
Abstract
BACKGROUND AND PURPOSE: Recent advances in fetal MR imaging technology have enabled acquisition of diagnostic images in the early second trimester. Interpretation of these examinations is limited by a lack of familiarity with the developmental changes that occur during these early stages of growth. This study aimed to characterize normal fetal brain growth between the 12th and 20th weeks of gestational age.
MATERIALS AND METHODS: This study was conducted as an observational retrospective analysis. Data were obtained from a tertiary care center's PACS database. All fetuses included had late fetal MR imaging (>20 weeks) or postnatal MR imaging, which confirmed normality. Each MR image was manually segmented, with ROIs placed to calculate the volume of the supratentorial parenchyma, brainstem, cerebellum, ventricular CSF, and extra-axial CSF. A linear regression analysis was used to evaluate gestational age as a predictor of the volume of each structure.
RESULTS: Thirty-one subjects with a mean gestational age of 17.23 weeks (range, 12–19 weeks) were studied. There was a positive, significant association between gestational age and intracranial, supratentorial parenchyma; brainstem cerebellum; intraventricular CSF; and extra-axial CSF volumes (P < .001). Growth was fastest in the supratentorial parenchyma and extra-axial CSF. Fetal sex was not associated with the volume in any of the ROIs.
CONCLUSIONS: This study demonstrates distinct trajectories for the major compartments of the fetal brain in the early second trimester. The fastest growth rates were observed in the supratentorial brain and extra-axial CSF.
ABBREVIATION:
- GA
- gestational age
Extensive literature has demonstrated the usefulness of fetal MR imaging in assessing CNS abnormalities during the late second and third trimesters.1⇓⇓-4 Due to the small size of the fetus and the high prevalence of motion artifacts, imaging is generally deferred until after 20 weeks' gestational age (GA).5 However, advancements in MR imaging technology, including receiving coils and the use of 3T scanners now allow imaging with sufficient spatial and temporal resolution to acquire diagnostic images in the early second trimester.6⇓-8 This growing practice has highlighted the relative void of information regarding normal brain development in vivo in these early stages.
Evaluating brain growth and neurologic well-being in the early second trimester is of great interest to developmental neuroscience and fetal neurology. This period is characterized by the formation of the subplate, intense neuronal proliferation in the germinal centers, extensive neuronal migration, early synaptic sprouting, and axonal growth.9 In clinical practice, patients with pregnancies with fetal abdominal wall defects, chromosomal abnormalities detected on screening tests, major CNS abnormalities, and complications related to multiple pregnancies frequently seek diagnostic imaging and prognostication at earlier time points. Information obtained from early second-trimester fetal MR imaging can be tremendously useful in counseling these families.
The purpose of this study was to characterize normal fetal brain development in vivo between the 12th and 20th weeks of gestation by performing a retrospective analysis at a large tertiary maternal and fetal care center. We hypothesized that while all structures in the fetal brain will grow during this period, our volumetric analysis will demonstrate distinct trajectories for the major constituents of the fetal brain at these early GAs.
MATERIALS AND METHODS
The institutional review board (Boston Children's Hospital) approved this observational retrospective study. All data were obtained from the PACS database at a tertiary children's hospital. Inclusion criteria were as follows: 1) fetal MR imaging performed between January 1, 2014, and December 30, 2022, in a pregnancy with <20 weeks' GA, 2) non-neurologic indication for the examination, and 3) the availability of a high-quality (fully diagnostic), late fetal (>20 weeks' GA), or postnatal MR imaging confirming a structurally normal brain. Exclusion criteria included the following: 1) fetal abnormalities that may affect neurodevelopment (eg, syndromic diseases, congenital infections, multiple gestations, chromosomal abnormalities), 2) twin pregnancies, and 3) MR imaging examinations with insufficient quality for manual segmentations. At least 1 series covering the fetal brain had to be devoid of motion in every single section to be considered of sufficient quality.
Data Acquisition
All images were acquired on 3T scanners (Magnetom Skyra and Magnetom Vida; Siemens). Institutional protocols were followed for image acquisition, consisting of HASTE or balanced steady-state free precession images. The parameters of the HASTE sequences were the following: TR = 1400–4000 ms, TE = 100–102 ms, FOV = 230 × 230 or 256 × 256, 1-mm in-plane resolution, 2- to 2.5-mm section thickness, acquisition matrix size = 208 × 208 or 256 × 256. For the balanced steady-state free precession sequences parameters were the following: TR = 4.3–5.2 ms, TE = 1.8–2.6 ms, FOV = 230 × 230–300 × 300, 1-mm in-plane resolution, 2- to 2.5-mm section thickness, acquisition matrix size = 256 × 320.
Image Processing
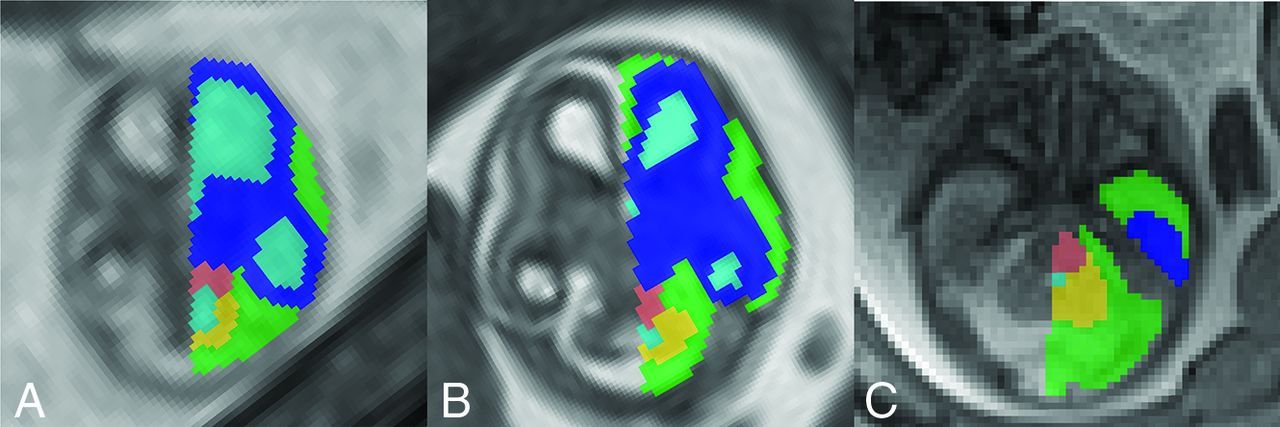
DICOM data of fetuses meeting the criteria were converted to the NIfTI format. Data were visualized and segmented using ITK-SNAP (Version 4.0.0; www.itksnap.org) (Fig 1). We performed manual segmentations, placing ROIs in the fetal supratentorial brain parenchyma (the portion of the brain above the tentorium cerebelli), brainstem, cerebellum, extra-axial CSF, and intraventricular CSF using a high-resolution (1080p) Wacom Cintiq Tablet (https://www.wacom.com/en-us/products/pen-displays/wacom-cintiq). Given that fetal MR imaging at such an early GA is prone to motion degradation and that either sequence provides sufficient tissue contrast to outline the desired anatomy, we chose the sequence with the highest SNR and lowest artifact degradation (shadowing, motion, banding). This choice was determined subjectively by an experienced neuroradiologist. We performed an intraobserver variability analysis for 4 randomly chosen fetuses; the second set of segmentations was completed >4 months after the original segmentation.

Representative example of ROIs in the brain of 12-week (A), 15-week (B), and 19-week-old fetuses (C). The supratentorial brain is labeled in dark blue; the ventricular CSF, in light blue; the extra-axial CSF, in green; the brainstem, in salmon; and the cerebellum, in yellow.
Statistical Analysis
The volume of each label was calculated for all subjects. Intracranial volume was calculated as the sum of all ROIs. A linear regression analysis was used to evaluate GA as a predictor of the volume of each structure. We also controlled for sex on the basis of previously reported findings on sexual dimorphism by Machado-Rivas et al.7 The relative volume of each structure was calculated as the ratio of the absolute volume of the structure to the intracranial volume. We performed an intraobserver reliability analysis for the manual segmentations by randomly choosing 4 fetuses, performing new volumetric segmentations, and estimating the percentage change of the results relative to the index segmentation. Descriptive statistics were used to summarize the data from relative volume estimations. All calculations were performed using R (Version 4.2.1; http://www.r-project.org/) with a significance level of .05. Plots were designed using the ggplot2 package (Version 3.4.0; https://www.rdocumentation.org/packages/ggplot2/versions/3.4.4).
RESULTS
Population
We retrieved a total of 270 early second-trimester fetal MRIs. The examinations of 51 subjects met the criteria for inclusion, and 20 of these were subsequently excluded due to low image quality that precluded accurate segmentations (Fig 2). The final sample consisted of 31 subjects (13 female) with a mean GA of 17.23 weeks (range, 12–19 weeks). For 26 subjects, the follow-up examination consisted of a second fetal MR imaging obtained at a mean age of 27.2 weeks (range, 21–36 weeks), and for 5 subjects, the follow-up consisted of a postnatal MR imaging obtained 8.2 months postdelivery (range, 1–24 months). The average interval between the index study and the follow-up study was 13.32 weeks (range, 3–57 weeks). Table 1 summarizes the indications for fetal MRIs.

Application of inclusion and exclusion criteria in a flow diagram.
Demographics and clinical characteristics
Volumetric Analysis
Intracranial Volume and Parenchyma.
There were significant positive associations between GA and intracranial volume, supratentorial parenchymal volume, brainstem volume, and cerebellar volume. Fetal sex was not significantly associated with the volume of any of the ROIs (P >.05). The Online Supplemental Data summarize the mean volume and weekly change of the individual structures across the study period. The Online Supplemental Data present the mean volume of the individual structures per week.
CSF Spaces.
We observed significant associations between GA and intraventricular CSF volume and extra-axial CSF. Fetal sex was not significantly associated with either ROI (P >.05, both). The Online Supplemental Data summarize the change in volume per week and present the mean volume per week.
The result of our intraobserver variability analysis showed high concordance between segmentations. The average percentage difference across all ROIs was 7.71%, and it was highest for the brainstem and intraventricular CSF ROIs. The highest concordance was found for the extra-axial CSF. The Online Supplemental Data summarize the data for this analysis.
Relative Volumetry
There was a significant GA-related increase in the relative volume of the supratentorial brain and extra-axial CSF (P < .02). Conversely, there was a significant decrease in the relative volume of the brainstem, cerebellum, and intraventricular CSF (P < .001) (Table 2). Figure 3 provides a graphical comparison of the absolute and relative growth of each structure per GA. Fetal sex was not significantly associated with relative volume growth (P >.05).

Absolute and relative volume growth per week. For each structure, absolute volume growth per week of GA (A) and relative volume growth per week (B) demonstrate relatively larger supratentorial growth during these early GAs.
Relative volume change per week based on linear regression analysesa
DISCUSSION
Advancements in MR imaging technology have expanded the clinical applications of fetal MR imaging, enabling the acquisition of diagnostic images in the early second trimester. This study aimed to address the scarcity of data on in vivo fetal brain development in pregnancies between the 12th and 20th weeks' GA by performing a retrospective analysis of brain growth in subjects whose subsequent neuroradiologic studies confirmed normality. Our results demonstrate rapid growth of all intracranial structures with distinct trajectories for individual regions. Awareness of normative and relative volumetry of structures can inform the interpretation of fetal MRIs and contribute to understanding the selective vulnerability and physiopathology of abnormalities that could arise at these early developmental stages.
Most MR imaging literature pertaining to fetal brain development in the early second trimester is based on ex vivo studies.10⇓⇓⇓-14 The absolute volumetric estimates for the cerebellum and total brain volume from our study align with those reported by Zhan et al10 and Xu et al.11 The analysis performed by Zhan et al used submillimeter acquisitions at 7T in conjunction with atlasing techniques. In addition to having similar growth trajectories, their approach enabled them to identify a clear anterior-to-posterior gradient in these developmental changes.10 Xu et al also used submillimeter acquisitions at 7T to study cerebellar growth, and while the trends they reported are consistent with our observations, their work delved deeper into the regional patterns of individual cerebellar lobules.11 Most important, our study is the only one that has addressed these challenges using in vivo MR imaging, demonstrating the feasibility of this approach and facilitating translation. Furthermore, the use of in vivo data minimizes the effects of biases related to tissue damage, swelling, and tissue preparation that are inherent in ex vivo analyses.15
The supratentorial brain was the dominant compartment, and it also displayed the highest growth rate. At 12 weeks, it constituted about one-third of the intracranial volume, which increased to nearly one-half by the 19 weeks. Active neuronal proliferation and migration, the formation of the subplate, and the rapid expansion of the latter likely drive this exuberant growth.16 As these processes halt or slow down, growth does the same, leading to a more modest growth rate reported later in pregnancy by Machado-Rivas et al.7 Despite moderately high rates of growth, the brainstem and cerebellum were outpaced by the supratentorial brain, which resulted in a slight decrease in their relative percentage of intracranial volume between the 12th and 19th weeks. At later GAs, the rate of growth of the supratentorial brain decreases and the cerebellum becomes the fastest-growing compartment.7,17
The ventricles constitute a dominant structure in early pregnancy, accounting for nearly one-quarter of intracranial volume at 12 weeks. Ventricular growth is slow, a finding previously corroborated by sonography and fetal MR imaging studies across a wide range of GAs.7,18 It is crucial to note that this slow growth results in a substantial decrease in the proportion of intracranial volume of the ventricles with advancing GA. The expansion of the extra-axial CSF emerged as another key finding in our analysis. Its growth rate was second only to that of the supratentorial parenchyma, reaching almost 40% of intracranial volume by 19 weeks' GA. The role of the extra-axial CSF as a marker of normal neurologic development is often underestimated. For instance, an increase in volume has been reported in cases of congenital heart disease, and a reduced volume is a hallmark of open neural tube defects.19,20
Fetal neuroimaging in pregnancies of <20 weeks' GA, though uncommon, is an area of increasing interest. The desire to counsel families as early as possible, monitor vulnerable pregnancies, and triage patients for a growing number of fetal interventions has fueled this trend. One relatively common indication in our cohort was the characterization of abdominal wall defects. While not the primary malformation, the neurologic well-being of these fetuses is a pivotal point in counseling because multiorgan system malformations necessitate specialized counseling, particularly in regard to the potential for genetic or syndromic etiologies. Monochorionic diamniotic twins represent another vulnerable population; these fetuses are at risk of unbalanced vascular and placental sharing (eg, twin-twin transfusion syndrome) and resultant complications, have a high risk of cerebrovascular events, and frequently are eligible for fetoscopic interventions.16,21 Last, sociopolitical factors, such as the evolving legal landscape surrounding pregnancy termination, could serve as an incentive to image fetuses at an earlier GA to provide prognostic information. The availability of normative volumetric data can enhance the interpretation of imaging findings in these early pregnancies.
The limitations of this study include its retrospective nature, which may introduce bias, and the relatively small sample size of 31 subjects. The exclusion of 20 subjects due to low image quality underscores the challenges of acquiring high-quality images during the early second trimester. The segmentations used for analysis were based on 2D images rather than 3D reconstructed volumes. Although previous work has pioneered the use of super-resolved 3D volumes for fetal images, these tools are not available for the GA range analyzed in this study. Consequently, the reported volumes of structures in the fetal brain might be underestimated or overestimated compared with a 3D volume estimation. Future studies with larger sample sizes, prospective designs, and improved image analysis pipelines may help refine and expand the normative data generated in this study.
CONCLUSIONS
This study provides essential normative data on fetal brain development in vivo between the 12th and 20th weeks of gestation. During this period, there is substantial absolute and relative growth in the brain parenchyma and extra-axial CSF volume relative to the intraventricular CSF, cerebellum, and brainstem. As the clinical footprint of fetal MR imaging continues to expand to the early second trimester, these data can aid in interpreting these examinations.
Footnotes
J.A. Estroff and C. Jaimes are co-senior authors.
This work was supported by the American Roentgen Ray Society Scholarship; Career Development Award from the Office of Faculty Development at Boston Children's Hospital; National Institute of Neurological Disorders and Stroke, grant/award Nos. R01EB031849, R01EB032366, R01HD109395, R01NS106030; National Institutes of Health Office of the Director, grant/award No. S10OD0250111; Rosamund Stone Zander Translational Neuroscience Center, Boston Children's Hospital; National Institute of Biomedical Imaging and Bioengineering; Eunice Kennedy Shriver National Institute of Child Health.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received July 6, 2023.
- Accepted after revision October 2, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}