy (FA), radial diffusivity (RD), axial diffusivity (AD), and mean diffusivity (MD) provide details about tissue alterations associated with WM damage in CP.12,13 In clinical populations and relative to normative values, lower FA has been interpreted as a local marker of the disruption of local tissue microstructural anisotropy, higher RD has corresponded with damaged myelination, lower AD has reflected axonal injury, and higher MD has indicated greater overall diffusivity within a region.12⇓-14 Together, these DTI outcomes reveal a holistic picture of microstructural differences in cerebral WM.
WM differences between children with spastic CP and typically developing children (TDC) have previously been found using DTI.1,2,10,11 Motor function in children with spastic bilateral CP involves multiple regions of the brain beyond the CST and motor regions, including the commissural and association tracts and the visual, limbic, and sensory regions.1,15 Therefore, methods and approaches that focus on a set of a priori regions ultimately limit the scope of analysis and may underestimate the global extent of WM differences.12 In contrast, Tract-Based Spatial Statistics (TBSS; http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/TBSS), a whole-brain voxel-based approach, is a comprehensive method to assess WM. Altered WM in spastic bilateral CP relative to TDC has been found using voxel-based approaches including TBSS.1,2,10 In addition, correlations between DTI outcomes and a measure of mobility using the Gross Motor Function Classification System (GMFCS),16 a categoric score, have been reported.2,10 While prior DTI correlation analyses have used this mobility classification system to assess CP severity, none have used a motor performance measurement that includes SVMC.
To our knowledge, this is the first study to evaluate the relationships between a clinical measure of SVMC in spastic CP and DTI outcomes for motor regions of the brain. SVMC was assessed using SCALE.4 Our primary hypothesis was the following: 1) SCALE would show a significant correlation with DTI outcomes in the motor tracts, particularly the CST; and 2) SCALE would be more sensitive to WM impairment than the Gross Motor Function Measure (GMFM),17 a measure of gross motor function in spastic CP. Our secondary hypothesis was that significantly different DTI outcomes would be found for children with CP compared with a control group of TDC.
MATERIALS AND METHODS
Participants
This study was conducted in an outpatient clinical research center (Center for CP at UCLA/OIC and Ahmanson-Lovelace Brain Mapping Center). The institutional review board of the University of California Los Angeles provided ethics approval. Informed consent and assent for research were obtained from the children and their parents or guardians.
Inclusion criteria for all participants were the following: 1) between 5 and 18 years of age, 2) the ability to understand and follow verbal directions, and 3) the ability to lie still. Additional inclusion criteria for the CP group were the following: 1) a history of prematurity, 2) a diagnosis of spastic bilateral CP and periventricular leukomalacia as evidenced by MR imaging or sonography, and 3) the ability to walk with or without assistive devices.
Exclusion criteria for all participants were the presence of the following: 1) metal implants not verified as MR imaging–safe, 2) programmable implants including ventriculoperitoneal shunts and intrathecal baclofen pumps, and 3) dental braces. Additional exclusion criteria for children with CP were the following: 1) seizures not controlled by medication, 2) orthopedic surgery or neurosurgery within 1 year of starting the study, and 3) botulinum toxin or casting within 3 months of starting the study. Additional exclusion criteria for the TDC group were neurodevelopmental, neuromuscular, or neuropsychiatric diagnoses and visible abnormalities as observed on T1-weighted structural scans.
Clinical Assessments
The CP group was evaluated by experienced physical therapists using standardized protocols. GMFM dimensions D (standing) and E (walking, running, and jumping) were assessed.17 The GMFM-66 Gross Motor Ability Estimator program was used to compute the final scores. SCALE was used to assess SVMC.4 Specific isolated movement patterns at the hip, knee, ankle, subtalar, and toe joints were evaluated bilaterally. SCALE scores for each limb ranged from 0 (absent SVMC) to 10 (normal SVMC).4 Left and right limb scores were summed for a total SCALE score with a maximum value of 20.
MR Imaging Protocols
Before MR imaging sessions, children viewed a slide presentation describing MR imaging procedures and practiced lying still for 10 minutes while listening to recordings of MR imaging sounds. Movies were provided during the MR imaging acquisition for children to view on request. All T1WI and DWI scans were acquired using a 32-channel coil on a 3T Magnetom Prisma MR imaging scanner (Siemens). T1-weighted MPRAGE images were obtained using TR = 2500 ms; TE = 1.8, 3.6, 5.39, and 7.18 ms; FOV = 256 × 256 mm2; and isotropic voxel resolution = 0.8 × 0.8 × 0.8 mm3. DWI scans were obtained using a single-shot, spin-echo, echo-planar acquisition with 6 reference images (b = 0 s/mm2), 52 gradient directions (b = 1500 s/mm2), TR = 3231 ms, TE = 89.6 ms, FOV = 210 × 210 mm2, echo spacing = 0.69 ms, and isotropic voxel resolution = 1.5 × 1.5 × 1.5 mm3.
Statistical Analysis
TBSS, a whole-brain voxel-based approach, was used to assess differences in DTI outcomes between the CP and TDC groups and correlations between DTI outcomes and SCALE and GMFM in the CP group. Whole-brain analyses of DTI outcomes FA, RD, AD, and MD were performed with TBSS using the FMRIB (FSL) Diffusion Toolbox (http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/FDT).18 The mean WM skeleton used in this analysis was derived from and overlaid on the FMRIB58 standard-space FA template (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/FMRIB58_FA). Results were obtained after 5000 permutation-based randomized tests and corrected for multiple comparisons (P < .05) using the threshold-free cluster enhancement procedure.19 Voxels with significant differences and correlations were projected separately onto the mean WM skeleton.
ROI analyses were performed to quantify voxels with significant findings within specific regions of the brain. Using the Johns Hopkins University ICBM-DTI-81 WM atlas labels (http://neuro.debian.net/pkgs/fsl-jhu-dti-whitematter-atlas.html),20 we transferred ROIs to all images produced in the TBSS pipeline after nonlinear warping to the standard Montreal Neurological Institute 152 space and skeletonization. ROIs located along the descending pathways of the CST were parcellated bilaterally into the following regions (Fig 1A): 1) area inferior to the cerebral peduncle (sub-CerPed), 2) cerebral peduncle (CerPed), 3) posterior limb of the internal capsule (PLIC), and 4) superior corona radiata (SCR). The sub-CerPed ROIs are labeled as CST in the Johns Hopkins University WM atlas labels. ROIs for the corpus callosum (CC) were the genu, body, and splenium.

TBSS results show significant differences (P <.05) in DTI measures between the CP and TDC groups. Coronal slices were selected at the level of the CST. From left to right, axial slices were selected at the level of the motor cortex, PLIC, and CerPed, respectively. Mid-sagittal slices were selected at the level of the CC. A, The WM skeleton is shown in green with arrows labeling the CST, somatosensory cortex, parietal lobe, external capsule, PLIC, anterior limb of the internal capsule (ALIC), and corpus callosum. In the coronal view, ROIs for the SCR (red), PLIC (yellow), CerPed (blue), and sub-CerPed (orange) are shown. Significant differences between the CP and TDC groups are shown for FA (B), RD (C), AD (D), and MD (E). The hot colormaps denote whether a DTI measure for the CP group was less than (red-yellow) or greater than (blue-light blue) that in the TDC group. A indicates anterior; FWE, family-wise error; I, inferior; L, left; P, posterior; R, right; S, superior.
To further compare the CP and TDC groups, we calculated means for FA, RD, AD, and MD in each ROI. Data were tested for normal distribution using the Shapiro-Wilk test.21 Between-group differences were analyzed using t tests, assuming unequal variance (JMP Pro 14; SAS Institute). Corrections for multiple comparisons were made using the Benjamini-Hochberg false discovery rate.22
Significant correlations between DTI outcomes and clinical measures (SCALE and GMFM) within each ROI were quantified for the CP group by performing voxel counts in FSL (http://www.fmrib.ox.ac.uk/fsl). The percentages of significant voxels in relation to the total number of voxels within ROIs were calculated.
RESULTS
Twelve children with spastic bilateral CP (2 girls, 10 boys; mean age, 11.5 [SD, 2.8] years; age range, 7.3–16.6 years) participated. GMFCS levels were the following: I (n = 3), II (n = 1), III (n = 7), and IV (n = 1). Total SCALE scores ranged from 1 to 18. Twelve participants were recruited for the TDC group (12 boys; mean age, 10.3 [SD, 1.5] years; age range, 7.5–12.9 years).
Group Differences
The mean WM skeleton used for statistical comparisons of whole-brain WM voxels is shown in Fig 1A. The CP group showed significantly lower FA values throughout the whole brain compared with the TDC group (Fig 1B). These areas included the CST, somatosensory cortex, parietal lobe, optic radiation, anterior limb of the internal capsule, external capsule, and CC. Within the CST, FA was significantly lower in the CerPed, PLIC, and motor cortex, but no significant differences were found in the SCR. RD was higher for the CP group throughout the brain, but fewer differences were found anteriorly at the level of the CerPed compared with other regions (Fig 1C). Bidirectional results were seen for AD (Fig 1D), which was lower for the CP group at the level of the CerPed and cortex (coronal view) but higher for the CP group in the posterior end of the PLIC (axial view) and SCR bilaterally (coronal view). Fewer differences in AD were seen at the level of the motor cortex (right hemisphere) compared with other regions. MD was higher for the CP group within the CC, right CerPed, bilateral PLIC, SCR, and motor cortex (Fig 1E).
ROI analysis revealed significant differences between mean DTI outcomes of the CP and TDC groups within specific ROIs located along the CST and CC (Fig 2). Significantly lower FA values in the right sub-CerPed, CerPed bilaterally, and CC body and splenium were found for the CP group. In contrast, RD was significantly higher for the CP group in the CerPed bilaterally and CC body and splenium. AD was significantly lower for the CP group in the left CerPed and higher in the SCR bilaterally. MD was significantly higher for the CP group in the SCR bilaterally and CC body and splenium.

Mean differences in DTI measures between the CP and TDC groups within ROIs for the CST and CC. The asterisk indicates significant differences (P <.05). L indicates left; R, right.
Correlation Analyses
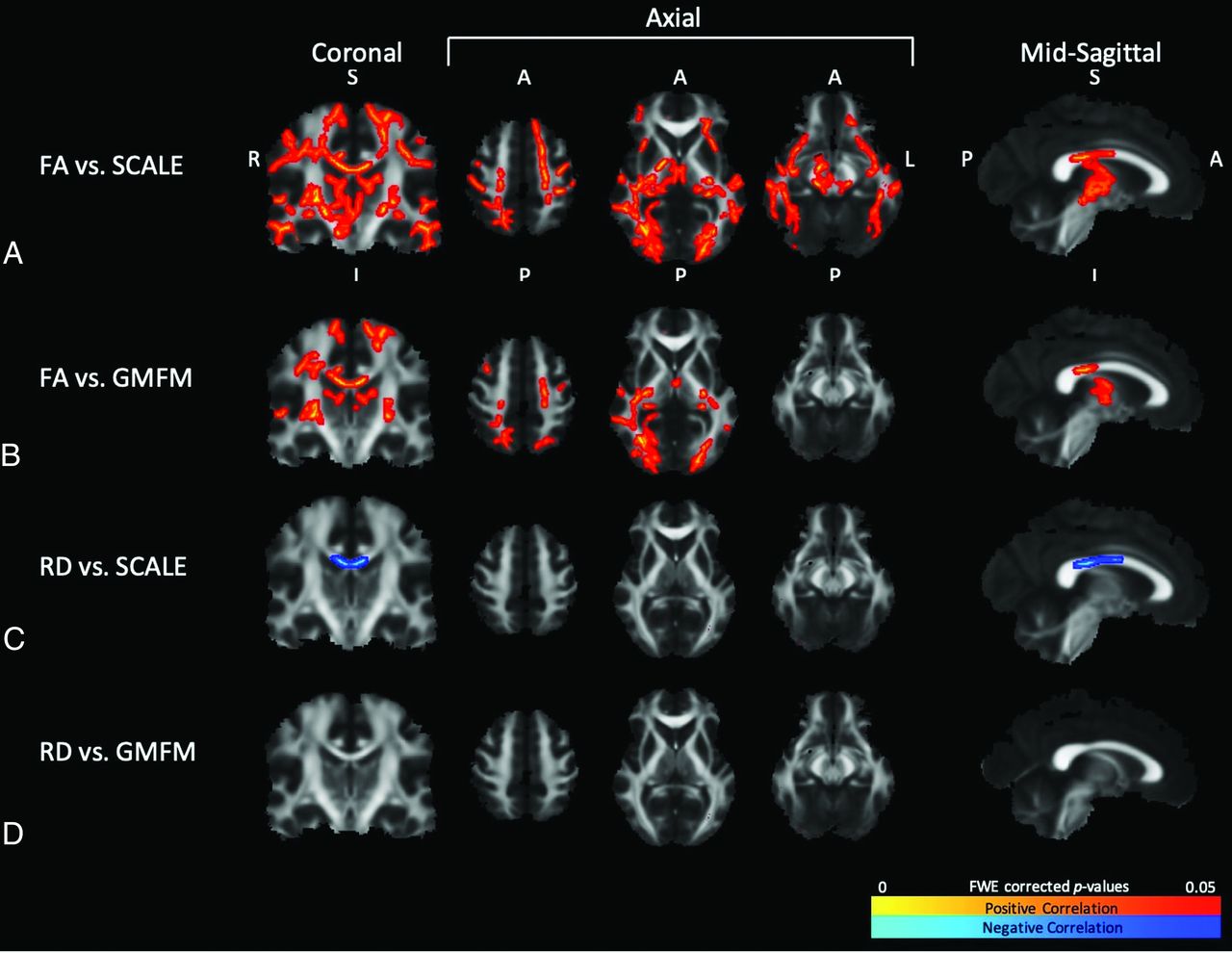
In the whole-brain correlation analyses for the CP group, significant correlations were found for FA and RD but not for AD and MD (Fig 3). Significant positive correlations were found between FA and SCALE for all slices shown in Fig 3A. These correlations were associated with motor function regions, including the CST at the level of the CerPed (right > left), PLIC (right > left), motor cortex (left > right), and CC. Fewer voxels within these motor regions exhibited significant positive correlations between FA and GMFM (Fig 3B). In the motor cortex, FA correlated with both SCALE and GMFM for bilateral lower extremity CST and left upper extremity CST as seen from the coronal views. More voxels showed significant correlations with SCALE than with GMFM in these regions. RD exhibited significant negative correlations with SCALE in the CC (Fig 3C), but significant correlations with GMFM were not found (Fig 3D).

TBSS results show significant correlations (P <.05) between DTI measures and clinical measures for the CP group. Coronal slices were selected at the level of the CST. From left to right, axial slices were selected at the level of the motor cortex, PLIC, and CerPed, respectively. Mid-sagittal slices were selected at the level of the CC. Significant correlations are shown for FA vs. SCALE (A), FA vs. GMFM (B), RD vs. SCALE (C), and RD vs. GMFM (D). The hot colormaps denote whether the correlations were positive (red-yellow) or negative (blue-light blue). A indicates anterior; FWE, family-wise error; I, inferior; L, left; P, posterior; R, right; S, superior.
Voxel counts of significant correlations between DTI outcomes and clinical measures within the CST and CC ROIs are shown in the Table. FA correlated positively with SCALE within the right sub-CerPed, CerPed (right > left), PLIC (right > left), SCR (right > left), and CC body and splenium. Compared to SCALE, fewer voxels showed significant positive correlations between FA and GMFM within the PLIC, SCR, CC body and splenium, and throughout the whole brain (30.4% versus 14.4%, respectively). No voxels showed significant correlations between FA and GMFM within the CerPed and sub-CerPed ROIs. RD correlated negatively with SCALE for voxels within all CC ROIs but not CST ROIs. No significant correlations between RD and GMFM were found in voxels for the CST and CC ROIs.
ROI correlation analyses comparing motor and whole-brain WM regions
DISCUSSION
This was the first study to associate SCALE, a sensitive measure of SVMC, with DTI outcomes for the CST and other WM tracts in children with spastic bilateral CP. We demonstrated that FA correlated with SCALE in key regions of the CST. A previous DTI study had reported that sensory but not motor tracts correlated with motor function using visual assessment of tract impairment.23 Motor function in that study, however, was measured using hand-held dynamometry, which is difficult to measure reliably in children with poor motor control.24 Additionally, the motor skill and ambulatory level were not well-defined. In our analysis, both SCALE and GMFM, which are valid clinical measures for spastic CP, were associated with CST impairment. SCALE emerged as the stronger clinical correlate using TBSS. To quantify the spatial differences, we performed voxel counts in 3D motor ROIs. In comparison with GMFM, the number of voxels with significant correlations between SCALE and FA and the number of voxels with significant correlations between SCALE and RD were greater, establishing SCALE as the more sensitive clinical correlate. Previous studies demonstrating a positive relationship between CST FA and functional ability were limited by their use of the GMFCS rating scale, which is a categoric descriptor of mobility.2,10 In contrast, SCALE and GMFM used in the present study are numeric measures of motor function.
Correlations of FA and RD with SCALE in the CC showed similar trends as reported by Arrigoni et al,10 in 2016, who reported correlations of FA and RD with GMFCS in the body of the CC. The significant negative correlations between RD and SCALE in the present study suggest that callosal fibers serving interhemispheric sensorimotor communication are better myelinated for children with greater SVMC.25 These findings may reflect one component of SCALE scoring procedures, the presence of mirroring, which lowers the score. Mirroring occurs when an intentional joint movement on one side of the body is accompanied by an obligatory synkinetic movement on the contralateral side.4 There are known associations between myelination of the CC and inhibition of mirroring.26⇓-28 Additionally, transcallosal motor fibers located in the CC body are believed to play an important role in motor control and inhibition of unwanted mirror movements,29 and lower FA in transcallosal motor fibers has been associated with mirroring in the hands of children with bilateral spastic CP and periventricular leukomalacia. The same mechanism likely occurs in lower extremity mirroring but has not been studied, to our knowledge.
Widespread correlations between SCALE and FA beyond the motor regions were found. In Fig 3, FA correlations with SCALE but not GMFM were seen in the brain stem, visual association pathways, and temporal lobes, suggesting that the integrity of these association pathways was more important for skilled, precise movements than for gross motor activities. Although a direct link between these regions and the ability to execute precise lower extremity movements is difficult to ascertain, such extensive correlations support prior studies demonstrating a relationship between motor function in spastic CP and long-range network connectivity disruptions of various nonmotor networks, including WM regions comprising the visual, limbic, and sensory systems.1,15 Additionally, lower SCALE scores may be associated with the overall severity of CP, including comorbidities of visual and cognitive impairments.
Consistent with previous studies, children with spastic bilateral CP had lower FA, higher RD, and higher MD in key regions of the CST, specifically the CerPed, PLIC, and motor cortex, compared with TDC.2,10 While periventricular leukomalacia is a hallmark of spastic CP, no significant between-group differences in FA were found in the periventricular WM. FA values in this region are affected by an abundance of crossing fibers beyond the CST, including the corticopontine, corticobulbar, and thalamocortical tracts, causing more variability in FA. This factor leads to overall reduced measurements of FA in this region and may contribute to the statistically nonsignificant group differences.1 In spastic CP, WM pathology extends beyond the periventricular WM.2,10 Accordingly, we found widespread higher RD for the CP group in the somatosensory cortex, parietal lobe, optic radiation, anterior limb of the internal capsule, external capsule, and CC. These higher RD values within the CST and throughout the whole brain are consistent with a lack of mature myelinated fibers and secondary Wallerian degeneration.3
Little is known about the relevance of AD differences between the spastic CP and TDC groups. In this analysis, mixed results were found for AD. Unexpectedly, AD was higher in the periventricular WM including the SCR for the CP cohort (Figs 1D and 2). This finding may be associated with the radial diffusion of crossing fibers running perpendicular to the ascending/descending tracts in this region.30 The interpretation of this result is not straightforward because the utility of AD as a putative marker of axonal degeneration or a precise descriptor of tissue microstructure is still under investigation.25,31
Statistically significant group differences observed in TBSS were not always reflected in ROI analyses (Figs 1 and 2). This issue can be attributed to the fact that ROI analyses smoothed data over large areas, reducing noise and the number of multiple comparisons. Notably, group-difference analyses in TBSS revealed brain-wide effects in the CP group, suggesting widespread microstructural tissue disruptions. Although motor tracts are deemed the region of injury in CP, WM pathways implicated in vision, hearing, sensation, proprioception, and cognition may be impacted.32 These findings are consistent with common comorbidities of spastic CP and may also suggest a global adaptation and neuroplasticity owing to recruitment of different brain regions postdamage.
These widespread differences in the CP group can also be understood in terms of network-connectivity disruptions. Englander et al,15 in 2013, showed changes to both short- and long-range brain network connectivity not limited to the sensorimotor network in severe-versus-moderate CP, though they did not include a healthy control sample. While we did not have a sufficient sample size to differentiate between severe and moderate cases of CP, our global voxelwise findings implicated similar WM regions including the visual, auditory, and cognitive systems. Ceschin et al,1 in 2015, found widespread voxelwise reductions of FA in CP and also showed disruption in network connectivity based on global topologic connectivity measures throughout the whole brain. Furthermore, they found alterations in the frontal-striatal and frontolimbic nodes, suggesting compensatory reorganization involving these frontal lobe pathways.1 Jiang et al,33,34 in 2019 and 2021, used DTI to show reduced global and nodal network efficiency and increased shortest-path length using the fiber count metrics in infants diagnosed with periventricular WM injury and spastic CP.33,34 Their study defined nodes as anatomic regions on the cortical gray matter and implicated impairment to the frontal, visual, and cingulate cortices in addition to the supplementary motor area, causing visual spatial or visual perception deficits.34
While our hypotheses targeted the CST and WM motor tracts in general, brain-wide WM group differences and brain-wide SCALE correlations suggest both a network-structure disruption effect and a network-region recruitment effort by long-range brain fibers that may serve in a compensatory capacity in response to periventricular leukomalacia injury. Zhou et al,35 in 2017, suggested the theory of “imperfect compensation,” whereby the red nucleus and rubrospinal tract, which are normally inhibited in early life in TDC, further develop to provide compensatory motor control (flexor and extensor synergy patterns) in cases of motor tract injury. While higher FA relative to controls has been reported in the rubrospinal system of adults following stroke,36,37 higher FA for the CP group in the present study was not found in any WM region. The development of new network-driven hypotheses targeting brain connectivity and compensatory mechanisms in response to perinatal brain injury should be explored.
The study was limited by a small sample size because we could include only participants who could cooperate with MR imaging without sedation. ROI analyses at the level of the primary motor cortex could not be performed because this region was not included in predefined segmentations of the Johns Hopkins University WM atlas labels.
CONCLUSIONS
This study establishes SCALE as a clinical correlate of multiple DTI measures. SCALE was sensitive to WM impairment within the CST and CC and throughout the whole brain. This study supports FA and RD as strong indicators of WM motor injury. It confirmed that children with spastic bilateral CP have altered WM diffusion properties throughout the whole brain, including the CST. Responsiveness to intervention using DTI measures is an important area for future research in CP.
Acknowledgments
We would like to thank the children and their families for participating in this study, in addition to Dr. Erica Hsu, Mr. Kylen Soriano, and Mr. Vinh Nguyen for their assistance with data processing and analysis.
Footnotes
MR imaging data acquisition and gait assessments were funded by donations and grants from the UCLA Children’s Discovery and Innovation Institute; Shapiro Family Foundation; United Cerebral Palsy of Los Angeles, Santa Barbara and Ventura Counties; Waters Foundation; California Community Foundation; Lena Longo Foundation; and UCLA Brain Mapping Center. No funders were involved in the preparation of this article.
Paper previously presented, in part, at: Annual Meeting of the American Academy for Cerebral Palsy and Developmental Medicine, September 18–21, 2019; Anaheim, California.
Disclosures: Eileen G. Fowler—RELATED: Grant: UCLA Children’s Discovery and Innovation Institute, Comments: This internal university grant provided funding for the MR images. Also, our institution received donations from individuals that supported salaries.* Joyce Matsumoto—RELATED: Grant: UCLA Children’s Discovery and Innovation Institute, Comments: Grant awarded to fund research MR images.* *Money paid to the institution.
References
- Received March 22, 2021.
- Accepted after revision June 23, 2021.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Improved Myelination following Camp Leg Power, a Selective Motor Control Intervention for Children with Spastic Bilateral Cerebral Palsy: A Diffusion Tensor MRI Study
- Improved Myelination following Camp Leg Power, a Selective Motor Control Intervention for Children with Spastic Bilateral Cerebral Palsy: A Diffusion Tensor MRI Study