
Abstract
BACKGROUND AND PURPOSE: In patients with ischemic stroke, DWI lesions can occasionally be reversed by reperfusion therapy. This study aimed to ascertain the relationship between ADC levels and DWI reversal in patients with acute ischemic stroke who underwent recanalization treatment.
MATERIALS AND METHODS: We conducted a retrospective cohort study in patients with acute ischemic stroke who underwent endovascular mechanical thrombectomy with successful recanalization between April 2017 and March 2021. DWI reversal was assessed through follow-up MR imaging approximately 24 hours after treatment.
RESULTS: In total, 118 patients were included. DWI reversal was confirmed in 42 patients. The ADC level in patients with reversal was significantly higher than that in patients without reversal. Eighty-three percent of patients with DWI reversal areas had mean ADC levels of ≥520 × 10−6 mm2/s, and 71% of patients without DWI reversal areas had mean ADC levels of <520 × 10−6 mm2/s. The mean ADC threshold was 520 × 10−6 mm2/s with a sensitivity and specificity of 71% and 83%, respectively. In multivariate analysis, the mean ADC level (OR, 1.023; 95% CI, 1.013–1.033; P < .0001) was independently associated with DWI reversal. Patients with DWI reversal areas had earlier neurologic improvement (NIHSS at 7 days) than patients without reversal areas (P < .0001).
CONCLUSIONS: In acute ischemic stroke, the ADC value is independently associated with DWI reversal. Lesions with a mean ADC of ≥520 × 10−6 mm2/s are salvageable by mechanical thrombectomy, and DWI reversal areas regain neurologic function. The ADC value is easily assessed and is a useful tool to predict viable lesions.
ABBREVIATIONS:
- IQR
- interquartile range
- MT
- mechanical thrombectomy
In acute ischemic stroke, DWI lesions are considered markers of irreversible ischemia but can occasionally be reversed. Defining the irreversible infarct core is crucial in assessing the risks and benefits of mechanical thrombectomy (MT) in acute ischemic stroke. Various MR imaging methods for selecting patients with ischemic salvageable regions for reperfusion therapies have been reported.1⇓-3 In these reports, DWI lesions were considered the infarct core; however, there have also been several studies on DWI lesion reversal through reperfusion therapy.4⇓-6
The ADC is a measure of the diffusivity of water molecules in tissues. In ischemic tissues, cytotoxic edema leads to a reduction in the ADC. Severe reduction of the ADC is associated with metabolic energy failure, which subsequently results in an infarct core.7,8 Given the DWI lesion reversal, mild ADC reduction could be reversed to normal ADC levels with early reperfusion.6,9 Such findings suggest that mild ADC reduction before metabolic energy failure is still reversible by reperfusion therapy.
We hypothesized that an ADC threshold that preserves the viability by reperfusion therapy exists in DWI lesions, explaining the concept of DWI reversal and neurologic improvement. Thus, in this study, we aimed to investigate the association between the ADC level and DWI reversal in patients with acute ischemia due to large-vessel occlusion recanalized by endovascular MT.
MATERIALS AND METHODS
Study Design and Patient Selection
This was a retrospective cohort study of patients with acute ischemic stroke who underwent endovascular MT between April 2017 and March 2021. The study protocol was approved by the institutional review board of our hospital. The requirement for written informed consent was waived due to the retrospective nature of the study. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Patients diagnosed with acute cerebral infarction were treated with intravenous tPA (0.6 mg/kg) within 4.5 hours of stroke onset and/or MT within 24 hours of onset. Follow-up MR imaging was performed 23–27 hours after MT to evaluate the status of the DWI lesion and recanalized artery.
The inclusion criteria were as follows: 1) diagnosis of symptomatic ischemic stroke; 2) anterior circulation occlusion (ICA, M1, M2, M3); 3) initial and follow-up MR imaging performed; and 4) successful recanalization by MT. The occlusion location was selected on the basis of the most proximal occluded segment on MRA. The degree of vessel occlusion at presentation and after treatment was defined using the modified TICI classification.10 In this study, successful recanalization was defined as TICI ≥ 2b. Stroke onset time was defined as the onset of symptoms or when a patient was last seen well if the onset was unknown. Recanalization time was defined as the time when the occluded artery reached TICI ≥ 2b. Patients whose conditions worsened due to other health problems or who lacked follow-up MR imaging data because of severe stroke or intracranial hemorrhage were excluded.
We collected the following information from medical records: age, sex, prestroke mRS score, initial NIHSS score, risk factors (hypertension, diabetes mellitus, hyperlipidemia, current smoking status, prior strokes), stroke subtype, occluded artery, emergency treatment (MT or tPA + MT), ASPECTS-DWI,11 stroke onset to imaging time, imaging to recanalization time, stroke onset to recanalization time, FLAIR lesions, and ADC values (mean, maximum, and minimum) in DWI lesions. The study end point was the mRS score 3 months after stroke.
MR Imaging Protocol
Initial and follow-up MR imaging was performed with a 3T scanner (Ingenia 3T CX; Philips Healthcare). The MR imaging protocol included DWI/ADC, T2*, FLAIR, and intracranial MRA. ADC maps were created for all patients. DWI was performed with single-shot spin-echo diffusion EPI with the following parameters: 220-mm FOV, twenty-seven 4-mm axial sections with a 1.0-mm gap, and a b-value of 1000 s/mm2 along 3 orthogonal directions.
Measurement of ADC and DWI Volume
DWI reversal was evaluated by comparing the initial and 23- to 27-hour posttreatment MR images and was defined as regional ADC normalization at the follow-up.6 The DWI lesion volume was represented as 11 minus the ASPECTS-DWI11 score at the initial and follow-up MR imaging. DWI reversal volume was calculated by subtracting the follow-up DWI scores from the initial scores. In cases with DWI reversal, the mean, maximum, and minimum ADC values in the reversal area were measured on the initial MR image. These parameters were obtained from 6- to 10-mm circular ROIs placed in them, excluding the cortex and CSF, in each of 11 areas of DWI lesions using the ASPECTS-DWI method, and the average was calculated (Fig 1). Cases without a reversal area were similarly evaluated (Online Supplemental Data). The ADC values of DWI lesions with reversal were similarly evaluated (Fig 1) and compared with the ADC values without reversal in the same cases.

Lesions with DWI reversal assessed by MR imaging DWI/ADC, DWI, ADC, and MRA images show a subtotal reversal of the left frontal ischemic lesion 24 hours after MT for M1 occlusion. The ADC values (mean, maximum, minimum) with reversal are measured in the ROIs (white circled area with a continuous line) in the pretreatment MR imaging, and each parameter is averaged. The ADC values (mean, maximum, minimum) without reversal are measured in the ROI (white circled area with a dotted line) at the pretreatment MR imaging. The ADC values of lesions with DWI reversal (mean, maximum, minimum) are 525 × 10−6 mm2/s, 748 × 10−6 mm2/s, and 368 × 10−6 mm2/s, respectively. The ADC values of lesions without DWI reversal (mean, maximum, minimum) are 434 × 10−6 mm2/s, 560 × 10−6 mm2/s, and 311 × 10−6 mm2/s, respectively.
Image analysis was performed by 2 neurologists (T.U. and T.M.) with at least 10 years of experience in assessing acute ischemic stroke with MR imaging. Both readers were blinded to all clinical and patient information. DWI reversal was determined by consensus, and interrater agreement was evaluated (κ = 0.92).
Statistical Analysis
Statistical analyses were performed using GraphPad Prism, Version 7 (GraphPad Software). Categoric variables are expressed as frequencies and percentages, whereas continuous variables are expressed as means (SD) or medians (interquartile range [IQR]). Baseline characteristics were compared between groups on the basis of the presence or absence of DWI reversal using the χ2 test for categoric variables or the Mann–Whitney U test for continuous variables. Logistic regression analysis was performed using JMP (SAS). The level of statistical significance was set at P < .05.
RESULTS
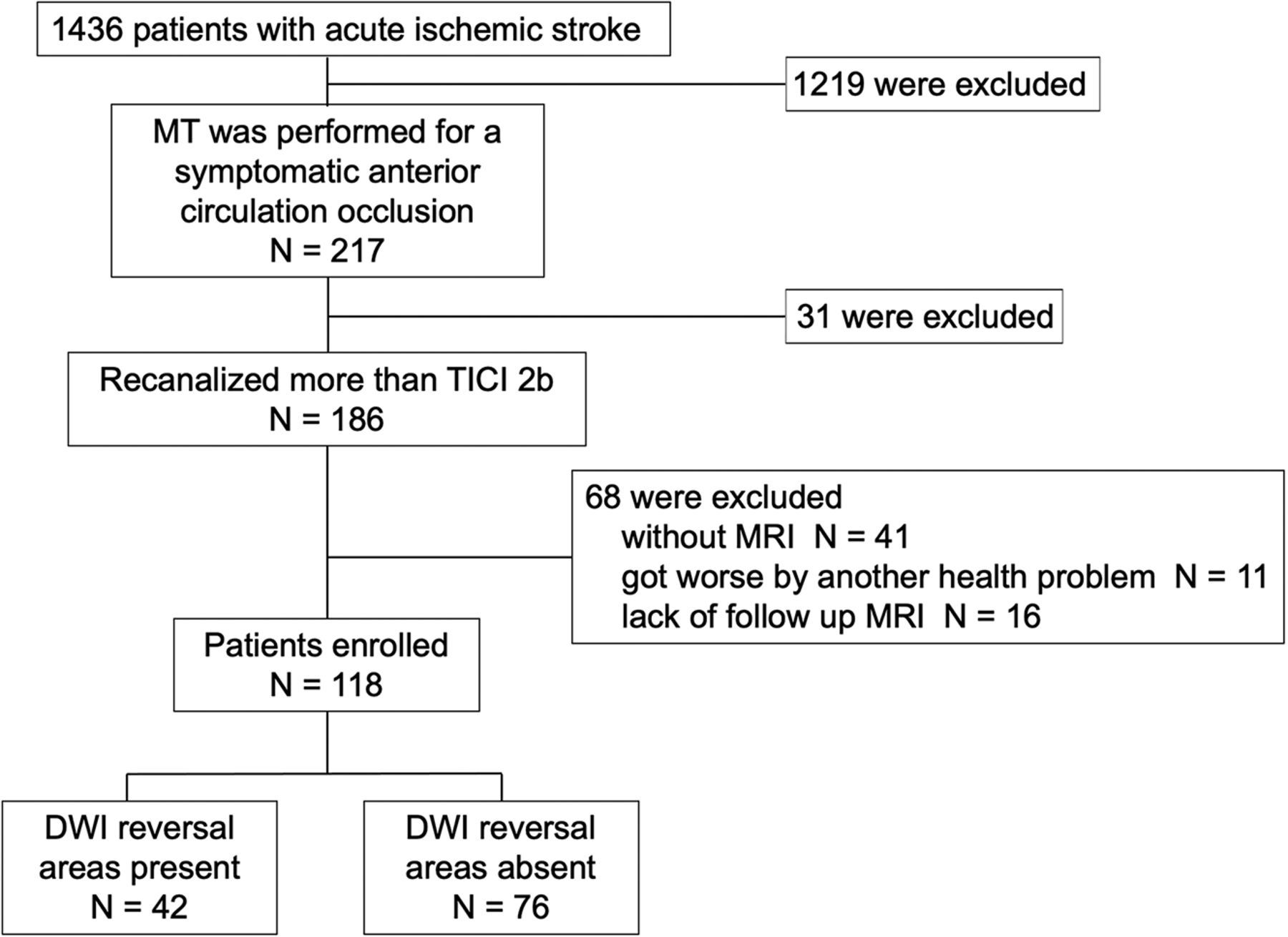
The study included 1436 consecutive patients admitted to our hospital with acute ischemic stroke between April 2017 and March 2021. Among them, MT was performed on 217 patients with symptomatic anterior large-vessel occlusion, and recanalization (TICI ≥ 2b) was achieved in 186 (86%) patients. Of these 186 patients, those who did not undergo MR imaging due to a cardiac pacemaker or other reasons (n = 41), those whose conditions worsened due to other health problems (n = 11), and those who did not undergo follow-up MR imaging because of severe stroke conditions or intracranial hemorrhage (n = 16) were excluded. After excluding these 68 patients, 118 patients were finally enrolled (Fig 2).

Flowchart of the study process.
The baseline, clinical, and imaging characteristics, and outcomes of the patients are shown in the Online Supplemental Data. On the basis of the Stop Stroke Study of the Trial of Org 10172 on Acute Stroke Treatment classification12 and the embolic stroke of undetermined source criteria,13 stroke subtypes were classified as cardioembolic stroke (n = 89), large-artery atherosclerosis (n = 15), embolic stroke of undetermined source (n = 12), and others (n = 2). The “others” classification included cases of ICA dissection. The occluded arteries included the ICA, M1, M2, and M3, and the number of patients with one of these arteries occluded was 27, 62, 28, and 1, respectively. On admission, 58 patients received tPA. The median ASPECTS-DWI was 8 (IQR, 7–9). The median stroke onset to imaging time was 119 minutes (IQR, 60–178 minutes), the imaging to recanalization time was 59 minutes (IQR, 40–82 minutes), and the stroke onset to recanalization time was 190 minutes (IQR, 112–270 minutes). In the initial MR image, the mean, maximum, and minimum median ADC levels were 515 (IQR, 459–578) × 10−6 mm2/s, 693 (IQR, 581–759) × 10−6 mm2/s, and 387 (IQR, 313–440) × 10−6 mm2/s, respectively. The second MR imaging was performed 23–27 hours after treatment. DWI reversal areas were observed in 42 (36%) of the 118 patients. Representative findings of DWI reversal assessed by MR imaging DWI/ADC are shown in Fig 1 and the Online Supplemental Data. All 118 patients had a DWI/FLAIR mismatch. All 42 patients with DWI reversal did not have FLAIR high intensity in DWI reversal areas at the second MR imaging, and 76 patients without DWI reversal had FLAIR high intensity in all initial DWI lesions at the second MR imaging. The median baseline, follow-up, and DWI reversal 11 minus ASPECTS-DWI scores were 3 (IQR, 2–5), 3 (IQR, 1–5), and 0 (IQR, 0–1), respectively. The recanalization states were classified as TICI 2b (n = 59) or TICI 3 (n = 59).
Regarding outcomes, 15 (13%) patients had parenchymal hemorrhage at the follow-up MR imaging. The median NIHSS score at 7 days was 4 (IQR, 2–12), and the median mRS at 3 months was 2 (IQR, 1–4).
There were no significant differences in vascular risk factors, stroke subtypes, occluded arteries, imaging to recanalization time, tPA treatment, ASPECTS-DWI, baseline 11 minus ASPECTS-DWI score, and recanalization state between the groups with and without DWI reversal areas. Patients with DWI reversal areas had significantly shorter times from onset to imaging and onset to recanalization than patients without DWI reversal areas (P = .049, .01). Additionally, patients with DWI reversal areas had significantly higher mean, maximum, and minimum ADC levels than those without DWI reversal areas (median: 575 [IQR, 539–621] versus 478 [IQR, 434–534], P < .0001; 747 [IQR, 695–798] versus 641 [IQR, 562–726], P < .0001; and 441 [IQR, 392–517] versus 346 [IQR, 294–411], P < .0001). Notably, 83% (35 of 42) of patients with DWI reversal areas had mean ADC values of ≥520 × 10−6 mm2/s, and 71% (54 of 76) without DWI reversal areas had mean ADC values of <520 × 10−6 mm2/s (Fig 3). Seventy-four percent (31 of 42) of patients with DWI reversal areas had maximum ADC values of ≥700 × 10−6 mm2/s, and 66% (50 of 76) of those without DWI reversal areas had ADC values of <700 × 10−6 mm2/s. Seventy-four percent (31 of 42) of patients with DWI reversal areas had minimum ADC values of ≥400 × 10−6 mm2/s, and 68% (52 of 76) of those without DWI reversal areas had mean ADC values of <400 × 10−6 mm2/s. To ascertain the threshold that had reversibility by MT, we performed a receiver operating characteristic analysis using the ADC values of reversal and nonreversal areas (Fig 3). The optimal mean, maximum, and minimum ADC thresholds for discriminating rev-ersibility from DWI lesions were 520 × 10−6 mm2/s, 700 × 10−6 mm2/s, and 400 × 10−6 mm2/s with sensitivities of 71%, 68%, and 68% and specificities of 83%, 74%, and 74%, respectively. The areas under the curve were 0.82, 0.75, and 0.78, respectively (Fig 3).

The ADC values of the initial DWI lesion (mean, maximum, minimum) according to the presence or absence of DWI reversal areas. Eighty-three percent (35 of 42) of patients with DWI reversal areas had mean ADC values of ≥520 × 10−6 mm2/s, and 71% (54 of 76) of patients without DWI reversal areas had ADC values of <520 × 10−6 mm2/s. Seventy-four percent (31 of 42) of patients with DWI reversal areas had maximum ADC values of ≥700 × 10−6 mm2/s, and 66% (50 of 76) of patients without DWI reversal areas had ADC values of <700 × 10−6 mm2/s. Seventy-four percent (31 of 42) of patients with DWI reversal areas had minimum ADC values of ≥400 × 10−6 mm2/s, and 68% (52 of 76) of patients without DWI reversal areas had ADC values of <400 × 10−6 mm2/s. The ADC values (mean, maximum, minimum) were significantly higher in patients with DWI reversal areas than in those without DWI reversal areas (P < .0001). The receiver operating characteristic curve for the collected data of this study (mean, maximum, minimum) shows that the ADC reflects areas that could be reversed by reperfusion therapy. The areas under the curves (mean, maximum, minimum) are 0.82, 0.75, and 0.78, respectively. The optimal mean, maximum, and minimum ADC thresholds for discriminating reversibility from DWI lesions are 520 × 10−6 mm2/s, 700 × 10−6 mm2/s, and 400 × 10−6 mm2/s with sensitivities of 71%, 68%, and 68% and specificities of 83%, 74%, and 74%, respectively.
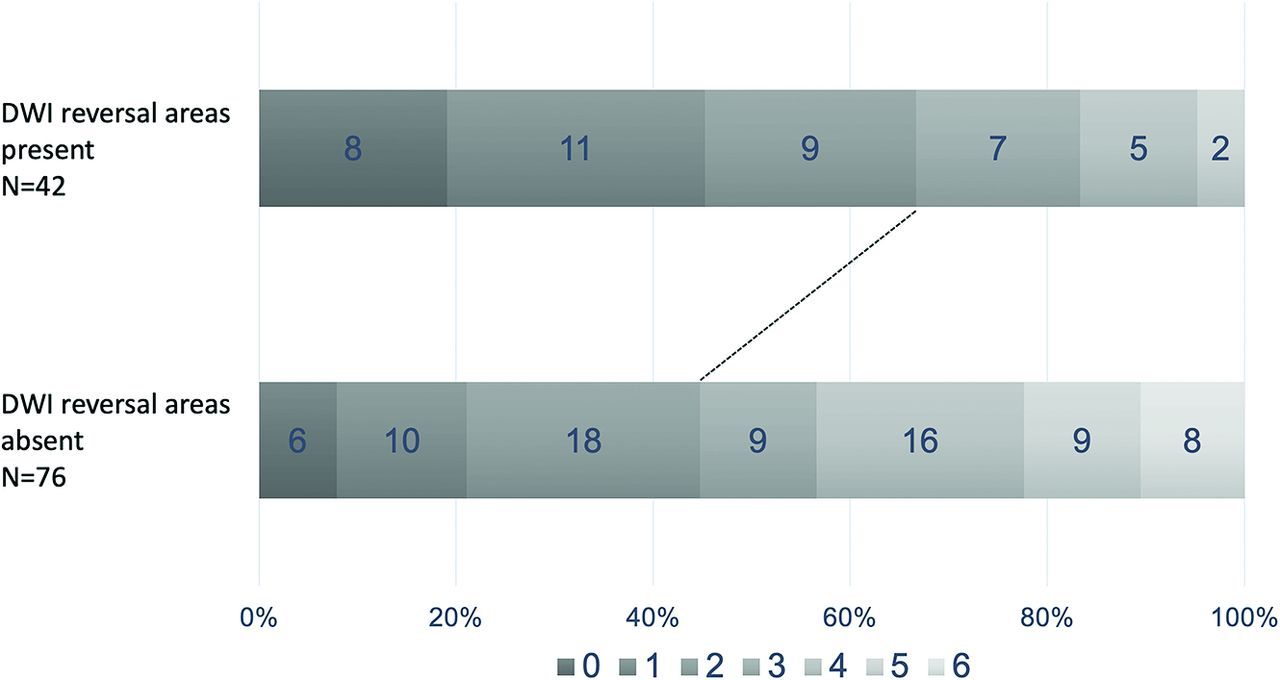
Patients with DWI reversal areas had significantly lower rates of parenchymal hemorrhage than patients without reversal areas (P = .002). The NIHSS score at 7 days and the mRS score at 3 months were significantly lower in patients with DWI reversal than in patients without reversal (P < .0001, P = .0009). Good functional outcome (mRS scores ≤ 0–2) after 3 months favored patients with DWI reversal areas (P = .011). The mRS distribution calculated at 3 months in patients with and without DWI reversal areas is shown in Fig 4.

mRS score 3 months after treatment. The rate of functional independence (mRS = 0–2) was significantly higher in patients with DWI reversal than in patients without DWI reversal (P = .011).
In 42 cases with DWI reversal, 22 cases had DWI lesions with and without DWI reversal. In these cases, the ADC values between DWI lesions with and without DWI reversal were compared in the same patients. There was no significant difference between mean and maximum ADC values, excluding minimum ADC values (Online Supplemental Data).
To identify factors associated with DWI reversal, we performed logistic regression analysis for factors (age, sex, initial NIHSS, ASPECTS-DWI, onset to image time, image to recanalization time, mean ADC, and recanalization state). In the multivariate analysis, mean ADC values (OR, 1.023; 95% CI, 1.013–1.033; P < .0001) were associated with DWI reversal (Online Supplemental Data). To identify factors associated with good functional outcomes (mRS 0–2), we performed logistic regression analysis for certain factors (age, sex, initial NIHSS score, ASPECTS-DWI, onset to image time, image to recanalization time, mean ADC, recanalization state, DWI reversal, and parenchymal hemorrhage). In the multivariate analysis, sex (men) (OR, 3.065; 95% CI, 1.081–8.690; P = .035), higher ASPECTS-DWI scores (OR, 2.527; 95% CI, 1.666–3.832; P < .0001), and recanalization states (TICI 3) (OR, 2.952; 95% CI, 1.074–8.113; P = .036) were associated with good functional outcomes (Online Supplemental Data).
DISCUSSION
This study suggests that the ADC value is independently associated with DWI reversal by reperfusion treatment and that DWI reversal results in early neurologic improvement (NIHSS score at 7 days) and a good prognosis (mRS at 3 months). In previous reports, the reversibility of DWI lesions by reperfusion therapy was unclear. Campbell et al14 reported that diffusion restriction could indicate irreversible ischemic damage, and Purushotham et al15 reported that the infarct core region showed an ADC of ≤620 × 10−6 mm2/s. In contrast, permanent DWI lesion reversal is well-established in animal studies using a temporary artery occlusion model.4,16 In patients treated within 4.5 hours of symptom onset, DWI reversal has often been confirmed and resulted in early neurologic improvement.5 The current study also supports the reversibility of DWI lesions by reperfusion therapy.
The reported prevalence of patients with DWI reversal varies widely among studies, ranging from 7% to 85%.14,17 In our study, 42/118 (36%) patients were found to have DWI reversal areas. Discrepancies in the rates of occurrence are likely explained by differences in the operational definition of DWI reversal, particularly in the timing of both acute and follow-up imaging. Our DWI reversal definition was based on follow-up MR imaging performed 23–27 hours after treatment, reflecting the treatment response. Accordingly, 24-hour DWI lesion volumes predict functional outcomes and late FLAIR of infarct volumes.14 Therefore, our study confirmed that angiographic recanalization (TICI ≥ 2b) and consequent DWI reversal are possible. Recently, Yoo et al18 reported DWI reversal after endovascular treatment in 15.5% of patients with stroke. However, in our study, the rate of DWI reversal was 36%. Two observations can explain this difference. First, the onset-to-recanalization time in the study of Yoo et al (mean DWI reversal: 369 [SD, 212], mean DWI increase: 417 [SD, 232]) was much longer than that in our study. Second, they included patients with TICI 1 or TICI 2a. Meanwhile, our study included only successful recanalization (>TICI 2b). These factors resulted in the high rate of DWI reversal.
Concerning the ADC threshold, Shinoda et al9 reported that a high relative ADC ratio, indicating the ratio of the ADC values of the affected territory to the ADC values of the contralateral normal brain regions, could result in DWI reversal, with an average relative ADC ratio of 0.890 (SD, 0.045) in reversible DWI lesions and 0.640 (SD, 0.041) in final infarct DWI lesions. Under these circumstances, a mean ADC of ≥520 × 10−6 mm2/s is suitable because the normal ADC level on the contralateral side was 650–750 × 10−6 mm2/s. In addition, our study considered maximum and minimum ADC values. Among these parameters, the mean ADC value (ADC threshold: 520 × 10−6 mm2/s) had the highest sensitivity and specificity (Fig 3). No significant differences were observed in the mean and maximum ADC values between lesions with and without reversal in the same cases (Online Supplemental Data). This finding might suggest that the degree of ADC decrease is the same in every DWI lesion. Multivariate analysis showed that the mean ADC value is independently associated with DWI reversal (P < .0001, Online Supplemental Data). The literature review suggests that early treatment and complete recanalization are associated with DWI reversal.5,18 However, the ADC value was not included. Therefore, we believe that the mean ADC value is the most important factor to predict DWI reversal, and placement of ROIs might be possible anywhere in DWI lesions.
Thomalla et al19 reported that in patients with acute stroke with an unknown time of onset, tPA treatment was effective for patients with a DWI/FLAIR mismatch. This phenomenon also partially reflects DWI reversal. In our study, all patients had DWI/FLAIR mismatch at the initial MR imaging. The ADC value is more accurate and sensitive for reflecting DWI reversal.
According to the literature, it is unknown whether DWI reversal areas retrieve neuronal function.6,20,21 In our study, the NIHSS score at 7 days in patients with DWI reversal was significantly lower than that in patients without DWI reversal (P < .0001), and there were no significant differences in the initial NIHSS and ASPECTS-DWI scores between patients with and without DWI reversal. These results suggest that patients with DWI lesions with reversal regain neurologic function.
Regarding outcomes, the mRS at 3 months was significa-ntly lower in patients with DWI reversal than in those without DWI reversal (P = .0009). This result suggests that patients with DWI reversal tend to improve. However, the factors associated with good functional outcomes (mRS, 0–2) were sex (men), a high ASPECTS-DWI score, and complete recanalization in logistic regression analysis (P = .035, P < .001, P = .036, respectively). Patients with a high ASPECTS-DWI score might have smaller infarct cores, and successful recanalization in such patients could cause complete improvement. Yoo et al18 also reported complete recanalization as an important factor for a good functional outcome. In a previous report,22 female sex and older age were predictive of cardiogenic embolism, and patients with high NIHSS scores have a poor prognosis in old age. These circumstances could result in male patients having a good functional outcome.
In this study, successful recanalization was an inclusion criterion. Moreover, we established this criterion to confirm recanalization at the DWI lesion and predict the effectiveness of this qualitative diagnosis. We believe that this new perspective could help ascertain the effectiveness of MT in cases with a low ASPECTS. Cases with low ASPECTS-DWI with mild ADC reduction improve with MT. In contrast, MT should not be performed in cases with low ASPECTS with severe ADC reduction. In our study, the rate of parenchymal hemorrhage of cases without DWI reversal was significantly higher than that of those with DWI reversal (Online Supplemental Data). Furthermore, 16 of the patients excluded due to lack of MR imaging with severe stroke or intracranial hemorrhage had severe ADC reduction at the initial MR imaging (mean of the median ADC values: 447 (IQR, 385–465) × 10−6 mm2/s). A recent article suggested that cases with a low ASPECTS could achieve good functional outcomes,23 and this might result from these patients having mild ADC reduction. Therefore, the ADC value is needed to decide on MT for cases with a low ASPECTS-DWI.
Therefore, we believe that DWI lesions are not infarct core. ADC mild reduction, especially a mean ADC of ≥520 × 10−6 mm2/s, is still viable and salvageable by MT. DWI reversal lesions could retrieve neurologic function. Because the ADC value is easily obtained, it could be a good predictor of the efficacy of reperfusion treatment.
This study had some limitations. First, the ADC values were obtained from circular ROIs that were placed manually on ADC maps. Therefore, they do not reflect all lesions with DWI reversal. Second, patients who did not undergo follow-up MR imaging because of severe stroke conditions or intracranial hemorrhage (n = 16) were excluded, and the ADC values of these patients decreased severely. Therefore, the prognosis of patients without DWI reversal might not be completely reflected. Third, the study sample was small. Last, this was a retrospective cohort study, and a prospective study is, therefore, necessary to confirm these results.
CONCLUSIONS
The ADC value is independently associated with DWI reversal. In the acute ischemic stage, DWI lesions with mild ADC reduction, especially those with a mean ADC value of ≥520 × 10−6 mm2/s, could be salvageable by MT, and patients with DWI reversal have early neurologic improvement (NIHSS score at 7 days). The ADC value is easily assessed and is a useful tool to predict viable lesions.
ACKNOWLEDGMENTS
We gratefully acknowledge the work of past and present members of our department.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received November 17, 2021.
- Accepted after revision March 17, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}