
Abstract
BACKGROUND AND PURPOSE: In patients with Moyamoya disease, the relationship between preoperative hemodynamic status and prognosis after encephalo-duro-arterial synangiosis (EDAS) surgery was unclear. We aimed to explore the value of the preoperative hemodynamic status acquired by cine phase-contrast MR imaging in predicting collateral formation and clinical outcomes after EDAS surgery in patients with Moyamoya disease.
MATERIALS AND METHODS: Participants with Moyamoya disease were prospectively recruited and underwent preoperative phase-contrast MR imaging. All participants were classified into good and poor groups according to the collateral formation after EDAS surgery. On the basis of the change in the mRS system, participants were classified into the improved mRS group and the poor response group. Hemodynamic status including mean velocity, peak velocity, and blood volume flow of the superficial temporal artery was compared between groups. Logistic regression was performed to relate the phase-contrast MR imaging parameters to collateral formation and clinical outcomes.
RESULTS: A total of 45 patients with Moyamoya disease with unilateral EDAS surgery were finally included. Mean velocity, peak velocity, and blood volume flow of the ipsilateral superficial temporal artery were significantly greater in patients with good collateral formation compared with those with poor collateral formation (P = .011, .004, and .013, respectively). The mean velocity, peak velocity, and blood volume flow were independently associated with postoperative collateral formation after adjusting for confounding factors. Furthermore, the peak velocity of the ipsilateral superficial temporal artery was also significantly associated with improvement of the mRS score.
CONCLUSIONS: Good hemodynamic status of the ipsilateral superficial temporal artery as a donor artery evaluated by phase-contrast MR imaging was significantly associated with better collateral formation and improved mRS after EDAS surgery in patients with Moyamoya disease.
ABBREVIATIONS:
- BVF
- blood volume flow
- EDAS
- encephalo-duro-arterial synangiosis
- MMA
- middle meningeal artery
- MMD
- Moyamoya disease
- PC-MRI
- phase-contrast MRI
- rCBF
- relative CBF
- rCBV
- relative CBV
- rTTP
- relative TTP
- STA
- superficial temporal artery
- Vmean
- mean velocity
- Vpeak
- peak velocity
Moyamoya disease (MMD) is a type of cerebrovascular disease characterized by progressive stenosis and even occlusive changes in the bilateral terminal part of the ICA and the middle and anterior cerebral arteries.1,2 Encephalo-duro-arterial synangiosis (EDAS) is one of the most commonly used indirect surgical procedures.3⇓-5 It reroutes a branch of the external carotid artery to the surface of the brain and relies on neovascularization via angiogenic mechanisms from pedicle-based grafts. Generally, the superficial temporal artery (STA) and its branches are the donor arteries. Therefore, identification of information about the STA as a donor artery may be beneficial in the prediction of surgical prognosis.
Previous studies proved that an increased caliber of the STA was associated with good prognosis of EDAS surgery.6,7 However, morphologic features of the STA could provide only indirect information. Functional characteristics, in particular the hemodynamic status, might provide more direct information about the role of the STA as the donor artery. To date, the relationship between the preoperative hemodynamic status of the STA and clinical outcome after surgery was unknown.
Phase-contrast MR imaging (PC-MR imaging) is a nonradioactive detection method for quantitatively analyzing the hemodynamic status of targeted vessels. The reliability and reproducibility of PC-MR imaging have been validated by several studies.8,9 PC-MR imaging has been performed in patients with MMD in several studies and could provide similar quantitative data of the targeted vessels.10⇓-12 Therefore, we hypothesized that the preoperative hemodynamic status of the STA is closely related to the development of collateral vasculature and the change of symptoms after the operation, aiming to explore the relationship between the hemodynamic status of the STA and postoperative outcomes in patients with MMD using PC-MR imaging.
MATERIALS AND METHODS
Study Population
This prospective study was approved by the institutional review board of Chinese PLA General Hospital. All participants provided written informed consent to participate in the study. From October 2020 to November 2021, consecutive participants who underwent their first EDAS surgery were recruited. Previously, PC-MR imaging examinations were performed in participants within 1 week before the operation. From the 59 participants, 14 were excluded for the following reasons: 1) poor image quality of the postoperative DSA or PC-MR imaging (n = 3); and 2) unavailable postoperative DSA (n = 11). Finally, 45 participants were recruited.
MR Imaging Examination
All participants underwent MR imaging examinations using a 3T whole-body MR imaging scanner (Magnetom Skyra; Siemens) with a head-neck coil. All participants were instructed to remain still during the examination.
The parameters of PC-MR images were as follows: TR = 20.36 ms; TE = 2.8 ms; section thickness = 5 mm; number of slices = 20; FOV = 233 × 340 mm; matrix = 176 × 256; flip angle = 20°; number of acquisitions = 3. Reconstructed MIP images of TOF, obtained previously, were used to position the PC-MR imaging sequence. The scan planes were placed where the targeted vessels were straight and perpendicular to the vessels on the basis of the coronal and sagittal projection images. Because the velocity of the vessels varied from one patient to another, prescans were performed to acquire the best velocity-encoding (the brightest sequence without any regurgitation). The prescan velocity-encoding of the STA was 15∼45 cm/s.
The parameters of DSC images were as follows: TR = 1360 ms; TE = 30 ms; section thickness = 5 mm; number of slices = 20; FOV read = 229 mm; matrix = 144 × 144; flip angle = 90°; number of acquisitions = 60. Gadolinium contrast medium (Magnevist; Bayer HealthCare Pharmaceuticals) was intravenously injected using a high-pressure injector (Medrad Spectris Solaris EP MR injection system; Bayer HealthCare) at the fifth acquisition (0.2 mL/kg, 4.5–5 mL/s) and followed immediately by a 30-mL physiologic saline flush.
Surgical Treatment
There is a standard procedure for the EDAS in our institution that is similar to that described previously in the literature.13 Generally, the STA and accompanying cuff of the galea connective tissue were exposed and then covered and sutured onto the surface of brain.
Angiography
All participants underwent DSA (Allura Xper FD20 angio system; Philips Healthcare) >3 months after the operation because the development of donor arteries was observed 3 months after indirect surgery.14 As selective catheterization and intra-arterial injection of nonionic monomeric iodine contrast medium were performed, anterior-posterior and lateral projection images of the bilateral ICAs, external carotid arteries, and dominant-side vertebral artery were obtained.
Data Analysis
MR Imaging Examination.
Images of PC-MR imaging and DSC were transmitted to the syngo via (Siemens) postprocessing workstation. Hemodynamic information acquired by PC-MR imaging was obtained by drawing ROIs on the phase images, which contained the lumen of the vessel as much as possible without exceeding the vessel contour. To determine the boundary of the STA, the window width of magnitude images could be narrowed and the junction of hyperintensity (signal of blood flow) and isointensity (signal of soft tissue) was the boundary of the STA. Measurements of mean velocity (Vmean), peak velocity (Vpeak), and blood volume flow (BVF) of the bilateral STA were performed and documented by 2 of the authors (H. Zhang and S. Liu), who had >5 years’ experience and were blinded to the clinical symptoms.
DSC data were analyzed by MR perfusion software. Maps of DSC were generated using the local arterial input function mode. ROIs were manually drawn at the lateral MCA territories and cerebellum. The great cerebral vessels and ischemic or hemorrhage lesions were avoided. Relative TTP (rTTP) was calculated by subtracting the value of the MCA territories from the value of the cerebellum. Relative CBF (rCBF) and CBV (rCBV) were calculated by dividing the value of the MCA territories by the value of the cerebellum.15
DSA Examination.
DSA data were independently evaluated by 2 neuroradiologists (H. Zhang and S. Liu) who were blinded to the radiologic findings. We modified the classification proposed by Matsushima et al,16 and collateral formation after surgery was divided into 4 grades, which included grade III, in which the area supplied by the surgical bypass covered more than two-thirds of the MCA distribution; grade II, in which between two-thirds and one-third of the MCA distribution was covered; grade I, in which less than one-third of the cortical branch of the MCA was covered; and grade 0, in which no collateral circulation was covered. Grades II and III were regarded as good collateral formation, and the others were poor collateral formation. In addition, morphologic features of the ipsilateral STA, which included straightness of the bilateral STA and location of the bifurcation, were also evaluated. The STA with no more than 3 turns was regarded as straight. The high bifurcation position defined as the STA trunk accounted for more than half of the full length of the STA. Furthermore, the diameters of the bilateral middle meningeal artery (MMA) after EDAS surgery were measured on DSA images.
Clinical Follow-up.
On the basis of the mRS system, preoperative and postoperative symptoms of patients were evaluated. Postoperative mRS was evaluated at the time of DSA examinations, which were performed at least 3 months after the operation. Participants were assigned to the improved group if their mRS scores improved by at least 1 grade. Patients with no change or worsening of symptoms after EDAS surgery were classified in the poor response group.
Statistical Analysis
Continuous variables were documented as mean (SD). Categoric variables were presented as frequencies. The independent Student t test was used if the continuous data adhered to a normal distribution and variance homogeneity. The Mann-Whitney U test was used to compare the difference in the Suzuki stage between the 2 groups. Categoric data were compared using the χ2 test. The sensitivity, specificity, and cutoff values were calculated, respectively. Univariate and multivariable logistic regression models were used to calculate the OR and the corresponding 95% CI of PC-MR imaging in discriminating the collateral foundation and mRS. Interreader and intrareader reliability were determined via intraclass correlation coefficients and 95% CIs or κ values. Results with P < .05 were regarded as statistically significant. SPSS 23.0 software (Version 23.0; IBM) was used for statistical analysis.
RESULTS
Patient Characteristics
Among the 45 participants (23 women and 22 men; mean age, 33.89 [SD, 18.04] years), 17 had hypertension (38%), 20 had hyperlipidemia (44%), 5 had diabetes (11%), and 1 (2%) had coronary heart disease. Three (7%) participants had a history of smoking, and the posterior cerebral arteries in 6 (13%) participants were involved. The average time interval from EDAS surgery to the postoperative DSA examination was 7.41 (SD, 1.81) months. The number of participants in Suzuki stages I–II, III–IV, and V–VI was 6 (13%), 30 (67%), and 9 (20%), respectively.
On the basis of the neoangiogenesis after revascularization, 23 participants (grade II revascularization, n = 22; grade III, n = 1) were observed to have good collateral formation on DSA during follow-up and 22 (grade 0, n = 3; grade I, n = 19) had poor collateral formation. Preoperative perfusion status including rTTP, rCBF, and rCBV in the ipsilateral hemispheres with good collateral formation was significantly worse than that in those with poor collateral formation (all, P value < .05; Table 1). No statistically significant difference was found in other clinical features between the participants with good and poor collateral formation (Tables 1 and 2; Figs 1 and 2).
Demographic and clinical characteristics
Comparison of measurements of the STA between participants with good and poor collateral formation

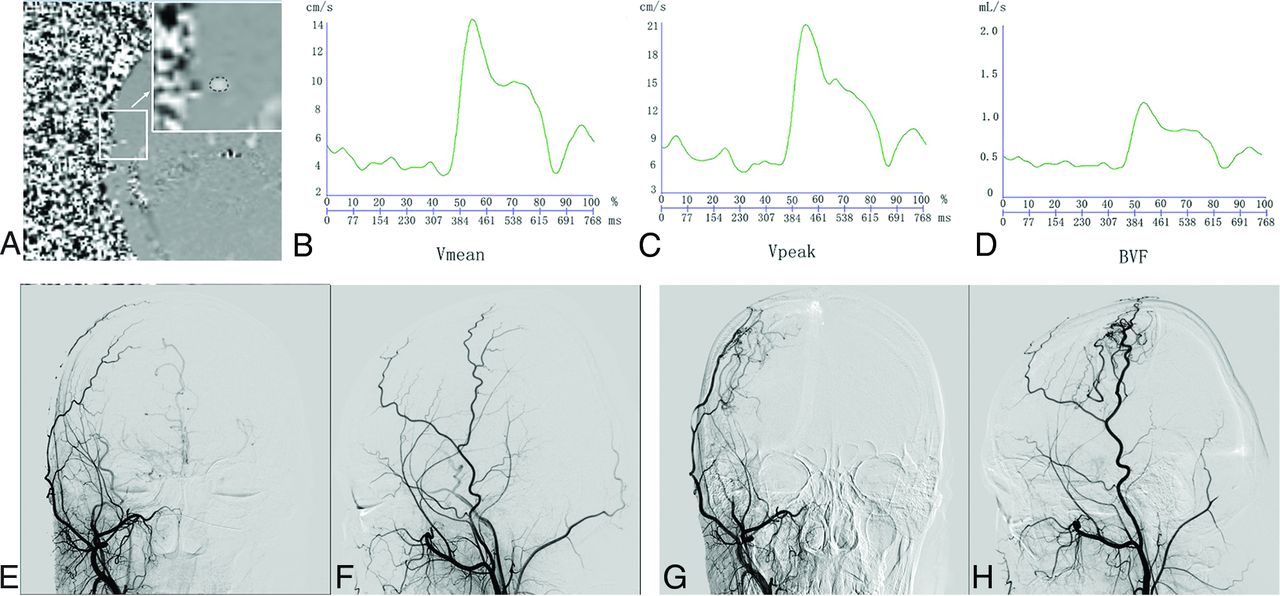
PC-MR imaging and DSA examination in a patient with good collateral formation. Images in a female patient diagnosed with MMD who had right EDAS surgery. She underwent PC-MRI and DSA before and 6 months after the operation. A, Phase image shows the ROI of the right STA. A, the arrow represents the enlarged view of the small white square. Modulation of the Vmean (B), Vpeak (C), and BVF (D) of the right STA acquired by PC-MRI. Anterior-posterior and lateral projections of preoperative (E and F) and postoperative (G and H) DSAs of the right external carotid artery show large areas of revascularization (more than one-third but less than two-thirds of MCA territory).

PC-MR imaging and DSA examination in a patient with poor collateral formation. Images in a male patient diagnosed with MMD who had right EDAS surgery. He underwent PC-MRI and DSA before and 7 months after the operation. A, Phase image shows the ROI of the right STA. A, the arrow represents the enlarged view of the small white square. Modulation of Vmean (B), Vpeak (C), and BVF (D) of the right STA acquired by PC-MRI. Anterior-posterior and lateral projections of preoperative (E and F) and postoperative (G and H) DSAs of right external carotid artery show small areas of revascularization (less than one-third of the MCA territory).
Association of Hemodynamic Features of STA and Postoperative Collateral Formation
The Vmean (6.69 [SD, 2.02] cm/s versus 5.30 [SD, 1.41] cm/s, P = .011), mean Vpeak (22.62 [SD, 5.79] cm/s versus 17.00 [SD, 6.62] cm/s, P = .004), and mean BVF (0.70 [SD, 0.32] mL/s versus 0.50 [SD, 0.17] mL/s, P = .013) of the ipsilateral STA in participants with good collateral formation were significantly greater compared with those with poor collateral formation (Table 2 and Fig 3A).

Comparison of PC-MR imaging parameters between patients with good and poor collateral formation (A) and between patients with improved mRS and poor response (B). The asterisk indicates P < .05.
When the Vmean = 6.020 cm/s was taken as the cutoff value, the sensitivity and specificity of Vmean in predicting good collateral formation were 0.696 and 0.727, respectively. The sensitivity and specificity of Vpeak in predicting good collateral formation were 0.826 and 0.591, respectively, when Vpeak = 18.315 cm/s was taken as the cutoff value. Moreover, the cutoff value of BVF was 0.585 mL/s with a sensitivity of 0.652 and specificity of 0.818.
Univariate logistic analysis showed that greater Vmean (OR = 1.66; 95% CI, 1.08–2.53; P = .020), Vpeak (OR = 1.16; 95% CI, 1.04–1.30; P = .009), and BVF (OR = 1.04; 95% CI, 1.01–1.07; P = .024) of the ipsilateral STA were significantly associated with good collateral formation. Multivariate logistic analysis showed that the association of greater Vmean (OR = 2.28; 95% CI, 1.23–4.25; P = .009), Vpeak (OR = 1.18; 95% CI, 1.04–1.34; P = .010), and BVF (OR = 1.73; 95% CI, 1.02–2.94; P = .043) of the ipsilateral STA and good collateral formation remained statistically significant after adjustment of patients’ clinical characteristics (age, sex, hypertension, hyperlipidemia, diabetes, smoking, and the interval from the operation to the latest DSA examination), morphologic features of the ipsilateral STA (cross-sectional area, straightness, and high bifurcation position of STA), preoperative perfusion status (rCBV), and diameter of the ipsilateral MMA after EDAS (Table 3).
Association of hemodynamic status of the ipsilateral STA and collateral formation using logistic regression analysisa
Association of Hemodynamic Information and Change of mRS
The mean Vpeak (22.13 [SD, 6.59] cm/s versus 17.30 [SD, 6.13] cm/s, P = .015) of the ipsilateral STA in participants with an improved mRS was significantly greater compared with those with a poor response (Table 4 and Fig 3B).
Comparison of PC-MR imaging of STA between participants with improved mRS and those with poor response
Univariate logistic analysis showed that greater Vpeak (OR = 1.13; 95% CI, 1.02–1.26; P = .022) of the ipsilateral STA was significantly associated with improved mRS scores. Multivariate logistic analysis showed that the association of greater Vpeak (OR = 1.18; 95% CI, 1.03–1.34; P = .014) of the ipsilateral STA and improved mRS remained statistically significant after adjustment of participants’ clinical characteristics (age, sex, hypertension, hyperlipidemia, diabetes, smoking, and the interval from the operation to latest DSA examination), morphologic features of ipsilateral STA (cross-sectional area, straightness, and high bifurcation position of the STA), preoperative rCBV, and diameter of the ipsilateral MMA.
Interaction of Age, Sex, and Preoperative rCBV
In predicting the collateral formation, no interactive effect was found between age and sex or between age and preoperative rCBV or between sex and preoperative rCBV (Table 5).
Interactive effects of age, sex, and rCBV on collateral formation
Reproducibility
κ values for the intrareader agreement in measurement of Vmean, Vpeak, and BVF were 0.83, 0.92 and 0.85, respectively. For interreader agreement, the κ values were 0.80, 0.91, and 0.77 in the measurement of Vmean, Vpeak, and BVF. The intrareader agreement in evaluating collateral formation was 0.82.
DISCUSSION
To our knowledge, this is the first study investigating the relationship between the preoperative hemodynamic status of the ipsilateral STA as a donor artery and the postoperative outcomes of patients with MMD using PC-MR imaging. We found that patients with greater Vmean, Vpeak, and BVF of the ipsilateral STA were more likely to have better postoperative collateral formation. Furthermore, Vpeak of the ipsilateral STA was associated with improvement of symptoms. Our results suggest that good hemodynamic status of ipsilateral STA may serve as a predictor of favorable outcome in patients with MMD after EDAS surgery.
The PC-MR imaging technique has been widely used in quantitatively analyzing vascular diseases and evaluating hemodynamic status.17,18 The hemodynamic characteristics of intracranial vessels in patients with MMD have been evaluated in previous studies using PC-MR imaging, and most of them explored the hemodynamic change of the anterior and posterior circulation before and after the operation.10,11,19 However, few studies focused on the hemodynamic status of the STA. EDAS, as one of the most commonly used indirect surgical procedures in MMD, mostly adopted STA and its branches as donor arteries. Therefore, the hemodynamic features of the STA before the operation may be more significantly associated with the postoperative outcomes compared with those of the ICA and the posterior cerebral artery. In the present study, we used PC-MR imaging to assess the velocity and BVF of the STA and found an excellent reliability in the measurements of these hemodynamic parameters.
EDAS surgery reroutes branches of the external carotid artery such as the STA to the surface of the brain. With the development of collateral circulation, blood flow is diverted from the external carotid artery to the blood supply area of the ICA. Therefore, abundant blood flow in the STA enables the formation of collateral circulation after EDAS surgery. The mechanism by which the good hemodynamic status of the STA may promote the development of collateral circulation may be as follows: 1) The greater blood volume flow of the STA may provide sufficient blood supply for collateral formation, and 2) the higher flow velocity of the STA may indicate better vasoreactivity and function status as a donor artery, which can enable richer neovascularization after EDAS. In this study, we found that there were no significant differences in the morphologic features of the ipsilateral STA, which included caliber, straightness, and high bifurcation position, between patients with good and poor collateral formation. This finding may be because morphologic information about the STA could not directly reflect the hemodynamic status. Therefore, morphologic features of the ipsilateral STA alone could not be used to predict the prognosis of EDAS surgery.
In the present study, we found that the greater Vmean, Vpeak, and BVF of the ipsilateral STA were significantly associated with good collateral formation after EDAS surgery. The cutoff values of Vmean, Vpeak, and BVF were 6.020 cm/s, 18.315 cm/s, and 0.585 mL/s, respectively. Furthermore, no statistically interactive effect was found among clinical factors (age, sex and preoperative rCBV) in predicting collateral formation. A previous study showed that the blood flow velocity of the STA as the bypass artery could be used to predict the postoperative outcomes in the direct revascularization surgery using sonography.20 Similar to the conclusion of the sonographic study, we found that good hemodynamic status was also associated with a favorable outcome after EDAS surgery, which is an indirect revascularization surgery mostly using the STA as a donor artery. Thus, we recommend that for patients with MMD, PC-MR imaging could be regarded as a supplementary examination to predict collateral formation after EDAS surgery.
Our results showed greater Vpeak of the ipsilateral STA closely related to the improved mRS scores after the operation, suggesting that better hemodynamic status of the ipsilateral STA may serve as a predictor of clinical outcomes in patients with MMD. As discussed above, the ipsilateral STA with better hemodynamic status correlated with more abundant collateral circulation formation, which could provide sufficient blood flow. Therefore, this result ameliorated the ischemic status of the hemispheres, and better mRS scores were obtained. In addition, Gao et al12 found that patients with poor hemodynamic status of the ipsilateral STA were more likely to develop cerebral hyperfusion syndrome, which could result in lower mRS scores.
This study had several limitations. First, the sample size of the study is limited, and further investigations with larger sample sizes are warranted. Second, in the present study, 2D-PC-MR imaging was used to assess the hemodynamic features. Recently, 3D-PC-MR imaging has been increasingly used in the evaluation of vascular diseases, which could be more time-saving and provide more information. Third, the present study included only patients with MMD who had undergone unilateral EDAS surgery; therefore, the prognosis of those who underwent bilateral surgery should be further investigated using PC-MR imaging. Fourth, the hemodynamic status of the MMA and the accessory meningeal artery before and after EDAS surgery was not included.
CONCLUSIONS
The good hemodynamic status of the ipsilateral STA as a donor artery evaluated by PC-MR imaging was significantly associated with better collateral formation and improved mRS after EDAS surgery in patients with MMD. Our results suggest that PC-MR imaging could provide valuable information on the prediction of clinical outcomes in patients with MMD after EDAS surgery.
Footnotes
Shitong Liu and Mingming Lu are co-first authors and contributed equally to this article.
Jianming Cai and Hongtao Zhang are co-senior authors and contributed equally to this article.
This study was supported by the grants of National Natural Science Foundation of China (82001774), Beijing Natural Science Foundation (7212100), Tianjin Science and Technology Project (TJWJ2021MS043), and Beijing Science and Technology Project (Z161100000516194).
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received May 2, 2022.
- Accepted after revision August 12, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.