
Abstract
BACKGROUND: Spontaneous intracranial hypotension is an important cause of treatable secondary headaches. Evidence on the efficacy of epidural blood patching and surgery for spontaneous intracranial hypotension has not been synthesized.
PURPOSE: Our aim was to identify evidence clusters and knowledge gaps in the efficacy of treatments for spontaneous intracranial hypotension to prioritize future research.
DATA SOURCES: We searched published English language articles on MEDLINE (Ovid), the Web of Science (Clarivate), and EMBASE (Elsevier) from inception until October 29, 2021.
STUDY SELECTION: We reviewed experimental, observational, and systematic review studies assessing the efficacy of epidural blood patching or surgery in spontaneous intracranial hypotension.
DATA ANALYSIS: One author performed data extraction, and a second verified it. Disagreements were resolved by consensus or adjudicated by a third author.
DATA SYNTHESIS: One hundred thirty-nine studies were included (median, 14 participants; range, 3–298 participants). Most articles were published in the past decade. Most assessed epidural blood patching outcomes. No studies met level 1 evidence. Most were retrospective cohort or case series (92.1%, n = 128). A few compared the efficacy of different treatments (10.8%, n = 15). Most used objective methods for the diagnosis of spontaneous intracranial hypotension (62.3%, n = 86); however, 37.7% (n = 52) did not clearly meet the International Classification of Headache Disorders-3 criteria. CSF leak type was unclear in 77.7% (n = 108). Nearly all reported patient symptoms using unvalidated measures (84.9%, n = 118). Outcomes were rarely collected at uniform prespecified time points.
LIMITATIONS: The investigation did not include transvenous embolization of CSF-to-venous fistulas.
CONCLUSIONS: Evidence gaps demonstrate a need for prospective study designs, clinical trials, and comparative studies. We recommend using the International Classification of Headache Disorders-3 diagnostic criteria, explicit reporting of CSF leak subtype, inclusion of key procedural details, and using objective validated outcome measures collected at uniform time points.
ABBREVIATIONS:
- EBP
- epidural blood patching
- ICHD-3
- International Classification of Headache Disorders-3
- QOL
- quality of life
- SIH
- spontaneous intracranial hypotension
Spontaneous intracranial hypotension (SIH) is a condition caused by a noniatrogenic spinal CSF leak that leads to considerable disability, typically in the form of an orthostatic headache (ie, improved with recumbency).1 Morbidity due to SIH is compounded by cranial nerve dysfunction, causing a variety of symptoms including diplopia, tinnitus, muffled hearing, and disequilibrium, among many others. SIH is now recognized as an important treatable cause of headache. During the past decade, increased awareness of this disorder has led to substantial growth in both patient diagnoses as well as research publications.
The treatment of SIH requires closure of the spinal CSF leak. The primary methods are via epidural blood patching (EBP) or surgical repair.2 Data on SIH treatment efficacy are limited. For example, reported responses to EBP range from 36%–90%.3⇓⇓⇓⇓⇓⇓-10 This wide range suggests that the true effect is not yet determined. Data for the efficacy of surgical repair are even more sparse. Furthermore, the efficacy of treatments may be impacted by leak subtypes (eg, disc osteophyte spur, nerve root diverticula, or CSF-venous fistula) or affected by differences in technical characteristics of the treatment (eg, EBP targeted to the leak site versus nontargeted). As a result, there is considerable uncertainty about the optimal treatment for any given patient, and there are currently neither consensus guideline recommendations nor widely accepted algorithms for management. This lack of consensus has resulted in a heterogeneity of treatment approaches.
Standardization of treatment algorithms for SIH will be best reached through the development of strong evidence supporting decision-making. Thus, future research should be directed toward specific-yet-unanswered questions regarding SIH treatment efficacy. Developing these questions requires a thorough understanding of the current state of the literature. Therefore, we aimed to systematically map the available evidence for the efficacy of SIH treatments. This review addressed 2 key objectives: first, to describe the published literature that evaluates the efficacy of epidural patching for treatment of patients with SIH, and second, to describe the published literature that evaluates the efficacy of surgery for treatment of patients with SIH. The results of this work will allow us to gain a better understanding of the landscape of existing research on these topics, including a systematic description of study characteristics; evidence clusters to guide subsequent systematic reviews and meta-analyses; and evidence gaps that may guide funding agencies and investigators toward prioritization of future research to fulfill unmet needs.
MATERIALS AND METHODS
This systematic review and evidence map adhered to Preferred Reporting Items for Systematic Reviews and Meta Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines.11 The protocol was published and registered a priori in Open Science Framework (OSF, 10.17605/OSF.IO/NWJU7; https://osf.io/) and has not been subject to amendments.12 All steps of this study were pilot-tested by the team before implementation.
Data Sources and Searches
The MEDLINE (Ovid), Web of Science (Clarivate), and EMBASE (Elsevier) databases were searched for published English language citations. The search was developed and conducted by a professional medical librarian in consultation with the author team and included a mix of database–specific subject headings and keywords representing SIH (including CSF leaks, low CSF volume headaches, low-pressure headaches, and hypoliquorrhoeic headaches) and terms related to EBP or surgical techniques for the treatment of SIH. Search hedges or database filters were used to remove publication types such as editorials, letters, case reports, comments, and animal-only studies as appropriate for each database. The searches were independently peer-reviewed by another librarian using a modified Peer Review of Electronic Search Strategies checklist.13 Complete reproducible search strategies for all databases are detailed in the Online Supplemental Data. The original searches were conducted on December 10, 2020; a search update was conducted on October 20, 2021, to identify newly published studies. The reference lists of key studies and all included systematic reviews were hand-searched to identify additional citations not previously captured.
Inclusion and Exclusion Criteria
We included experimental, observational, and systematic review studies that assessed the efficacy of EBP or surgery for the treatment of patients of any age or sex with a reported diagnosis of SIH.
We excluded studies of patients with cranial CSF leaks, iatrogenic spinal CSF leaks (eg, post-dural puncture or postoperative), those with headaches not secondary to SIH, and mixed populations of patients with and without SIH without subgroup analyses. Single case reports, small case series (<3 cases), clinical guidelines, narrative reviews, editorials, and protocols were excluded. There was no limitation on date of publication.
Study Selection
The titles and abstracts of all articles identified by electronic searches were screened independently by 2 authors for relevance. Articles included by either investigator by title and abstract review advanced to full-text screening where they were again independently dual-screened. Disagreements between authors during full-text screening were resolved by consensus or by a third investigator when consensus could not be reached. All results were tracked in Covidence (https://www.covidence.org/), a web-based data-synthesis software program, and duplicates were removed.14 EndNote reference management software (Clarivate) was used during drafting of the manuscript. Articles that met the criteria for inclusion underwent data extraction.
Data Extraction
One author abstracted data from each included study using a customized data-extraction form within Covidence. Abstracted data were then verified by a second author. Disagreements were resolved by consensus or adjudicated by a third author when consensus could not be reached. Extracted data elements included study design, study setting, number of patients included, patient demographics, method of SIH diagnosis, treatment-intervention characteristics (eg, type of EBP or surgery), outcome measures used, and timing of outcome assessment. Article authors were contacted for clarification or supplemental data when necessary.
Data Synthesis and Analysis
We tabulated included studies and summarized key study characteristics (eg, study design, patient demographics, details of treatment intervention) using tabular and graphic formats, including bubble plots to display evidence clusters and identify gaps. Areas of interest included the number of publications across time, clusters and gaps in study designs (such as a preponderance of retrospective designs or the absence of particular designs), patterns of both strengths and deficiencies in the reporting of diagnostic features (eg, International Classification of Headache Disorders-3 [ICHD-3] criteria, CSF leak subtypes), procedural details (eg, targeting EBP, patch material used), and measures of efficacy (eg, patient symptoms, quality of life, imaging biomarkers). Proportions were assessed by 2-tailed χ2 tests for significance. Two-tailed t tests were used to compare means. Linear regression was used to assess continuous variables such as the mean number of patients included per study across time. All statistical analyses were conducted using an open-source statistical analysis program (R statistical and computing software; Version 3.4.1; http://www.r-project.org). A P value < .05 was considered statistically significant.
Certainty of Evidence
A critical appraisal of the methodologic quality and risk of bias for individual studies as well as grading of the strength of evidence was not performed because this is an evidence mapping review.15
Role of Funding Source
This study was not supported by external funding sources.
Standard Protocol Approvals, Registrations, and Patient Consent
This Health Insurance Portability and Accountability Act-compliant study was deemed exempt from institutional review board oversight. The protocol for this study was registered with Open Science Framework on December 8, 2020.
Data Availability Statement
Anonymized data not published within this article will be made available by request from any qualified investigator.
RESULTS
The primary literature search identified 3608 studies. After duplicate articles were removed, a total of 2040 underwent title and abstract screening. Of these, 176 were moved on to full-text review, and a total of 139 were included in the evidence map (Fig 1 and Online Supplemental Data).

Evidence map or the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart. The asterisk indicates Martin 2019,26 Ohtonari 2012,27 Urbach 2020,28 Beck 2019,29 Pagani-Estevez 2019,30 Levi 2019,31 Franzini 2013,32 Watanabe 2011,33 Beck 2019,29 Angelo 2011;34 hash, Ferrante 2016,35 Ferrante 2015.36
Characteristics of Included Studies
Most included studies (66.2%, 92 of 139) were published in the past decade. The number of studies published per year has progressively increased, particularly during the past 5–10 years (Fig 2). Most studies assessed outcomes after EBP. Very few studies investigated surgical approaches alone. Articles were published by authors at institutions throughout the world, though the greatest number came from the United States, followed by South Korea and Japan (Fig 3). Most studies were generated from either dedicated SIH referral centers or universities. Studies that included surgery were more likely to come from referral centers (62.5%, 35 of 56) than those that included EBP (28.8%, 36 of 125), possibly due to the complexity of these operative procedures (P < .001). The number of patients per study has significantly increased with time (mean, 29.8 [SD 41.9] patients; range, 3–298 patients; P < .001). Characteristics of included studies can be found in the Online Supplemental Data.

Timeline of included publications.

Countries of origin for included studies.
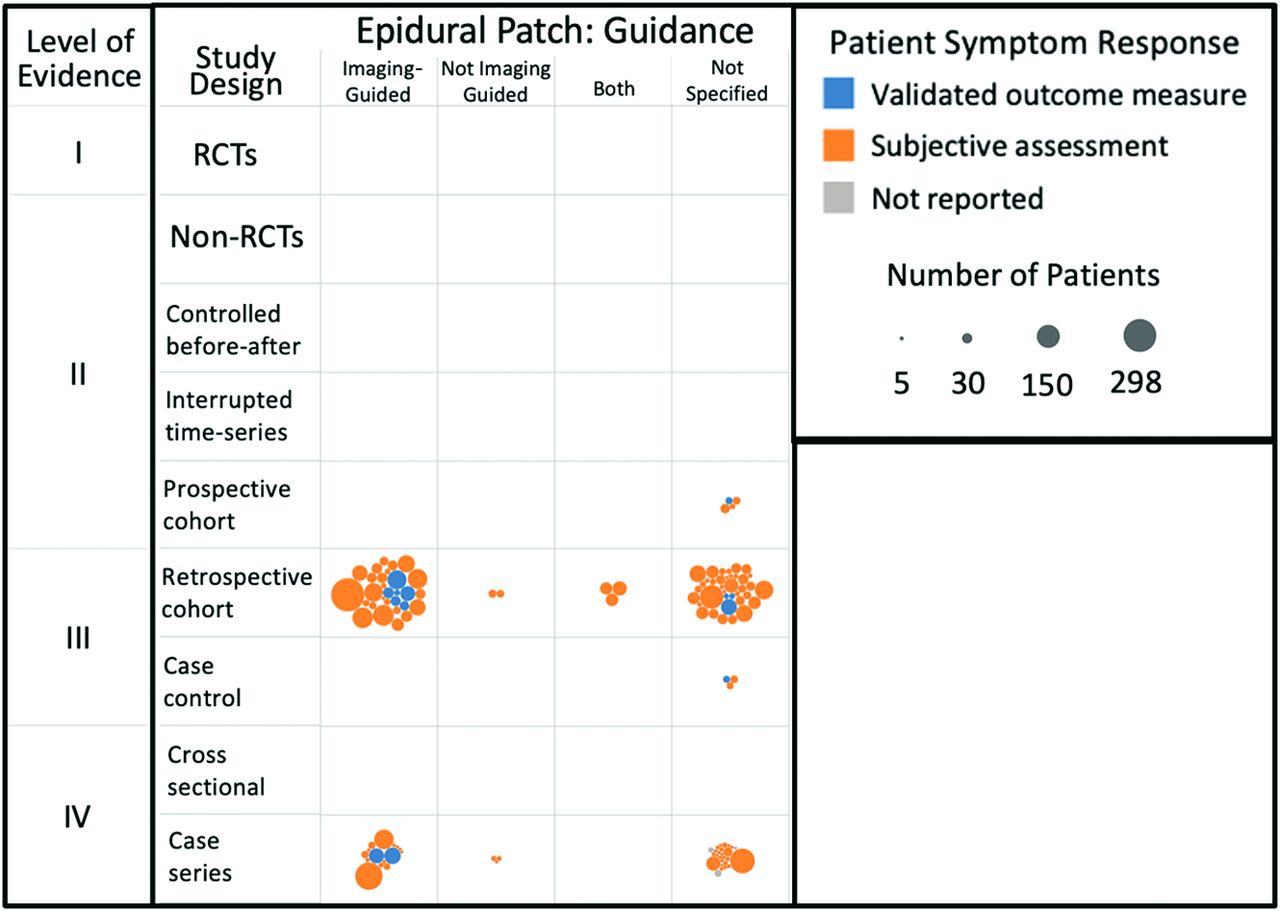
There were no studies that met level 1 evidence (ie, no randomized controlled trials). Most study designs were retrospective cohort studies (56.1%, 78 of 139) or case series (36%, 50 of 139), with only a few prospective cohort studies (3.6%, 5 of 139) (Figs 4–7). However, the evidence level of studies has slowly increased with time. For example, 52.8% of all published studies from 1996 to 2001 were case series, compared with 24.5% from 2017 to 2021. This interval reduction in the percentage of case studies reflects an increasing quality of study design. Furthermore, during the past 5 years, 67.8% of studies were a retrospective cohort design (increased from 30.6% in 1996–2001), and the first systematic reviews were published (3.8%, n = 3).

Evidence map of studies investigating treatments for SIH that included epidural patching and describing imaging-guidance methods. Note that each circle represents a single study with the area of the circle proportional to the study sample size; and colors represent the method of assessing a patient’s symptomatic response in each study, either a validated outcome measure (blue), subjective (nonvalidated) assessment (orange), or not reported (gray). RCT indicates randomized controlled trial.

Evidence map of studies investigating treatments in SIH that included epidural patching and described the patching material used. RCT indicates randomized controlled trial.

Evidence map of studies investigating treatments in SIH that included epidural patching and described targeted or nontargeted approaches. RCT indicates randomized controlled trial.

Evidence map of studies investigating treatments in SIH that included surgery. RCT indicates randomized controlled trial.
There were very few studies that included a comparison of 2 active treatments, and none were published before 2007. Of those published, most (66.7%, 10 of 15) were published only within the past 5 years.
The following subsections report results for the cohort of studies that included EBP and the cohort of studies that included surgery, as well as report key characteristics about included studies such as the methods of SIH diagnosis, the included CSF leak subtypes, and the outcome measures used to assess the efficacy of treatment.
Epidural Patching
Most studies (57.6%, 72 of 125) that investigated the efficacy of epidural patching did not specify whether imaging guidance was used to direct needle placement (Fig 4). Moreover, several of the studies reporting the use of imaging guidance did not specify the type of guidance (ie, fluoroscopy or CT).
Nearly one-quarter of the epidural patching studies did not specify the patching material used (22.4%, 28 of 125). Most studies that did report the patching material used autologous blood (56.8%, 71 of 125). Very few studies investigated the efficacy of procedures using fibrin glue alone (3.2%, 4 of 125) (Fig 5).
The largest proportion of studies on epidural patching (28.8%, 36 of 125) did not specify whether needle placements were targeted to a site of CSF leak or were nontargeted (Fig 6). When specified, more studies reported on procedures that were nontargeted (24.8%, 31 of 125) than targeted (19.2%, 24 of 125). Many studies reported a heterogeneous mixture of both targeted and nontargeted approaches (27.2%, 34 of 125), but nearly all of these studies did not include a comparison between these subgroups.
Surgery
There were fewer studies that investigated outcomes after surgical treatment of SIH than after epidural patching (n = 56 versus 125, respectively). Studies that assessed outcomes after surgical treatment of SIH had significantly smaller sample sizes (mean, 9.9 [SD 12.8] patients; range, 1–69 patients) compared with EBP (mean, 30.1 [SD 43.6] patients; range, 1–298 patients) (P < .001). More than half of investigations on surgical treatment included <10 patients.
Most surgical studies (66.1%, 37 of 56) either did not specify the surgical approach used or included a heterogeneous mixture of multiple surgical approaches, typically in the form of case series (Fig 7). The most commonly reported surgical techniques included intradural and extradural approaches to dural repair (some using fat-packing, muscle flaps, fibrin glue, or Gelfoam; Phadia), nerve root ligation or clipping, electrocautery of epidural veins for CSF-to-venous fistulas, and nerve root sleeve meningeal diverticulum repair.
SIH: Diagnosis
Greater than one-third of the included studies either did not specify the diagnosis method (13.8%, 19 of 138) or used a subjective criterion such as physician reporting of perceived patient improvement (23.9%, 33 of 138). The remainder of the included studies used an objective method to establish a patient diagnosis of SIH (62.3%, 86 of 138) (Fig 8A). The proportion of studies using objective diagnostic criteria was similar between studies investigating treatment with EBP and those investigating treatment with surgery.

Methods of SIH diagnosis and types of CSF leaks.
Greater than half of the included studies used diagnosis methods that satisfy current ICHD-3 criteria for a diagnosis of SIH (58.7%, 81 of 138). However, in a substantial number of studies, it was not possible to determine whether included patients satisfied the ICHD-3 criteria (37.7%, 52 of 138). In a small number of studies, reporting of methodologic details was sufficient to determine that the included patients did not meet ICHD-3 diagnostic criteria (3.6%, 5 of 138) (Fig 8B).16
Types of CSF Leaks
SIH is caused by 3 known types of spinal CSF leaks: nerve root sleeve diverticula, disc osteophyte spurs, and CSF-to-venous fistulas.1 Most studies provided insufficient detail to determine which type or types of CSF leaks were included in their investigations (Fig 8C). For example, 77.7% (108 of 139) of studies either did not report the type of CSF leaks included (56.8%, 79 of 139) or their reporting was unclear, making it impossible to tell what subtypes were included (20.9%, 29 of 139). Studies including surgical treatments were significantly more likely to report the specific subtypes of CSF leaks than studies investigating treatment with EBP (48.2%, 27 of 56 versus 17.6%, 22 of 125, P < .001).
Outcome Measures
Nearly all of the studies made use of subjective nonvalidated reporting of changes in patient symptoms to assess treatment efficacy (84.9%, 118 of 139). In fact, only 12.2% (17 of 139) used validated outcome measures, most commonly a Pain Numeric Rating Scale (Figs 4⇑⇑–7 and 9A).
There were almost no studies that included measures of quality of life (QOL). Only 1 study (0.7%) reported results from a validated QOL measure (modified Rankin scale), and 98.6% (137 of 139) did not report on QOL at all (Fig 9B). A single study subjectively reported QOL changes.

Outcome measures.
Posttreatment brain MR imaging and spine imaging are sometimes used as noninvasive biomarkers for successful resolution of SIH.17 Most of the included studies (61.2%, 85 of 139) did not report on posttreatment changes in imaging (Fig 9C). When a change was reported, it was typically in the form of a subjective interpretation of the imaging (eg, “imaging improved”), which was the case in 37.4% (52 of 139) of the studies. Only 2 studies (1.4%) used objective outcome measures such as the Bern score.18 Studies including surgery were more likely to obtain posttreatment imaging (53.6%, 30 of 56) than those including EBP (37.6%, 47 of 125) (P = .04) . However, these studies typically included only subjective assessments of the imaging.
There were very few studies that had predetermined and set postprocedural time points for the collection of outcome measures. Far more commonly, patient outcomes were collected at variable times after treatment. In 34.6% (47 of 136) of studies, the timing of outcome collection was not reported at all.
DISCUSSION
We identified and reviewed 139 studies that reported the efficacy of surgery and EBP, the 2 most common treatments for patients with SIH. We found no studies providing level 1 evidence for the efficacy of either treatment and identified no published clinical trials. Most published studies were retrospective, typically either case series or smaller cohort studies. In general, important study details were often missing, including methodologic details such as how a diagnosis of SIH was established and what specific subtypes of CSF leaks were being treated. Furthermore, procedural characteristics were often lacking, which made it difficult to determine important information such as whether imaging guidance or targeting was used in EBP or exactly what type of surgery was performed. Finally, patient-outcome assessment typically used subjective, nonvalidated measures collected at variable or unspecified time intervals.
The results of this evidence map suggest that the current efficacy estimates for EBP and surgery in SIH should be interpreted with caution. The incomplete description of patient characteristics in many of the included studies makes it difficult to understand how the study cohort compares with the broader SIH population, limiting applicability. For example, in some studies, the methods for establishing an SIH diagnosis were ambiguous, leading to uncertainty about the diagnosis itself. Additionally, we found that 77.7% of the studies did not adequately describe the subtypes of CSF leaks that were being treated. There may prove to be substantial differences in the treatment outcomes between patients with different subtypes of CSF leaks, which could skew the results of individual studies, possibly leading to spurious conclusions. Similarly, the absence of key procedural details in many instances makes it difficult, if not impossible, to understand the impact of certain decisions on the efficacy of treatments, such as whether to use a targeted approach or to include fibrin glue in EBP. Finally, the use of subjective, nonvalidated outcome measures without prespecified or uniform collection times leads to uncertainty about the usefulness of the collected data. Without establishing content validity, a chosen outcome measure may not truly capture the intended information of interest. For example, the use of outcome measures focused on patients’ pain may not accurately reflect the severity of disease if morbidity is due to cranial nerve dysfunction, fatigue, or cognitive dysfunction. Moreover, collecting outcomes at variable time points makes it challenging to compare cohorts of patients and could introduce bias (eg, outcomes only collected when the patient is symptomatic and returning to clinic).
To our knowledge, this represents the first systematic review to map the evidence for the efficacy of EBP and surgery in the treatment of SIH. We identified 3 previously published systematic reviews of SIH, but none of these mapped the current evidence to describe characteristics of the literature nor did they identify evidence clusters and knowledge gaps. Two also included meta-analyses.19,20 The article by D’Antona et al19 is a general review of SIH containing a small subsection on treatment, which provides some summary estimates about conservative approaches, EBP, and surgery. The study by Signorelli et al20 focused on factors affecting the outcome of EBP in SIH. Their review and analysis included only 6 articles, all retrospective. This small number was presumably due to the strict inclusion criteria used, such as the need for the studies to be comparative. This finding is in keeping with our findings that there are few prospective or comparative studies of EBP. Shlobin et al21 published a systematic review of patients with SIH with CSF-to-venous fistulas. The purpose of their review was to provide a comprehensive picture of CSF-to-venous fistulas, rather than to focus solely on treatment or map the evidence, as in the present study. They found 16 articles that met the inclusion criteria and performed a patient-level meta-analysis on 18 patients from 7 of these studies. Similarly, they found either only retrospective case series or cohort studies.
Given the considerable clinical and methodologic heterogeneity of the SIH literature, there was resultant statistical heterogeneity in many of the meta-analyses in these 2 studies, which raises some concern about the pooled estimates because they could lead to misleading conclusions. This heterogeneity is reflected in large I2 values (a measure of variation due to study heterogeneity rather than chance) for the meta-analyses, many >75% (considered high heterogeneity) and some in excess of 95%.19,20 In fact, very few published meta-analyses have I2 > 90%.22 Sources of heterogeneity are not identified, calling into question the value of the pooled estimates. In addition, many of the meta-analyses consisted of predominantly small studies. Although random effects analysis is appropriate, it can lend undue weight to smaller studies, skewing the estimated summary effect. Given the resultant uncertainty regarding the reported estimates, caution should be used before changing practice on the basis of these results.
The current study adds to these prior systematic reviews by providing clear descriptions of study design and methodology, including details about SIH diagnostic criteria, patient characteristics, procedure specifics, and the outcome measures used. Furthermore, this investigation maps the breadth of the literature rather than focusing on a narrow question in a small subset of studies. It, therefore, provides a better perspective to identify knowledge gaps and to suggest designs that might address these unmet needs. The results of this investigation reveal several evidence gaps and clear opportunities for methodologic improvement, which, when addressed through future research, will serve to improve the state of the literature and advance our knowledge about SIH treatment efficacy. First, the dearth of prospective studies and the absence of any level 1 evidence or clinical trials demonstrate a clear unmet need. Similarly, there are few comparative studies. Thus, future research should be directed toward designing comparative prospective studies beginning with cohort designs followed by randomized controlled trials, preferably with a multicenter approach to maximize patient enrollment and generalizability. These efforts may be best facilitated through development of a research infrastructure among a consortium of dedicated research institutions. Furthermore, there are very few studies investigating surgical treatments of SIH. Dedicated effort to determine the efficacy of SIH treatments other than EBP (ie, surgery and the newly developed venous embolization of CSF-venous fistulas) should be pursued.23 Second, future research should endeavor to reduce the potential for bias through adherence to sound methodologic practices and to improve interpretability through the clear reporting of key components of the study design. We recommend that objective SIH diagnostic criteria be used for patient inclusion, which should follow the current ICHD criteria at the time of the study (currently ICHD-3).16 Similarly, investigators should report the subtypes of spinal CSF leaks included in their cohort and whether there are efficacy differences among these subgroups of patients with SIH.
The following key procedural details should also be included at a minimum so that results may be better interpreted. For EBP, we strongly recommend including whether imaging guidance was used and the type (eg, CT fluoroscopy), whether the needles were targeted to the site of a known CSF leak or nontargeted, and the type of patch material used (eg, blood, fibrin glue, or both). For surgery, we recommend describing the operative approach or approaches in detail or providing references to previously described techniques. Critically, we recommend reporting symptom and disability outcome measures that are validated for use in SIH and that these measures be collected at prespecified uniform time points. To our knowledge, there are currently no validated outcome measures for use in SIH. Thus, effort should be directed toward validating existing measures or generating new ones. Until these efforts are completed, we recommend using objective measures validated for use in other headache disorders, such as the Headache Impact Test-6 and EuroQol-5D (https://euroqol.org/).24,25 Finally, the use of changes in imaging (eg, resolution of SIH findings on brain MR imaging) as an outcome measure should include either an objective scoring system or description.18
This study is a protocol-driven, methodologically rigorous evidence map. However, there are several potential limitations to this investigation. It is possible that our search inadvertently excluded studies that would have otherwise met the criteria for inclusion. This issue could have occurred due to the use of narrower search terms that included the “spontaneous” concept. However, we followed best practices for search development and reviewed a random sample of studies from the more expansive search to ensure that the probability of this exclusion was minimal, at best. Furthermore, we did not search the gray literature because this was deemed unlikely to have identified relevant studies and, therefore, did not warrant the substantial additional effort. This investigation did not include the few studies that reported the efficacy of transvenous embolization of CSF-to-venous fistulas because this newer treatment method was developed after the protocol for this review was established and there are so few publications on this promising new intervention to date. Additionally, the authors recognize that some of our recommendations are dependent on presumptions that are yet to be proved. For example, if nontargeted patching is equivalent in efficacy to targeted patching, then identifying the CSF leak subtype and localizing the leak with advanced myelography techniques may not be necessary. Finally, given that evidence mapping is a relatively new approach to critically appraising the literature, the standards are evolving. We followed current best practices, but these may be subject to change.
CONCLUSIONS
This systematic review and evidence map summarize the current state of the literature investigating the efficacy of EBP and surgery in the treatment of SIH based on 139 articles. Most studies were retrospective, and there was no published level 1 evidence. Identified gaps include the need for studies comparing the efficacy of different treatments as well as more sophisticated study designs such as prospective cohorts and randomized controlled trials. There remain many opportunities for the improvement in study methodology. We recommend that future research use the ICHD diagnostic criteria for SIH, explicitly report the specific subtypes of CSF leaks, include key procedural details such as whether EBP was imaging-guided and targeted and the type of patching material used or provide details about the surgical approach, and use objective outcome measures preferably validated for use in SIH and collected at uniform prespecified time points.
Acknowledgments
The authors would like to thank Reginald Lerebours from Duke University Medical Center for his assistance with the power analysis for the initial screening search and Eric Monson for his assistance in generating the figures for this article.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received February 23, 2023.
- Accepted after revision April 21, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Spinal CSF Leaks: The Neuroradiologist Transforming Care
- Perspectives from the Inaugural "Spinal CSF Leak: Bridging the Gap" Conference: A Convergence of Clinical and Patient Expertise
- Comment on: multidisciplinary consensus guideline for the diagnosis and management of spontaneous intracranial hypotension